Medical expert of the article

New publications
Right bundle branch blockade
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
If during the passage of electrical impulses along the cardiac conductive muscle fibers to the myocardium of the right ventricle, their delay occurs, the electrocardiogram shows such a pathological condition as right bundle branch blockade of the Hiss, which negatively affects the heart and blood circulation. [1]
Epidemiology
Right bundle branch block occurs in healthy people (up to 0.5-0.7% of people under 40 years of age), but its prevalence - due to changes in the conduction system of the heart - increases with age. According to some estimates, in 11.3% of the population aged 80 years ECG registers this pathological condition, and in cases of infarction - in almost 6% of patients (regardless of age).
Causes of the right bundle branch block
The heart is constantly contracting, and these contractions are regulated by the heart's conducting system, which is made up of conducting cardiomyocytes, the cells of the heart's conducting muscle fibers. The bundle of such fibers emanating from the atrioventricular or atrial-ventricular node (nodus atrioventricularis) of the right atrium is called the bundle of Hiss (fasciculus atrioventricularis). This atrial-ventricular muscle bundle has a common trunk, the branching part of which is divided into right and left legs.
The right pedicle is a long, thin structure composed of fast-acting Purkinje fibers; the distal section goes to the myocardium of the right ventricle and provides the conduction of electrical impulses (action potentials) that come from the sinoatrial (sinus) node, the pacemaker (pacesetter), and automatically cause the right atrium to contract and relax.
It should be borne in mind that the electrocardiogram of some healthy people shows this condition without any underlying cardiac disease. And the causes of right bundle branch blockade noted by cardiologists are associated with the presence of patients:
- Right ventricular hypertrophy or distension;
- Cardiomyopathy (diseases that affect the tissues of the heart muscle - myocardium);
- Coronary or coronary heart disease;
- Myocardial infarction;
- Postinfarction hemopericardium of the heart;
- Acute right ventricular failure;
- Heart defects, such as atrial septal defect and mitral valve stenosis;
- Rheumatoid heart disease, including myocarditis;
- Brugada syndrome;
- Kearns-Sayre syndrome;
- Idiopathic fibrosis and calcification (senile degeneration) of the conduction system of the heart - Leva disease or Lenegre-Leve syndrome;
- Pulmonary heart;
- Chronic lung disease with pulmonary hypertension;
- Pulmonary embolism.
Right bundle branch blockade in a child may result from
Arrhythmogenic right ventricular cardiomyopathy in children or heart surgery. Congenital right bundle branch block is seen on ECG in congenital heart defects such as primary atrial septal defect or tricuspid valve displacement toward the right ventricle (Ebstein's anomaly).
Also read - hiss bundle branch blockade: causes, symptoms, diagnosis, treatment
Risk factors
Elderly age, high blood pressure (systemic hypertension), and cardiac disease are considered risk factors for cardiac conduction system dysfunction in the form of Hiss bundle branch blockade (BBBB).
Often the risk is due to blunt trauma to the chest or a direct blow to the precardiac region, as well as prolonged compression of the chest wall causing compression of the heart between the spine and sternum.
Pathogenesis
Guis bundle branch blockades refer to intraventricular blockades, and experts attribute the pathogenesis of BPNPH, that is, the results seen on the electrocardiogram, to a change in the normal activation sequence in the Guis-Purkinje system.
The function of the Purkinje bundle cells of the right leg of the bundle of Hiss is to rapidly (1-3 m/s) conduct action potentials generated by the sinus node.
In norm, the initial activation of conducting cardiomyocytes occurs near the apex of the endocardium of the right ventricle, where the right pedicle runs down the right side of the interventricular septum; it then spreads to the septum, followed by the right pedicle in the middle third of the muscular part, and further by its branches, which go to the free wall of the right ventricle. And only after that the electrical impulses spread to the myocardial cells.
The blockade results from abnormalities in this pathway of impulse conduction, with the right ventricle not being directly activated by impulses passing through the bundle of Purkinje fibers of the right pedicle, resulting in slow and uncoordinated depolarization of the right ventricle - due to intercellular conduction that extends from the interventricular septum and left ventricle.
