Medical expert of the article

New publications
Uterine adenocarcinoma
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Uterine adenocarcinoma is one of the types of malignant tumors of the uterus. This cancer is characterized by the fact that it primarily affects the most superficial layer, the endometrium of the uterus.
Clinical manifestations of endometrial cancer occur in the form of bleeding, which as the disease progresses is supplemented by pain symptoms in the lower abdomen. There may be a tendency to either increase or decrease the size of the uterus. The development of pathological processes in most cases directly affects the body of the uterus.
Causes uterine adenocarcinoma
The exact causes of uterine cancer (like many other forms of cancer) are unknown. Some studies suggest that the risk of developing uterine cancer increases with:
Just as it is currently impossible to say with complete certainty exactly what actually causes cancer in its various forms, the causes of uterine adenocarcinoma can only be reduced to a list of factors that can provoke or contribute to the development of this malignant disease.
The age range in which there is the greatest probability of the formation of such a tumor covers the period in a woman’s life from 50 to 65 years.
As the results of some studies show, women in particular are at risk when they have a metabolic disorder and are overweight, with obesity. Especially with obesity of 2-3 degrees, with a significant excess of the body mass index.
There is a high risk of developing uterine adenocarcinoma in women who have never given birth.
The risk of this disease increases with late onset of menopause, if a woman's menopause occurs at the age of over 52 years.
Causes of uterine adenocarcinoma also include the presence of polycystic ovary syndrome in a woman.
The possibility of developing this malignant tumor is increased by a woman’s history of breast cancer, and in addition, if she is directly related to someone who has had uterine cancer – her mother or sister.
Symptoms uterine adenocarcinoma
The neoplasm has the appearance of a tumor node, the growth process of which occurs according to the exophytic type, with the possibility of subsequent spread to the myometrium. But, as a rule, such a tendency occurs in exceptional cases, mainly the tumor has a certain specific localization, does not expand the affected area to the endometrium over its entire surface, and does not penetrate the myometrium and parametrium.
Symptoms of uterine adenocarcinoma at the stage preceding its occurrence are manifested as the following precancerous and background diseases affecting the endometrium.
An endometrial polyp is characterized by the appearance of a limited thickening on the inner lining of the uterus, extending like an outgrowth into the uterine cavity.
Another harbinger of a malignant neoplasm beginning in the uterus may be a significantly increased number of endometrial glands, which is known as endometrial adenomatosis.
Precancerous conditions or the onset of cancer are indicated by such phenomena as the presence of prolonged aching pain symptoms in the lumbar region; prolonged bleeding with a large degree of blood loss during the menstrual cycle in women of reproductive age; bleeding in the uterus, which can be provoked during the onset of menopause, such as the resumption of bleeding after a long period of time.
A simple and effective preventive measure can be regular visits to a gynecologist. The specialist is able to competently identify the symptoms of uterine adenocarcinoma and prescribe timely appropriate treatment, preventing the transition of the disease to a more serious phase and the possible emergence of all sorts of complications.
Adenocarcinoma of the cervix
Cervical cancer is a malignant disease that in most cases develops in the flat epithelial cells that make up the inner lining of the cervix. Much less likely is adenocarcinoma of the cervix, which originates in mucus-producing cells.
A cancerous neoplasm localized in the cervix can be either exophytic or endophytic. In the first case, the direction of tumor growth is directed inside the vagina, and for the other, the expansion of the affected areas is characteristic due to deepening into the cervical canal, towards the body of the uterus.
It should also be noted that there is a third type – papillary cervical cancer. In this type, the tumor is formed by a collection of something similar to small papillae, similar in appearance to Brussels sprouts.
Cervical adenocarcinoma is diagnosed by a method that consists of detecting the presence of cancer cells in smears taken from the cervix, or, on the contrary, stating their absence. This diagnostic method is called the Pap test or Papanicolaou test. Cervical cancers can often be asymptomatic, which makes timely diagnosis and treatment especially important.
Adenocarcinoma of the uterine body
Adenocarcinoma of the uterine body is a malignant neoplasm that originates from the tissues of the muscular or mucous membrane of the uterus.
Based on the fact that the endometrium exhibits significant sensitivity to the effects of sex hormones, in particular, estrogen, this oncology is a hormone-dependent cancer disease.
