Medical expert of the article

New publications
S-scoliosis
Last reviewed: 12.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
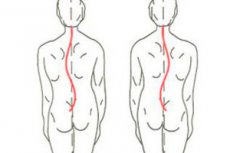
Any scoliosis is a deformation of the spine, and S-shaped scoliosis is defined when, along with the frontal curvature, resembling the letter C, there is a second lateral curvature - compensating, giving the spinal column the shape of the letter S.
This type of deforming dorsopathy in most cases affects the thoracolumbar region of the spinal column - the thoracic and lumbar regions. According to ICD-10, the scoliosis code is M41.0 M41.9.
Epidemiology
WHO statistics on scoliosis (2012-2014) indicate the seriousness of this pathology on a global scale: curvature of the spine has been diagnosed in 28 million patients, and 93% of them are children aged 10-16 years.
And experts from the National Scoliosis Foundation (USA) predict that this figure will increase to 36 million by 2050.
Today, it is possible to determine the cause of curvature in approximately 20% of scoliosis cases. About 10% of patients have adolescent idiopathic S-shaped scoliosis, and its prevalence is up to 3% of the population. At the same time, 90% of cases concern teenage girls.
The prevalence of congenital scoliosis in children is estimated at 1-4%.
Causes S-scoliosis
As vertebrologists note, S-shaped scoliosis in children and adolescents occurs during the period of the most active growth of the spine - at the age of 7-15 years, and is four times more often observed in girls (who grow faster during this period). If a C-shaped thoracic scoliosis is formed in the thoracic spine, then when the lumbar spine is involved in the pathological process, two oppositely directed arcs are formed, and S-shaped scoliosis develops.
Among the explanations for the etiology of this form of spinal curvature, the following most probable causes are named:
- genetic predisposition (although specific genes have not yet been identified);
- pathologies of skeletal ontogenesis – anomalies of its formation during the period of intrauterine development (between the 6th and 8th weeks of pregnancy), leading to congenital defects, for example, spina bifida;
- spinal cord injuries sustained during childbirth or in early childhood;
- poor posture in children;
- neuromuscular conditions accompanying various types of muscular dystrophy, torsion dystonia, as well as cerebral palsy and poliomyelitis;
- short leg syndrome;
- multiple hereditary osteochondromas (osseous-cartilaginous exostoses) of the spine;
- osteochondrosis of the lumbosacral spine (in adults);
- systemic rheumatic pathologies – lupus erythematosus, rheumatoid arthritis, polyarthritis, accompanied by inflammation of the connective tissue (fascia);
- juvenile (adolescent) ankylosing spondylitis or Bechterew's disease;
The so-called syndromic scoliosis is also noted, including S-shaped scoliosis, which is part of the clinical picture of a number of congenital syndromes with problems of the musculoskeletal system, in particular, Angelman syndrome, Down, Prader-Willi, Ehlers-Danlos, hereditary osteosclerosis (Albers-Schonberg disease), etc.
Idiopathic S-shaped scoliosis, which is considered the most commonly diagnosed type of spinal curvature in adolescents aged 10 to 17 years, develops spontaneously in most cases – without identifiable causes. There are many theories regarding the etiology of this disease, including hormonal imbalance, asymmetry of bone growth and muscle imbalance. About 30% of patients have a family history of scoliosis, which is considered indirect confirmation of possible genetic predispositions.
Read also – Scoliosis: what causes it and how to recognize it?
Risk factors
Among the risk factors for the development of scoliosis, experts note:
- prepubertal age and the associated accelerated growth of children, whose skeleton is in the process of development before the completion of puberty and is considered immature;
- female gender;
- the presence of deforming dorsopathies among close relatives;
- imbalance of loads on the spinal column and weakening of the joints;
- vertebral injuries;
- development of osteoporosis in adults and spondyloarthrosis in the elderly;
- the presence of myofascial pain syndrome (forcing one to seek a body position and posture to reduce pain).
There are also a number of factors that can increase the risk of abnormalities in the formation of the somites of the chord and neural tube of the fetus during pregnancy - with the development of congenital anomalies of the fetus and congenital scoliosis in the infant. This may include fetal hypoxia, placental insufficiency, gestational diabetes, the use of antiepileptic drugs or steroids, prolonged febrile fevers of pregnancy, the impact of toxic and radioactive substances on their body.
Pathogenesis
A healthy spine, when viewed from the side, has natural anatomical curves: forward – in the neck and lumbar region (lordosis) and backward – in the thoracic and sacral region (kyphosis). When viewed from behind, the spinal column runs strictly vertically in the middle of the back.
However, with scoliosis, the vertical position of the spine is disrupted, and the pathogenesis of its curvature - not fully studied to date - is seen in the asymmetric growth of the vertebrae. Based on the well-known anatomical and biomechanical features of the spine, specialists have studied the mechanisms of vertebral growth, which, while children grow, lengthen and become more voluminous.
