Medical expert of the article

New publications
Hypoplasia of the left vertebral artery
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Disorder of cerebral circulation, manifested by symptoms of vertebrobasilar deficit, may result from such a disorder as hypoplasia of the left vertebral artery. It is a congenital anomaly, which consists in the underdevelopment of vertebral arterial vessels - members of the arterial system - the so-called villous circle, supplying blood to brain structures. In this pathology, the vascular lumen is narrowed in the area where the vessel passes into the bone canal, which causes a disorder of blood supply to the brain. [1]
Epidemiology
Hypoplasia of the left vertebral artery means narrowing of its internal diameter to less than 2 mm. Although there is no universally accepted indicator: some experts consider a decrease in diameter of less than 3 mm as a sign of hypoplasia, although this occurs in at least 6% of healthy patients.
Measurements of the diametric size are standardly performed in the V2 segment, the most convenient part of the vertebral artery, which gives a minimum of measurement errors.
It is noted that the most intensive development of vertebral arteries occurs in children in the periods of 5-7 and 7-9 years of age. The diameter of these vessels is approximately stable until the age of five - from 1.1 to 2 mm.
In medicine, vertebral artery hypoplasia is considered as one of the signs of undifferentiated connective tissue dysplasia. There are no data on the frequency of pathology in patients with genetic connective tissue disorders.
During magnetic resonance angiography with contrast, hypoplasia of the right and left vertebral artery was identified in approximately 3% of people, and unilateral hypoplasia was identified in more than 30% of people.
In ultrasound duplex scanning of vertebral arteries, left hypoplasia was diagnosed in 8% of cases.
The problem is more often experienced by women than men (67% vs. 33%). The disorder is found predominantly at the age of over 30 years.
Causes of the hypoplasia of the left vertebral artery
The vertebral arteries branch off from the subclavian arteries, joining together in the skull box. They supply blood to all brain structures, delivering nutrients and oxygen to the tissues.
The most intensive development of these arterial vessels occurs at the age of 6-9 years. Just at this stage it is possible to influence the factors that prevent the adequate course of this process. A certain role can be played by:
- Genetic features of the structure of the circulatory system;
- Connective tissue pathologies, inflammatory diseases;
- Unfavorable environmental factors.
When the internal diameter of the left vertebral artery narrows to two millimeters, it is said about the development of hypoplasia of the vessel, which becomes insufficiently passable. Often, pathological vascular curvatures are additionally detected, leading to hemodynamic disorders, impaired cerebral productivity. [2]
Risk factors
The main risk factor is intrauterine disorders, which in turn can be caused by:
- Abdominal (uterine) trauma;
- Bad habits of the future mother, intoxication during pregnancy;
- Infectious diseases during pregnancy;
- By radioactive exposure;
- Genetic predisposition, etc.
A healthy lifestyle reduces the risks of hypoplasia of the left vertebral artery, but does not eliminate them completely: the leading role is played by individual characteristics of the body and heredity. [3]
Pathogenesis
The vertebral arteries run from the subclavian arteries, joining the basilar arterial vessel after diverging into the posterior inferior cerebellar arteries. These branches act as the main blood supply to cerebral structures, including the midbrain, cerebellum, medulla oblongata, and pontine.
In general, the term hypoplasia refers to the underdevelopment of an organ - in this case, we are talking about the left vertebral artery.
The disorder forms at the stage of intrauterine development. Among the possible developmental pathways:
- Improper primary germ cell laying;
- Obstructed fetal positioning;
- Amniotic fluid deficiency;
- Toxic effects on the fetus during intrauterine development (due to smoking, alcoholic beverages or narcotic substances use by the future mother, etc.);
- Infectious exposures to the fetus during the intrauterine development stage;
- Physical tissue damage;
- The effects of irradiating radiation, excessive temperatures and other stressful physical factors;
- Metabolic disorders.
Hypoplasia of the sections of the left vertebral artery provokes the appearance of disorders from the organs that it supplies with blood. [4]
Symptoms of the hypoplasia of the left vertebral artery
The immediate factors that determine the clinical symptomatology in hypoplasia of the left vertebral artery are increased blood pressure and cerebral circulation deficit, as well as functional disorder of the cerebellum. The degree and breadth of the clinical picture directly depend on the degree of narrowing (underdevelopment) of the vessel.
