
Pericardial effusion
Last reviewed: 23.11.2021

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Among the many possible complications of cardiovascular pathologies, a special place belongs to pericarditis - these are diseases that are not always accompanied by severe clinical symptoms, but often pose a threat to the health and life of the patient. One of such dangerous variants of pathology is exudative pericarditis, in which an excess volume of fluid accumulates in the space between the sheets of the outer inflamed cardiac membrane. In a healthy person, such a volume is within 25 ml, and with pericarditis, it increases ten or more times. The rapid filling of the space leads to squeezing of the muscle layer, which is a life-threatening condition and requires emergency medical attention. With a slow accumulation of fluid, stagnation is noted, and circulatory failure is increasing. [1]
Epidemiology
In most patients, pericardial effusion becomes a complication or one of the signs of another cardiovascular or visceral disorder, only in rare cases does it acquire the character of an independent disease.
Regardless of the origin, pericardial effusion belongs to the category of dangerous (often life-threatening) conditions. According to pathoanatomical statistics, the disease (experienced or actual at the time of the patient's death) is detected in about 5% of cases. But the frequency of intravital diagnostics is much lower, which is associated, first of all, with certain diagnostic difficulties.
Female and male patients suffer from exudative pericarditis approximately equally.
Effusion in the pericardium is possible for all ages and groups. The predominant etiology of effusion depends on demographic characteristics such as age, geography, and comorbidities. There are few data on the prevalence and frequency of pericardial effusions. Viral pericarditis, leading to effusion, is the most common cause in developed countries. In developing regions , pericardial effusion due to Mycobacterium tuberculosis. Pretty common. Bacterial and parasitic etiologies are less common. Among non-inflammatory pericardial effusions, multiple malignancies can lead to pericardial effusion. In patients with pericardial effusion, malignant neoplasms account for 12% to 23% of cases of pericarditis. In HIV patients, pericardial effusion was noted in 5–43%, depending on inclusion criteria, with 13% having moderate to severe effusion. According to a study in pediatric patients, the main causes of pericarditis were postcardiac surgery (54%), neoplasia (13%), renal (13%), idiopathic or viral pericarditis (5%), and rheumatologic (5%). And pericardial effusion in children. [2], [3], [4]
Causes of the exudative pericarditis
Pericardial effusion is more often a consequence, not an underlying cause: the disease develops in response to an existing polyserositis or other pathology, accompanied by a lesion of the pericardium.
According to the etiological factor, infectious exudative pericarditis (specific and nonspecific), non-infectious pericarditis (immunogenic, mechanical, intoxication) and idiopathic (with an unknown cause) pericarditis are distinguished. [5]
The nonspecific form of infectious pericarditis is most often provoked by:
- cocci (strepto or staphylococcus, pneumococcus);
- viral infection (influenza vitus, enterovirus).
- A specific form of pericarditis can be provoked by the causative agent of such diseases:
- tuberculosis, brucellosis;
- typhoid fever, tularemia;
- fungal infections, helminthiasis, rickettsioses.
Pericardial effusion of tuberculous origin develops when mycobacteria enter the pericardium with lymph flow from the lymph nodes of the mediastinum, trachea and bronchi. A purulent form of the disease can occur as a complication of coronary surgery, as well as in infectious and inflammatory lesions of the endocardium, immunosuppressive treatment, with self-opening of a pulmonary abscess. [6]
The non-infectious type of exudative pericarditis is often idiopathic - that is, it is not possible to find out the cause of its appearance. If the reason is still determined, then most often it is:
- about malignant lesions of the pericardium (in particular, about mesothelioma);
- invasions and metastases in pulmonary carcinoma, breast cancer, lymphoma or leukemia;
- about connective tissue pathologies (rheumatism, systemic lupus erythematosus, etc.);
- about allergic reactions (serum sickness);
- about uremia accompanying chronic renal failure;
- about radiation damage to the mediastinal organs;
- about the early stage of myocardial infarction;
- about the reduced function of the thyroid gland;
- about impaired cholesterol metabolism. [7]
Risk factors
A small amount of effusion is always present in the pericardial space. This is necessary to ensure glide during heartbeats. The increase in this volume occurs as a result of an inflammatory reaction and an increase in vascular permeability. With the development of pathology, serous layers are not able to absorb excess effusion, which enters at an accelerated rate, therefore, its level increases rapidly. [8]
Pericardial effusion is predominantly secondary in nature, as it is a complication of other diseases and pathological conditions:
- severe infectious diseases;
- autoimmune disorders;
- allergic processes;
- traumatic injuries (blunt injuries, penetrating injuries);
- the effects of radiation;
- blood diseases;
- tumor processes;
- myocardial infarction;
- metabolic disorders;
- cardiological operations;
- insufficient renal function.