But the growth of the vertebral bodies in front in relation to the dorsal (back) part is uneven. Thus, a decrease in dorsal growth prevents the growth of the ventrally located (lower) vertebral bodies with an increase in their height, causing torsion - twisting around the internal posterior longitudinal ligament towards the concave side with the formation of rotational lordosis and disruption of normal thoracic kyphosis.
Ossification nuclei gradually form on the surfaces of the vertebral joints, and their cartilaginous matrix is filled with bone tissue, fixing the defect.
In addition, with frontal displacement of the vertebral bodies, their “jamming” is revealed due to deformation of the intervertebral spaces; anomalies of bone growth plates (growth zones), dystrophy and degenerative changes in cartilage are noted; decreased bone mineral density.
Numerous clinical studies in adolescent patients with idiopathic S-shaped scoliosis have revealed abnormalities in the biomechanics of the spine, correlated with fibrosis of the paraspinal muscles that support the spine and its rotational movements.
And, perhaps, not the least important role in the pathogenesis of adolescent idiopathic S-shaped scoliosis is played by the deficiency of the hormone melatonin produced in the pineal gland, which stimulates the proliferation and differentiation of young bone tissue cells (osteoblasts).
Symptoms S-scoliosis
It is easy to miss the first signs of S-shaped curvature of the spine: at first (while the angle of curvature is no more than 5°) there are no symptoms, except in cases of congenital syndromic scoliosis. In infants, symptoms may include a bulge on one side of the chest, a protruding shoulder blade, the child may lie bent to one side.
In adolescents, the most common symptoms of S-shaped scoliosis include:
- slight deviation of the head (relative to the central position);
- asymmetry of the ribs (which protrude forward);
- changes in the horizontal position of the waist line;
- increasing the height of one shoulder and/or scapula compared to the opposite side;
- pain localized in the back, chest and lower limbs.
Lumbar S-shaped scoliosis can cause one hip to appear higher than the other with a sensation of shortening of one leg, which leads to the development of a habit of leaning on one side when standing - with excessive stretching of the intercostal muscles (on the side contralateral to the curvature) and weakening of the abdominal muscles.
The fourth degree of curvature often leads to the formation of a rib hump and back pain. Read more - Scoliosis as a factor in the development of back pain.
 [ 11 ]
[ 11 ]
Stages
The severity of the disease is determined by the degree of curvature of the spine - depending on the angle of rotation of the spinal column, visualized on an X-ray and defined as the Cobb angle. There are four such degrees:
- if the magnitude of the curvature angle does not exceed 10°, this is degree 1;
- more than 10° but less than 25° – 2nd degree;
- in the range of 25-50° – 3rd degree;
- more than 50° – 4th degree.
[ 12 ]
Forms
Types or kinds of S-shaped curvature of the spine are distinguished depending on the location:
- S-shaped scoliosis of the cervical and cervicothoracic spine with curvature in the cervical spine (with the apex at the TIII-TIV vertebrae);
- S-shaped thoracic scoliosis or thoracic, which is observed in the thoracic spine (peak in the middle of the back - vertebrae TVIII-TIX, curvature is limited to vertebrae TI-TXII) and is usually diagnosed in children or adolescents;
- S-shaped thoracolumbar scoliosis or thoracolumbar – affects both the lower thoracic and upper lumbar vertebrae (apical vertebrae TXI-TXII). Often, this curvature is congenital, forming in the womb during the sixth to eighth week of gestation and detectable at birth. It may be a secondary effect of a neuromuscular condition (such as spina bifida or cerebral palsy);
- S-shaped scoliosis of the lumbar spine (lumbar) - more common in adults (the apex is noted below the vertebrae TXII-LI).
When the curvature of the spine is directed to the left, S-shaped left-sided scoliosis is diagnosed, and if to the right, right-sided S-shaped scoliosis.
There is also congenital S-shaped scoliosis in children, neuromuscular and degenerative scoliosis in adults.
Complications and consequences
If scoliosis is left untreated, the spine will continue to deform and problems may develop over time.
According to observations, mild S-type scoliosis (up to 10°) progresses in 22% of patients. When the curvature angle is determined at a level of up to 20° and higher, the risk of progression increases to 65-68%. According to foreign orthopedists, in 36% of cases of idiopathic scoliosis in adolescents, the curvature increased after 20-22 years by more than 10°.
Degenerative S-shaped scoliosis in adults over 45 years old can develop towards an increase in the angle of curvature by 0.3° per year, and in people over 65 years old – by 2-2.5° annually. But the highest risk of progression is in adolescent idiopathic S-shaped thoracic scoliosis – 58-100%.
Complications and consequences of this type of spinal deformity include chronic pain in the back, chest, legs; problems with the heart and lungs, a significant decrease in physical endurance and activity. Also, the curvature of the spine can cause damage to the spinal cord, the consequences of which lead to paralysis of the lower limbs (paraplegia) and disability.