Among the main and most common symptoms are:
- Regular dizziness, fainting;
- Constant or frequent pain in the back of the head, parietal region;
- Sensation of numbness in hands and/or feet, weakness of limbs;
- Trembling fingers, hands;
- Spikes in blood pressure readings;
- Coordination disorders, vestibular disorders;
- Impaired performance, unstable emotional background.
Some patients complain of generalized weakness, tinnitus or ringing in the ears, deterioration of hearing function, shortness of breath, increased fatigue.
The clinical picture does not manifest itself immediately, but the steady tendency to gradual progression and periodicity of manifestations draws attention.
In some cases, the pathology manifests itself abruptly, without any previous abnormality: the patient develops an acute cerebral circulation disorder or other brain tissue lesions. [5], [6]
Hypoplasia of the left vertebral artery in a child
Vertebral artery hypoplasia is diagnosed in about 3% of children under 17 years of age: a reduced vessel diameter of 2 to 1.5 mm with compensatory dilatation of the vertebral artery on the opposite side is found.
In children, there is a decrease in the blood flow in the narrowed artery below the age norm, as well as an increase in the outflow velocity through the vertebral venous network on the side of the affected vessel. Vertebral insufficiency, deformations of other vessels (in particular, internal carotid arteries), other anomalies (atrial septal defects, open interatrial communications, etc.) may be diagnosed.
Some children complain of periodic dizziness, headaches, fainting, but most often the problem is asymptomatic and detected accidentally. It can be combined with heart defects.
Hypoplasia detected in childhood may be a consequence of hereditary variant of connective tissue lesions, or the impact of negative factors in the intrauterine period, leading to impaired formation of a framework of connective tissue in the vessel wall.
Stages
Depending on the degree of deficiency of arterial blood supply to the affected area, such stages of circulatory disorder are distinguished:
- Functional compensation.
- Subcompensatory stage.
- Decompensation stage.
The probability of pathology transition to one or another stage directly depends on the quality and timeliness of diagnosis of hypoplasia.
At the stage of functional compensation, it is important to ensure regular dynamic monitoring with the use of imaging techniques.
Forms
When making a diagnosis, the localization of the affected arterial segment is taken into account. Thus, the following segments of the vertebral artery are distinguished:
- Anteroposterior division (V1);
- Cervical (V2);
- Atlantean (V3);
- Intracranial (V4).
The first three localizations of the pathology are hypoplasia of the extracranial section of the left vertebral artery when it has an extracranial location.
Hypoplasia of the intracranial segment of the left vertebral artery is located in the cranial cavity. Another name for this disorder is hypoplasia of the v4 segment of the left vertebral artery. These concepts are diagnostically equivalent.
Before the right and left vertebral arteries form the basilar artery, they branch downward and medially to form the anterior spinal arterial trunk. Hypoplasia of the left posterior vertebral artery may run from the posterior inferior cerebellar artery.
Complications and consequences
Brain structures against the background of hypoplasia of the left vertebral artery will try to adapt to the unilateral disruption of blood supply. Adaptation is carried out at the expense of another, normally developed right vertebral artery. Thus, oxygen supply to the vital stem centers is compensated, their protection from oxygen deficiency is activated. However, this adaptation mechanism can be disturbed - for example, over the years due to atherosclerotic vascular changes, as a result of dystrophic degenerative pathologies of the spinal column, head and skull traumas, and so on. As a result, the first signs of the pathological process are detected in a person:
- Impaired consciousness;
- Vestibular disorders (especially in the morning hours);
- Vision problems (mainly when turning the head).
Many patients complain of severe constant occipital headaches, with irradiation to the eyes, face. There is noise in the head, ringing in the ears. The clinical picture gradually worsens. Chronic oxygen deficiency adversely affects the general well-being, anxiety, phobias, delusions appear, the quality of life falls.