Pathogenesis
Violation of the blood supply to the pericardium in exudative pericarditis can manifest itself to varying degrees, depending on the amount of accumulated fluid, on the rate of accumulation, on the quality of adaptation to the load of the external pericardial layer. If the fluid enters gradually, then the leaf has time to adapt, to stretch: the pressure inside the pericardium changes slightly, and the intracardiac circulation is compensated for a long time. In patients with exudative pericarditis, different amounts of exudate can accumulate - from 400-500 ml to 1.5-2 liters. The larger the volume of such fluid, the more the organs and nerve endings located near the heart are compressed. [9]
If the exudate accumulates in a large volume in a short period of time, then the pericardium does not have time to adapt, the pressure in the pericardial space increases significantly, and a complication develops - cardiac tamponade. [10]
Fluid with exudative pericarditis can be reorganized in the future, being replaced by granulations. These processes cause pericardial thickening: the space is preserved or obliterated. [11]
Symptoms of the exudative pericarditis
The first and main symptom in exudative pericarditis is chest pain, which increases during a deep breath. The pain makes itself felt sharply, acutely, sometimes like a heart attack. The patient's suffering is somewhat relieved by sitting.
Features of pain in exudative pericarditis:
- starts abruptly, lasts a long time (sometimes does not go away for several days);
- marked behind the sternum or slightly to the left;
- gives to the left hand, collarbone, shoulder, neck area, to the left half of the lower jaw;
- does not disappear after taking nitroglycerin;
- increases with inspiration, during coughing or swallowing;
- worse in a horizontal position, especially when trying to lie on your back;
- decreases when seated with a forward bend.
Fever is less common.
It is important to understand that often pericardial effusion occurs simultaneously with other cardiac pathologies - in particular, with myocardial infarction. Therefore, the clinical picture can expand, taking into account another disease or acute condition, which greatly complicates the diagnosis.
First signs
As the exudate accumulates in the pericardium, there are signs of compression of the myocardium and the respiratory system. The most common symptoms are:
- chest pain;
- persistent hiccups;
- an unexplained feeling of anxiety;
- persistent cough;
- hoarse voice;
- feeling of lack of air;
- shortness of breath while lying down;
- periodic depression of consciousness.
Chest pain sometimes resembles an angina attack, heart attack, or pneumonia:
- increases with physical activity, inhalation, swallowing;
- disappears when bending forward in a sitting position;
- starts abruptly, lasts a long time;
- may have different intensities;
- can give to the left upper limb, shoulder, neck area.
The position of the patient with exudative pericarditis
A patient with exudative pericarditis usually sits slightly leaning forward: this position helps to relieve pain. Other external signs are also noteworthy:
- the skin is pale, the fingers are bluish;
- the chest swells, the veins of the neck swell (they do not collapse when inhaling);
- heartbeat is frequent, irregular, heart beat is not detected or weak;
- heart sounds are weakened by auscultation;
- ascites grows, the liver is enlarged.
Forms
To date, the following classification of pericarditis is considered generally accepted:
- By etiological characteristics:
- bacterial pericarditis;
- infectious and parasitic pericarditis;
- unspecified pericarditis.
- By pathogenetic and morphological characteristics:
- chronic adhesive;
- chronic constrictive;
- non-inflammatory pericarditis ( hydropericardium , chylopericardium);
- hemopericardium .
- By the nature of the flow:
- acute exudative pericarditis;
- chronic exudative pericarditis.
Acute pericarditis lasts less than six weeks, and chronic pericarditis lasts more than six weeks. The acute form develops against the background of an infectious process, or becomes a complication of sepsis, tuberculosis, rheumatism, etc. The inflammatory reaction captures the external and internal pericardial sheets. The initial stages of pathology most often proceed without exudative phenomena, like dry pericarditis, but later exudative pericarditis develops.
If the acute form is not treated promptly, then it acquires a chronic course , in which thickening and adhesion of the pericardial sheets occurs: an exudative-adhesive process is formed.
Exudative adhesive pericarditis is otherwise called adhesive, adhesive. This division is considered conditional. This name is understood as such an outcome of pericarditis, in which residual phenomena are noted in the form of an adhesive process between the pericardial sheets, or between the pericardium and nearby organs. Sometimes in the hardened pericardium, calcium crystals accumulate, liming begins.