Symptoms of the right bundle branch block
Far from always right bundle branch block causes symptoms, but due to the delay in the flow of electrical impulses into the right ventricle, the heart rhythm may change, affecting blood pressure, resulting in dizziness, weakness, pre-syncope and fainting.
In the presence of various diseases with this cardiac conduction disorder, the clinical picture may include pressure and a feeling of heaviness in the chest, shortness of breath, heart pain, arrhythmia and increased heart rate - tachycardia.
More information in the material - heart rhythm and conduction disorders: symptoms and diagnosis
Depending on the degree of conduction disturbance, a distinction is made between incomplete blockade of the right bundle branch of the Hiss - if impulses pass with difficulty and slow (for example, as in combined mitral malformation) - and complete blockade of the right bundle branch of the Hiss, when impulses do not pass.
Transient or transient right bundle branch block may occur in chest trauma with myocardial contusion, after right heart catheterization, pulmonary balloon dilation, and repair of mitral valve and atrial septal defects.
In normal heart rhythm driver electrical signal travels along both legs of the Gis bundle, and intermittent or intermittent right bundle branch blockade is defined when impulses are not conducted simultaneously to the left leg of the Gis bundle, as manifested by an irregular heartbeat.
And blockade of the right and left legs of the bundle of Hiss means complete blockage of conduction of electrical signals from the upper chambers of the heart to the lower ones, i.e. From the atria to the ventricles.
Complications and consequences
What is the danger of right bundle branch block? In the absence of cardiac diseases and symptoms in patients, such blockade is often clinically insignificant and practically does not threaten anything.
However, if etiologically related diseases and pathologies are present and if there is a marked symptomatology, the effects and complications of BPNPH may manifest:
- Acute or chronic heart failure;
- With intravascular clots;
- Ventricular fibrillation;
- Progression to atrioventricular block (AV block);
- Asystole with cardiac arrest.
Diagnostics of the right bundle branch block
When examining the heart after auscultation, instrumental diagnostics is used: ECG - electrocardiography, transthoracic Doppler echocardiography, coronarography (coronary angiography).
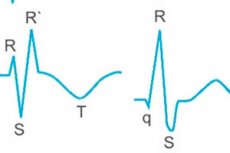
Right bundle branch block on ECG shows right-sided deviation of the electrical axis of the heart, widening of the QRS complex (QRS wave duration from 110 to 120 m/s). The QRS complex often shows an additional deviation reflecting rapid depolarization of the left ventricle. The blockade affects the terminal phase of ventricular depolarization, causing a broad R (increased amplitude) in the right thoracic leads, a broad S in the left thoracic leads (waveform 1A-B), and a deviation of the T plaque in the direction opposite to the terminal deviation of the QRS complex. All these signs are due to delayed depolarization of the right ventricle.
Read more: eCG Analysis and Decoding
To identify the cause of this cardiac conduction disorder, tests are taken, including a general blood count and lipidemic index, for troponin levels (cTn I and cTn II); AST, ALT, and amylase enzymes; and for rheumatoid factor.
The differential diagnosis is also aimed at finding out the etiology of the blockage.
Who to contact?
Treatment of the right bundle branch block
In cases where there is no cardiac or pulmonary disease or symptoms, BPNPH does not need to be treated.
Treatment will depend on the specific symptoms and conditions and may include:
- Hypotensive medications - high blood pressure pills;
- Antiarrhythmic drugs;
- Antiplatelet agents (Aspirin, Clopidogrel) and thrombolytics (Urokinase, Alteplase);
- Drugs to prevent and correct heart failure;
- Sedatives (valerian tablets, valocordine ).
Pacemaker placement may be considered if there is a history of Hiss bundle branch block and syncope.
Prevention
Right bundle branch blockade observed on ECG can not be prevented, but for the prevention of cardiac and pulmonary diseases it is recommended to adhere to a healthy lifestyle and the principles of a balanced diet.
Forecast
For each patient, if right bundle branch block is detected, the prognosis depends on the presence of cardiovascular disease. If there is none, this cardiac conduction disorder does not affect life expectancy. Although, the possibility of BPNDH to progress with involvement of other conduction branches should be taken into account.
Are army and sports compatible with right bundle branch blockade? In complete blockade, many sports are contraindicated, as well as compulsory military service, but in incomplete asymptomatic blockade there are no such restrictions.