With hypoplasia of the left vertebral artery, blood flow in the entire vertebrobasilar system is impaired. The brain experiences high hemodynamic loads, which entails an increased risk of stroke - an acute circulatory disorder of the brain. Additional risks occur if hypoplasia is combined with cerebral form of atherosclerosis. [7]
Diagnostics of the hypoplasia of the left vertebral artery
Assessment of clinical symptoms, neurologic examination, and palpation of the left vertebral artery points in the suboccipital region between the transverse processes of the I and II cervical vertebrae are mandatory procedures as part of the preliminary diagnosis.
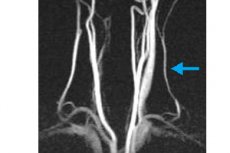
During an ultrasound examination of the vascular network, the doctor may suspect arterial hypoplasia. To clarify important points, the doctor may additionally prescribe magnetic resonance angiography - a widespread and informative diagnostic method, which, unlike CT scanning, has no irradiating effect on tissues.
Magnetic resonance angiography helps to thoroughly examine the condition of the vessels, detect narrowing and assess its degree. The specialist has the opportunity to use a three-dimensional image with good detail, which allows to view the vertebral artery along its entire length, to determine the locations of curvatures, changes in diameter, the degree of patency, compensatory capabilities, etc.
Tests include general blood and urine tests, blood chemistry (lipidogram with cholesterol, tiglycerides, HDL and LDL values), and enzyme-linked immunosorbent assays (ELISA).
Instrumental diagnostics can be extended by radiography of the cervical spine with functional tests, as well as spiral computed tomography of the brain and cervical spine. On individual indications, duplex scanning of the brachiocephalic arteries with functional tests with turning, extending and bending the head, as well as duplex scanning of the cervical veins may be prescribed. [8]
Oto-neurologic diagnosis is anchored by computerized examinations that provide insight into the status of brain stem structures.
The quality of the vestibular-coordinator apparatus is checked by performing stabilometry.
Differential diagnosis
Hypoplasia of the left vertebral artery is often asymptomatic if the other vessels are not damaged and perform their function normally. In such a situation, the quality of blood flow is compensated by the other vertebral artery and large carotid arteries.
If compensation is disturbed and insufficient, and patients are found to have a specific symptomatology, it is necessary to realize that it is nonspecific and can be caused by a variety of other pathologies. In particular, it is necessary to exclude:
- Atherosclerosis;
- MS;
- Tumor processes;
- Other vascular disorders.
The diagnosis should include a neurologist, oncologist, hematologist, ophthalmologist, otorhinolaryngologist, if indicated - doctors of other specialties.
Who to contact?
Treatment of the hypoplasia of the left vertebral artery
Disruption of blood flow in the left vertebral artery is accompanied by neurological symptoms and impaired venous outflow. This can, in turn, cause the development of congestion, so treatment begins with therapy that facilitates blood circulation, improves the adaptation of brain structures, eliminates the associated inflammatory and edematous processes.
Major medications that optimize venous outflow:
- Detralex, Flebodia (Diosmin semi-synthetic) 600-1200 mg per day;
- Troxerutin 600-900 mg per day;
- Medications, ginkgo biloba supplements;
- L-lysine escinate 100-200 mg per day.
Nonsteroidal anti-inflammatory drugs (for pain and inflammation):
- Nimesil 100-200 mg per day;
- Lornoxicam 8-16 mg per day.
Hemodynamic disorders in arterial hypoplasia are detected in almost all patients. And not only vertebrobasilar vessels, but also the carotid basin network are affected.
To improve blood flow in the vertebral artery is prescribed:
- Purine derivatives (Pentoxifylline 300-900 mg daily);
- Periwinkle preparations (Vincamine 60 mg daily, vinpocetine 15-30 mg daily);
- Cinnarizine 75-150 mg daily, Nimodipine 240 mg daily;
- α-adrenoblockers (Nicergoline 30-60 mg daily).
Mandatorily connect neuroprotectors, which is especially relevant for patients with a high risk of acute cerebral circulatory disorders, suffering from transient ischemic attacks, drop attacks. The most effective use of:
- Citicoline, which improves metabolism and blood circulation in the brain;
- Actovegin, which optimizes microcirculatory and trophic processes, increasing the adaptation of brain tissue to oxygen deficiency.
