Medical expert of the article

New publications
Brachial nerve plexus root impingement
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Pinching of the brachial plexus root, or, as is often said, pinching of the brachial nerve, is a fairly serious neurological lesion, since the network of intersecting nerves of this anatomical region transmits signals from the spinal cord to the upper limbs, responsible for the motor (motor or muscular) and sensory (that is, cutaneous sensory) innervation of the shoulder, arm and hand.
Epidemiology
The incidence of brachial plexus injury in road traffic accident-related injuries is reported to exceed 40%.
Postoperative damage to the brachial plexus occurs in 12-15% of cases.
The prevalence of compressive effects of tumors on the plexus brachialis roots is estimated at 0.4-1.2%.
And the statistics for the development of brachial plexus paralysis in newborns: 0.4-5% of cases per thousand live births. [ 1 ]
Causes brachial nerve entrapment
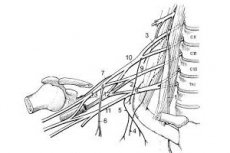
When considering the etiology of the pinched root of the brachial plexus nerve (plexus brachialis) - without touching on the short and long lateral branches emerging from it at various points, it should be recalled that this peripheral plexus is formed by the ventral (anterior) branches of the spinal nerves (cervical C5-C8 and the first thoracic T1) and extends from the base of the neck to the armpit, passing between the anterior and medial scalene muscles (musculus scalenus). And its motor and sensory roots are precisely the aforementioned paired spinal nerves, which exit the spinal cord through the intervertebral openings at the level of the lower cervical and upper thoracic vertebrae. [ 2 ]
The key causes of compression damage to the roots – pinching or compression – can be due to:
- trauma to the brachial plexus and damage to the joint and/or bone-ligamentous apparatus, including birth injuries (obstetric trauma to the brachial plexus); [ 3 ]
- habitual dislocation of the shoulder joint;
- increased physical stress on the shoulder girdle;
- osteochondrosis of the cervical-thoracic spine with the development of anterior scalene muscle syndrome; [ 4 ]
- elongated (hypertrophied) spinous process of the seventh cervical vertebra (C7) – the most protruding in the neck area;
- thoracic outlet syndrome (compression of the nerve roots between the clavicle and the first rib); [ 5 ], [ 6 ]
- growing tumor of the brachial plexus, in particular schwannoma, neurofibroma, neurosarcoma, as well as metastases from primary lung carcinoma.
Risk factors
Risk factors for pinched brachial nerve (brachial plexus roots) include:
- road traffic accidents;
- falls with bruises, dislocations and fractures of the shoulder joint, lower cervical vertebral joints or clavicle;
- frequent carrying of heavy objects, including in a bag on a shoulder strap or in a backpack;
- participation in contact sports, in particular football and wrestling;
- surgical interventions in the brachial plexus area.
In infants, the risk of strangulation is increased during difficult births, which may be due to the large weight, abnormal presentation or dystocia of the fetus's shoulders, as well as the narrow pelvis of the mother.
Pathogenesis
Experts note the vulnerability of nerve roots to compression, since their epineurium (outer layer) is poorly developed, and the connective tissue sheath (perineurium) is absent. [ 7 ]
Compression neuropathies are caused by direct pressure on the nerves. In essence, pinching of the nerve roots (including the brachial plexus) leads to the development of compression ischemic neuropathy with deterioration of the nutrition of the tissue of nerve fibers, which negatively affects their functions. And the pathogenesis of neuropathic pain caused by pinching, muscle (motor) and sensory disorders lies in the partial or complete blockade of nerve conduction. [ 8 ], [ 9 ]
Symptoms brachial nerve entrapment
The first signs of pinching in the form of radicular syndrome depend on which root is subject to compression and its innervation zone (muscles and dermatomes).
Thus, pinching of the C5 root, responsible for the innervation of the muscles of the shoulder girdle and part of the shoulder muscles, weakens the deltoid muscle of the shoulder and part of the biceps (flexing and extending the arm at the elbow joint) and reduces the sensitivity of the skin of its outer surface to the elbow, causing tingling or burning, as well as loss of skin sensitivity - numbness. The pain may radiate to the shoulder.