Complications and consequences
Pericardial effusion may include transudate (hydropericarditis), exudate, purulent fluid (pyopericarditis), and blood (hemopericarditis). Large amounts of exudate are characteristic of tumor processes, tuberculosis, uremic or cholesterol form of pericarditis, helminthiasis and myxedema. Gradually increasing effusion most often does not show any symptoms, but with a rapid accumulation of exudate, cardiac tamponade can occur.
Cardiac tamponade is a stage of decompensation when the heart is compressed, when fluid accumulates in the pericardial space with an increase in pressure in it. Surgical tamponade is accompanied by a rapid increase in pressure, and with an inflammatory reaction, this occurs within several days or weeks.
Local compression may cause shortness of breath, impaired swallowing, hoarseness, hiccups, or nausea. Distant heart sounds. When the base of the lungs is compressed, there is a dullness under the left scapula. With the onset of tamponade, intrathoracic discomfort, shortness of breath, stress tachypnea with transition to orthopnea appear, a cough occurs, the patient may periodically lose consciousness.
In turn, cardiac tamponade can be complicated by renal failure, "shock" liver, mesenteric ischemia, plethora of abdominal organs.
If difficulties arise with diagnosis, pericardiocentesis, pericardioscopy, biopsy of the epicardium and pericardium are performed (PCR, immunochemistry and immunohistochemistry are involved).
Diagnostics of the exudative pericarditis
Pericardial effusion is diagnosed based on information obtained during physical examination, laboratory and instrumental diagnostics.
The physical examination includes listening to cardiac activity with a stethoscope. With exudative pericarditis, there will be some protrusion of the anterior surface of the chest and a slight edema in the pericardial zone, weakness or loss of the apical impulse, expanded boundaries of the relative and absolute dullness of the heart, dullness of the percussion sound. The onset of the development of a complication - cardiac tamponade - is indicated by an increase in central venous pressure, a decrease in blood pressure, an increase in heart rate with a transient disturbance of the heart rhythm, a paradoxical pulse. [12]
Analyzes are carried out in a general diagnostic aspect:
- a general blood test (leukocytosis, accelerated ESR, signs of secondary pericarditis are possible);
- general urine analysis (signs of nephrotic syndrome, renal failure).
Additionally diagnosed:
- blood electrolytes;
- total protein and fractions;
- blood urea;
- creatinine level and glomerular filtration rate;
- AST, ALT, bilirubin (total, direct);
- lipid spectrum;
- coagulogram;
- immunogram;
- tumor markers;
- PCR for tuberculosis in the blood;
- antinuclear antibodies;
- rheumatoid factor;
- thyroid hormones;
- procalcitonin test.
Instrumental diagnostics includes the following procedures:
- chest x-ray;
- echocardiography, electrocardiography;
- pericardial puncture
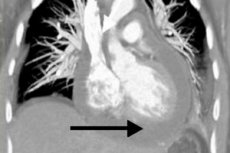
X-rays are given if pericarditis is suspected to assess the level of exudate in the pericardial space. The shadow of the heart may appear enlarged if there is a large amount of fluid in the cavity. With a relatively small amount of effusion, radiographs may not indicate pathology. In general, an enlarged shadow and smoothing of the contour of the heart, weak pulsation, a change in the shape of the organ (triangle - if chronic effusion is present for a long time) are considered radiological signs of exudative pericarditis. For clarification, it is possible to prescribe multispiral computed tomography, which usually confirms the presence of pathological fluid and thickening of the layers of the pericardium. [13]
Pericardial effusion on the ECG is manifested by a decrease in the amplitude of all teeth. With additional ultrasound of the heart (echocardiography), it is possible to determine the limitation of the mobility of the heart by fluid. [14], [15]
Puncture of the pericardium with further study of the nature of the exudate is necessary to clarify the cause of the violation. The withdrawn fluid is subjected to general clinical , bacteriological , cytological analysis, as well as research for AHAT and LE-cells. [16]
Differential diagnosis
The course of exudative pericarditis should be distinguished from the formidable complication of this disease - cardiac tamponade .