Additionally, cholinergic agents such as Ceretone (800 mg daily) or Citicoline (500 mg daily) may be prescribed, as well:
- Cerebrolysin 10-50 ml per day;
- Piracetam 1200 or 2400 mg per day;
- Mildronate 500 mg per day;
- Trimetazidine 60 mg per day.
As part of symptomatic treatment, myorelaxants (Tizanidine), antispasmodics (No-shpa), antimigraine drugs (Sumatriptan), and B-group vitamins are used.
The effectiveness of therapy is enhanced if additionally apply such procedures as massage of the collar region, acupuncture, apparatus effects, therapeutic exercise. [9]
Surgical treatment
Many patients with decompensated blood supply to brain structures require surgery. This can be a complex microsurgical intervention of arterial bypass surgery or balloon angioplasty or stenting.
A bypass intervention is performed to redirect blood flow to bypass the segment with hypoplasia. The anastomosis is formed from parts of the patient's own vessels.
The operation is performed using general anesthesia and lasts several hours. Contact Doppler diagnostics of the involved vessels is performed to check the quality of the anastomosis before the intervention is completed. After the operation, control Dopplerography and magnetic resonance imaging are repeatedly performed.
Balloon angioplasty is a dilation of the vascular lumen with a special balloon inserted by a catheter through a puncture in a peripheral arterial vessel. The process is monitored by a doctor using fluoroscopy.
In order to create a stable adequate arterial lumen, angioplasty can be combined with a stenting procedure. A special intravascular mesh construction is used.
For surgical treatment of arterial hypoplasia, modern neuroendoscopic and microsurgical equipment, radiological imaging methods, neuronavigation devices and intraoperative control over the functionality of the nervous system are used.
Prevention
Hypoplasia of the left vertebral artery is a defect that forms in the intrauterine period. It can be associated with genetics, environmental, toxic or infectious factors.
The occurrence of this disorder can be prevented if a woman is properly prepared for pregnancy, will timely visit doctors and treat emerging diseases, immunized in advance, eat rationally, take a doctor-recommended complex vitamin and mineral preparations, folic acid, iodine, etc.
During pregnancy, the future mother should not allow contact with harmful substances (heavy metals, nitrates, etc.), do not take any medications without prior consultation with a doctor, do not drink alcohol and do not smoke.
Even before conceiving a child, the couple should lead a healthy lifestyle. After the onset of pregnancy, a woman should timely register with a gynecologist, make a routine ultrasound.
Nutrition while carrying a baby should be balanced, so that the fetus receives enough vitamins and micronutrients for the proper development of organs.
Forecast
Left vertebral artery hypoplasia itself does not pose an immediate threat to life, but it significantly impairs the quality of life.
After carrying out the necessary diagnostic measures, patients are prescribed complex treatment to improve blood supply to the brain and normalize blood circulation. However, such drugs must be taken almost constantly, so patients often experience certain side effects: increased heart rate, increased sweating, shortness of breath, sleep disturbances, etc. To reduce the likelihood of side symptoms, treatment is prescribed in courses, with the minimum possible breaks and replacement of groups of drugs (if necessary).
With the development of a critical situation - for example, if hypoplasia of the left vertebral artery can be complicated by acute cerebral circulatory failure - the patient is prescribed surgical treatment (angioplasty) to ensure full blood flow through the narrowed vessel.
Hypoplasia of the left vertebral artery and the army
Hypoplasia of the left vertebral artery is often detected incidentally, for example, during routine diagnostics. Since the disorder is undetectable for quite a long time, pathological narrowing of the artery at a young age can be perceived as normal.
If the conscript has neurological symptoms indicative of impaired cerebral circulation, additional diagnostics and treatment may be required. Thus, suspicion is aroused by such symptoms as:
- Regular headaches and dizziness;
- Regular blackouts;
- Changes in limb sensitivity;
- Blood pressure fluctuations.
In complex cases, it is possible to detect chronic cerebral circulatory disorders as well as dyscirculatory encephalopathy.
Practitioners note that at a young age, such complications are rare, so asymptomatic or moderate hypoplasia of the left vertebral artery in the vast majority of cases does not become a hindrance to military service. Recognition as restricted or unfit for military service is possible if serious dysfunctions and complications are detected.