In approximately half of the cases, the tumor is localized in the area of the fundus of the uterus; less commonly, the isthmus may be affected, or the entire uterine cavity may be affected.
As the disease progresses, pathological cells tend to expand the affected area by spreading to neighboring cells. The cervix, ovaries with fallopian tubes, and tissues surrounding the uterus, as well as lymph nodes and lymphatic transport pathways to all other organs, may be involved in the processes of metastasis.
Adenocarcinoma of the uterine body is most often detected in women of premenopausal age. It is diagnosed by scraping the cervical canal for subsequent histological examination. An unfavorable factor complicating diagnosis is its location in deep tissue layers.
Where does it hurt?
Stages
The following stages of uterine adenocarcinoma are distinguished:
- At the first stage of this cancer, the tumor from the uterine mucosa spreads to the uterine wall. The probability of stopping further pathological progress and preventing complications with timely diagnosis and treatment is very high and equals approximately 87%.
- The second stage is characterized by the inclusion of the cervix in the area of damage by this oncology. At the same time, the surrounding organs remain unaffected. The prognosis for successful treatment is favorable, and the chance of recovery is 76%.
- At the third stage of uterine adenocarcinoma, the adjacent internal organs are affected by the disease, and the lymph nodes are also involved in the affected area. The probability of recovery at this stage, compared to the previous ones, decreases to 63%.
- The peculiarities of the fourth stage are that cancer, in addition to spreading to nearby organs, is accompanied by the appearance of metastases. The possibility of recovery is designated as a probability of 37%.
Depending on the stage, one or another conservative or radical treatment method is appropriate, such as surgery to remove the tumor, radiation therapy, etc.
Forms
Well differentiated adenocarcinoma of the uterus
Highly differentiated adenocarcinoma of the uterus is one of the types of malignant neoplasms belonging to the group of cancers that can develop in the epithelium of glandular tissues. The criteria for distinguishing between these types are determined by the degree of their cellular differentiation.
In this case, there is a minimal degree of polymorphism. This means that the affected cells of a particular tissue differ from healthy ones in the most insignificant way.
Of the obvious symptoms and manifestations that characterize highly differentiated adenocarcinoma of the uterus, it can only be noted that in its presence, the nuclei of cells that have undergone pathological degeneration increase in size and become somewhat more elongated. Based on this, differential diagnostics and establishing an accurate appropriate diagnosis in this case presents certain difficulties.
In this form of uterine adenocarcinoma, its superficial spread into the myometrium occurs. The risk of significant complications and the appearance of lymphogenous metastases when it is localized within the mucous membrane in this area of the uterus is minimal. The probability is no more than 1%.
 [ 21 ], [ 22 ], [ 23 ], [ 24 ]
[ 21 ], [ 22 ], [ 23 ], [ 24 ]
Moderately differentiated adenocarcinoma of the uterus
Moderately differentiated adenocarcinoma of the uterus is characterized by a high level of polymorphism of cells that have undergone changes caused by this oncological disease in the uterus, its muscle tissue or mucous membrane.
The mechanism of action of this uterine oncology is largely similar to the development and course of highly differentiated adenocarcinoma. The significant difference in this case is that a significantly larger number of cells are involved in pathological phenomena, with which active processes of mitosis and cell division occur.
Thus, moderately differentiated adenocarcinoma of the uterus is characterized by a higher degree of severity. It is more likely to lead to the development of all sorts of complications and pathologies in case of untimely diagnosis and treatment.
The way of spreading cancerous neoplasm is mainly together with the lymph flow in the lymph nodes of the small pelvis. Metastasis of lymphatic origin in moderately differentiated adenocarcinoma of the uterus occurs in 9% of female patients.
In young women under 30 years of age, the presence of metastases is not detected in the vast majority of cases.
Poorly differentiated adenocarcinoma of the uterus
Poorly differentiated adenocarcinoma of the uterus is the third histopathological stage of uterine cancer. The tumor is a collection of cells formed as bands or masses of irregular shape. Intracellular mucin is observed in only one case out of two.
In some individual cases, there may be oxyphilic, light, glycogen-rich, or lipid-rich, foamy contents of the cellular cytoplasm.
One of the characteristic features that distinguishes low-differentiated adenocarcinoma of the uterus is the manifestation of pronounced cellular polymorphism. In this type of cancer of the uterus, there is obvious malignancy, which is expressed in the formation of tissues that have undergone pathological changes.