In women, 3-4 degrees of S-shaped scoliosis limits their ability to bear and give birth to a child. And young people with a curvature of more than 10-15° are not called up for military service.
[ 13 ]
Diagnostics S-scoliosis
To establish an individual therapeutic strategy, diagnostics requires a thorough clinical and visual examination with anthropometry. See - Visual criteria for statics and dynamics of the musculoskeletal system
To determine the condition of the vertebral joints, instrumental diagnostics are used:
- radiography with spondylometry;
- computed tomography of the spine (CT);
- MRI of the thoracic and lumbar spine;
- electromyography (EMG).
Differential diagnosis
Based on the examination results, differential diagnosis may also reveal other back problems, such as decreased motor activity, myasthenia or spasticity, indicating damage to the upper motor neurons, as well as myelomeningocele and syringomyelia, which have some similarities, associated with spinal cord alteration.
See more details - Some diseases accompanied by deformation of the spine.
Who to contact?
Treatment S-scoliosis
The main goal of scoliosis treatment is to try to prevent further curvature of the spine. Conservative treatment of idiopathic S-shaped scoliosis with a curvature angle of less than 40° consists of observation, special exercises and spinal bracing.
Congenital scoliosis, which has the worst prognosis, requires treatment from the first days of a child's life. As experience shows, only a quarter of cases can be managed without fixation, and 75% of cases require surgical intervention, which is carried out between the ages of one and four years.
To correct lateral curvature in some children, traction therapy - longitudinal stretching of the spine using special equipment - can be used.
In addition, surgical treatment by spondylodesis (fixation of vertebrae with metal rods, screws, hooks) is considered a necessary option in cases of unsuccessful attempts to stop further curvature of the spine or in cases of severe deformation. All details in the material - Scoliosis: surgery
Most adult patients (at the age of bone maturity) with idiopathic S-shaped scoliosis – with a curvature of less than 20° and not exceeding 40° – do not require surgical intervention or fixation, but they need physical therapy and exercise therapy (at least one and a half hours daily), as well as periodic examinations by the attending orthopedic surgeon or vertebrologist – with visualization of the spine using X-rays.
When the curvature in adolescents progresses (with a Cobb angle between 20-30°), fixation with brackets ("vertebral braces") is used to reduce the rate of the pathological process and to correct the deformation transversely. There are different types of orthopedic brackets, they are selected individually and used for a certain number of hours per day.
In order to stabilize the spine, reduce the load on the deformed vertebral bodies and restrain further curvature, a redressing (compensatory) corset or thoracolumbosacral orthosis is used.
More details – Treatment of scoliosis.
Physiotherapy treatment
In case of spinal column deformations, physiotherapy plays a key role. Currently, exercise therapy for S-shaped scoliosis is based on three-dimensional scoliosis therapy and special gymnastics developed by Katharina Schroth and the recommendations of the International Society for Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT). Depending on the degree of curvature and its localization, an individual exercise program is developed for each patient, and the physiotherapist must have the appropriate qualifications and sufficient clinical experience in scoliosis correction.
Exercises for S-shaped scoliosis - isometric and isotonic - are aimed at slowing down, stopping and correcting the curvature, as well as preventing muscle hypotrophy. And this is achieved by stabilizing muscle tension and activating paravertebral muscles, developing the skill of postural self-control and special breathing exercises.
Asymmetrical exercises for S-shaped scoliosis that strengthen the spinal muscles have a significant positive effect, including side planks and stretches, as well as some yoga asanas (apanasana, adha pavanmuktasana, jathara, vakrasana, trikonasana, parigahasana). A set of such exercises helps to: strengthen the back muscles and weak lateral muscles on the side where the ribs are convex; stretch the dense (spasmodic and hyperactive) lateral muscles on the concave side; increase the mobility and strength of the rectus femoris and quadriceps; strengthen the abdominal muscles and expand the chest.
Read:
Since the curvatures lead to musculoskeletal imbalance, therapeutic massage is recommended for S-shaped scoliosis. Massage courses help to distribute the load on the back muscles more correctly and maintain the musculoskeletal functions of the spine, and can also help reduce the displacement of the vertebrae.
In the treatment of this disease, electrical stimulation of muscles (electromyostimulation) of the lateral surface of the body is used.
Prevention
Most cases of S-shaped scoliosis are idiopathic, which means that prevention of spinal curvature consists of correct posture, sufficient physical activity (swimming is especially useful), proper nutrition, and mandatory monitoring of the condition of the spine, especially in the presence of risk factors for the development of this dorsopathy.
[ 19 ]
Forecast
For children with scoliosis, the prognosis varies depending on its severity, age, and overall health. Mild idiopathic S-shaped scoliosis in older children and adolescents is corrected with therapeutic exercise.
Congenital syndromes, neuromuscular and autoimmune conditions may be incurable, and spinal deformity often leads to disability.