When the C6 root of the brachial plexus is compressed, symptoms include pain in the shoulder and forearm (which intensifies with arm or neck movements); paresthesia or numbness of the outer side of the forearm, thumb and index finger; decreased strength or complete loss of muscle reflexes of the biceps brachii.
If the C7 root is pinched, there is a loss of skin sensitivity down the back of the hand to the index and middle fingers; a decrease in the triceps reflex (the three-headed muscle of the shoulder that straightens the elbow), as well as pain in the shoulder and forearm (along the back surface), which may radiate under the shoulder blade.
Symptoms of C8 and T1 nerve root entrapment include pain in parts of the shoulder, forearm, hand, and little finger; progressive weakness in the wrist, hand, or fingers; and numbness in the forearm or hand.
A pinched nerve in the shoulder joint is accompanied by pain in the shoulder and neck (especially when turning the head from side to side), numbness and muscle weakness of the arm and hand (thenar muscles of the palm), leading to difficulties with raising the arm and fine motor skills.
Read also – Brachial Plexus Injury Syndromes
Complications and consequences
Complications of brachial nerve (brachial plexus root) entrapment can be very serious, and some consequences are irreversible.
For example, pain resulting from damage to nerve roots can become chronic and reach causalgia, and limited mobility of the arm or hand leads to so-called joint stiffness, which aggravates the difficulty in moving the limb.
Compression of nerve fibers causes not only muscle denervation, but also their gradual atrophy.
Severe injuries to the brachial plexus with pinching of its roots can lead to paralysis of the arm and disability.
Diagnostics brachial nerve entrapment
A physical examination by a neurologist (with an assessment of the range of motion on the affected side) and anamnesis are supplemented by mandatory instrumental diagnostics, including an X-ray of the shoulder joint and shoulder girdle, an X-ray of the cervical spine, an ultrasound of the brachial plexus, electromyography and electroneuromyography (a study of nerve conduction). If necessary, a CT or MRI is performed. [ 10 ]
Differential diagnosis
Differential diagnostics should exclude brachial plexitis, inflammatory diseases of the shoulder joint, pinching of the C1-C4 cervical plexus roots (cervical radiculopathy), cervical facet joint syndrome, tunnel syndromes, myofascial syndrome, compression syndromes of the superior thoracic aperture, endocrine peripheral neuropathies, autoimmune diseases of motor neurons, etc.
Who to contact?
Treatment brachial nerve entrapment
Once a diagnosis is made, in most cases, treatment for a pinched shoulder nerve is carried out at home.
The main pharmacological drugs are symptomatic: pain pills - non-steroidal anti-inflammatory drugs (NSAIDs) with an analgesic effect, for example, Paracetamol, Ibuprofen and other neuralgia pills
Corticosteroid injections may also be prescribed to relieve pain.
To restore motor functions and expand the range of motion of the arms and hands, physiotherapy is used: exercise therapy and massage for pinched shoulder nerves.
For more details, read the publications:
- Treatment of neuropathy of the upper extremities
- Treatment of neuropathic pain
- Treatment for numbness in hands
Additionally, herbal treatment may be performed using: calamus root extract (Acorus calamus) - as a pain reliever; ginkgo biloba - to improve tissue trophism and reduce oxidative stress, as well as to increase the conduction of nerve impulses in the central nervous system; sage (Salvia officinalis) - as a means of strengthening the nervous system.
Prevention
Most often, damage to the brachial plexus cannot be prevented, except by limiting physical activity on the shoulder girdle.
Forecast
In cases of relatively minor damage to the brachial plexus, the prognosis is more favorable, since in such cases, in 90% of patients, the mobility and sensitivity of the upper limbs - with proper treatment - can be normalized. Severe damage is characterized by chronic dysfunction of the roots of the brachial plexus.