The prognosis in this case appears to be the least favorable. The probability of deep invasion into the myometrium is three to four times higher, and the occurrence of metastases in regional lymph nodes is 16-18 times higher than the frequency with which they occur at those stages of this uterine oncology that are characterized by a higher degree of differentiation.
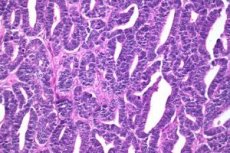
Endometrioid adenocarcinoma of the uterus
Endometrioid adenocarcinoma of the uterus is one of the most common malignant tumors in the uterus. This type of oncology occurs in 75% of cancer cases in women.
In this type of adenocarcinoma, glandular structures arise, forming from one to several layers of tubular epithelial cells, which are characterized by cellular atypia. The tumor parenchyma becomes the site of the emergence of papillary and tubular structures, and in addition, squamous cell metaplasia may form.
Endometrioid adenocarcinoma of the uterus can be provoked by estrogen stimulation; endometrioid hyperplasia can also serve as a prerequisite for its development.
The following varieties are differentiated:
- An extremely aggressive form is serous carcinoma, which has a great deal of similarity to serous carcinoma of the fallopian tubes and ovaries. As a rule, it occurs in 7-10% of cases and is found in elderly women.
- Next, it is necessary to note clear cell carcinoma. The prognosis in its presence is unfavorable, due to the fact that it has a tendency to the appearance of early implantation metastasis in the serous membranes of the peritoneal cavity.
- And finally, the rarest can be considered secretory adenocarcinoma. The prognosis for it is positive in most cases.
Diagnostics uterine adenocarcinoma
If a woman at the age when menopause occurs has uterine bleeding, she should immediately visit a gynecologist to accurately determine the cause as a result of the necessary studies. And, if necessary, conduct additional diagnostic measures in order to exclude, or, on the contrary, confirm the fact of the onset of oncology in the uterus.
Among the main methods used to diagnose uterine adenocarcinoma, it is necessary to note, first of all, a gynecological examination.
During the examination, the specialist may detect a foreign neoplasm in the uterus by palpation. In this case, additional diagnostics are prescribed using the following methods.
As a result of an ultrasound examination (US) of the pelvis, it may be established that the inner layer of the uterus is thicker. In addition, if cancer has already been diagnosed and established, an ultrasound allows metastases to be found.
Scraping of the uterine cavity for diagnostic purposes is performed to obtain the endometrium for subsequent examination under a microscope.
A modern method is hysteroscopic diagnostics and endometrial biopsy. A hysteroscope is an optical device that is inserted into the uterine cavity for internal examination and biopsy – separation of a tissue fragment for subsequent examination under a microscope to detect cancer if there is a suspicion.
What do need to examine?
Differential diagnosis
Today, adenocarcinoma of the uterus is classified by several types of endometrial cancer. Sometimes, differential diagnostics to separate endometrioid adenocarcinoma from atypical hyperplasia of endometrial tissue is associated with certain difficulties. A factor in accurately establishing the appropriate diagnosis is a scrupulous analysis of the state of the stroma. The presence of necrotic changes in its tissues, or a significant decrease in its presence, up to complete disappearance, in areas in the spaces between glandular formations, as well as if specific foamy cells are detected - all this may indicate endometrioid adenocarcinoma.
Who to contact?
Treatment uterine adenocarcinoma
Treatment of uterine adenocarcinoma involves certain methods and techniques of treatment, the appropriateness of which is determined in each specific case based on the stage of the disease process.
The first stage is characterized by the fact that treatment is mainly surgical and consists of removing the uterus along with its appendages.
The second stage, in addition to the removal of the uterus and appendages, also has as an indication the removal of the lymph nodes located near it. This is dictated by the reasons that there is a possibility of metastases in them.
In later stages, treatment is carried out using one of the following methods.
Radiotherapy is a course of dosed irradiation of the corresponding areas of the uterus with special X-rays. As a result, the cells of the pathological focus disintegrate until the tumor is completely destroyed.
Chemotherapy is a method of targeted destructive action with special drugs on adenocarcinoma of the uterus. Treatment of adenocarcinoma of the uterus with chemotherapy occurs with the use of drugs Doxorubicin, Carboplatin, Cisplatin and others.
Surgery for uterine adenocarcinoma
Surgery for uterine adenocarcinoma is a fairly common method of treating this type of uterine cancer.
This type of surgical intervention, performed to remove the body of the uterus, is called a hysterectomy.
In some cases, along with the uterus, the tissues surrounding it may also be removed: the cervix with part of the vagina, both ovaries, fallopian tubes and regional lymph nodes.
The duration of the recovery period after such an operation is determined by the individual characteristics and general health of each specific patient. As a rule, discharge from the hospital can occur after a few days, and in order to fully recover a woman needs from 4 to 8 weeks.
In the first few days after the operation, discomfort, pain, fatigue or general weakness may occur. Sometimes there are bouts of nausea, problems with the bladder and constipation. All these phenomena are temporary and disappear after a very short time.
Surgery for uterine adenocarcinoma causes significant changes in hormonal levels due to a significant decrease in female hormones. This can result in vaginal dryness, hot flashes, and increased night sweats.
Special medications and products, of which there are many today, help to optimize hormonal balance.
More information of the treatment
Prevention
It is not possible to completely avoid the occurrence and development of uterine cancer. However, there is prevention of uterine adenocarcinoma, which offers certain measures and principles, following which you can minimize the risk of uterine oncology.
One of the most important points in this regard is maintaining optimal body weight and keeping the body mass index within the normal range.
To maintain the appropriate body weight, a woman needs to lead an active lifestyle, increase the amount of fresh fruits and vegetables in her diet, and optimize her daily calorie intake.
A decrease in the intensity of carcinogenic factors in the air and in the premises at the workplace also helps to reduce the likelihood of developing cancer.
Prevention of uterine adenocarcinoma can be effective and efficient only if a woman aged 30 and above undergoes regular preventive examination by a gynecologist at least twice a year. Systematic visits to a gynecologist are mandatory from the time a girl begins to live a sexual life.
Such examinations make it possible to detect diseases that precede the development of cancer at early stages.
Forecast
The prognosis for uterine adenocarcinoma is most favorable if the cancerous tumor is detected and diagnosed at the first stage of the disease.
In such a case, a complete recovery is possible as a result of a surgical intervention that is not very severe, followed by appropriate therapy.
In less than a year, the woman will be able to fully return to normal life.
Treatment of uterine adenocarcinoma at its second stage is associated with more significant difficulties, since there is a larger surgical field, and the postoperative period requires a long course of radiological and chemotherapy.
The extent of the uterine damage at this stage often requires its complete removal. This circumstance ultimately leads to the complete loss of the ability to bear children and provokes a severe hormonal imbalance.
The recovery course can take up to three years, and as a result, the body’s healthy state that preceded the disease is still not fully achieved.
The prognosis of stage three uterine adenocarcinoma is aggravated by the fact that in cases of severe metastasis, in addition to removing the uterus itself, it is also necessary to remove part of the vagina, or the entire vagina. Even after three years of recovery, complete recovery is unattainable.
The fourth stage is characterized by the fact that the question of actually fighting for the patient's life becomes relevant. There is a well-founded probability of a fatal outcome.
Recovery measures may have some positive effect, but in the future life will be associated with many aggravating factors.
Prognosis for cervical adenocarcinoma
The unfavorable prognosis for cervical adenocarcinoma is determined by the factors listed below.
A tendency for lesions to spread widely throughout the body.
There is a high probability of death within 5 years from the onset of the disease in its 4th stage.
Metastasis of lymph nodes, features of their localization and large sizes. Direct correlation of the presence of metastases to the percentage of deaths due to this type of cancer in a 5-year time period
The fatality rate increases depending on the size of the pathological neoplasm. Thus, with tumors not exceeding 2 cm, the overwhelming majority of patients survive after 5 years of the disease. Tumor sizes from 2 to 4 cm reduce this probability to 60%. When the cancerous tumor is larger than 4 cm, in almost half of the cases (40%), a fatal outcome occurs.
In cases of tumor infiltration of the parametrium, the number of survivors after 5 years is 69%; in its absence, the survival prognosis is 95%.
The prognosis for adenocarcinoma of the cervix is also negative with deep invasion.
In addition, the prognosis for successful radiological treatment is aggravated by the presence of thrombocytopenia and anemia.