|
The clinical picture of tamponade |
Changes in blood pressure, increased heart rate, pulse paradoxicality, shortness of breath against the background of clean lungs. |
|
Provoking mechanisms |
Medicines (anticoagulants, thrombolytics), cardiac surgery, catheterization, closed chest injuries, tumor processes, connective tissue pathologies, sepsis or renal failure. |
|
Electrocardiogram |
Normal or nonspecific ST-T changes, bradycardia, electromechanical dissociation, electrical alternation. |
|
Chest x-ray |
Increased cardiac shadow against the background of clear pulmonary fields. |
|
Echocardiogram |
Diastolic collapse of the anterior wall of the right ventricle, right atrial or left atrial collapse, increased rigidity of the left ventricular wall in diastole, dilated inferior vena cava, "floating" heart. |
|
Doppler ultrasonography |
Decrease in systolic and diastolic venous blood flow during inhalation, increased reverse blood flow during atrial contraction. |
|
Color Doppler (M-Mode) |
In the mitral / tricuspid valve, pronounced respiratory fluctuations in blood flow are noted. |
|
Cardiac catheterization |
The diagnosis is confirmed and hemodynamic disturbances are assessed. |
|
Ventriculography |
Atrial contractions and small overactive chambers of the heart ventricles. |
|
Coronary angiography |
Compression of the coronary arteries in diastole |
|
CT scan |
The subepicardial fat of the two ventricles is not visualized, which indicates the tubular configuration of the anteriorly displaced atria. |
Often myocarditis and pericardial effusion accompany each other, which is manifested by a general or local dysfunction of the heart muscle. The laboratory features of this phenomenon are an increased level of cardiac troponins I and T, the CF fraction of CF, the level of myoglobin and tumor necrosis factor in the blood. On the electrocardiogram, there is a concordant ST segment elevation.
Who to contact?
Treatment of the exudative pericarditis
Therapeutic tactics for exudative pericarditis depends on the causes and clinical course of the disease.
Among non-steroidal anti-inflammatory drugs, Ibuprofen is preferred, which is associated with relatively rare side effects, a positive effect on coronary circulation and the ability to change the dosage over a wide range. Usually, the patient is prescribed 300-800 mg of the drug every 7 hours, for a long time (until the disappearance of the pericardial exudate). [17]
All patients are prescribed proton pump inhibitors to protect the digestive tract.
Corticosteroids are prescribed when indicated:
- connective tissue pathologies;
- autoreactive pericarditis;
- uremic pericarditis.
Intrapericardial administration of corticosteroids is effective and helps prevent the development of side effects that occur with their systemic use. Against the background of a gradual reduction in the dosage of Prednisolone, ibuprofen is prescribed in advance.
With cardiac tamponade, surgical treatment is indicated in the form of pericardiocentesis.
Essential medicines for pericardial effusion
|
Non-steroidal anti-inflammatory drugs (Ibuprofen 200-400 mg, Diclofenac 25-50 mg, etc.) |
Up to 3 times a day as a pathogenetic anti-inflammatory treatment. Side effects: gastrointestinal disorders. |
|
Glucocorticoid systemic agents (Prednisolone 5 mg, Prednisolone 25 mg / ml, etc.) |
In individual dosages, as a pathogenetic anti-inflammatory treatment for systemic pathologies. |
|
Glucocorticoid drugs for intrapericardial administration (Triamcinolone 1 ml / 0.01 g, 1 ml / 0.04 g, etc.) |
According to an individual protocol. |
|
Proton pump inhibitors (Omeprazole 20 mg, Pantoprazole 20 mg) |
Once a day to protect the digestive tract. |
|
Acetylsalicylic acid 75 mg, 100 mg. |
Once a day, if pericardial effusion is combined with a heart attack. |
|
Azathioprine 0.05 g |
1-2.5 mg / kg per day for 1-2 doses, with ineffectiveness of non-steroidal anti-inflammatory drugs and corticosteroids. |
|
Cyclophosphamide 50 mg, 100 mg |
Orally at 1-5 mg / kg per day, intravenously at 10-15 mg / kg in the absence of the effectiveness of non-steroidal anti-inflammatory drugs and corticosteroids. |
|
Aminoglycosides (Tobramycin 1 ml 4%) |
With bacterial exudative pericarditis 1-2 times a day until clinical signs of eradication appear (1-3 weeks). |
|
Antiarrhythmics (Amiodarone 150 mg in amp., 200 mg in tablets; Verapamil 5 mg in ampoules, 40-80 mg in tablets) |
1-2 times a day to eliminate and prevent arrhythmias. |
|
Inotropic drugs (Dobutamine 20 ml 250 mg) |
With a sharp drop in blood pressure and with a peripheral picture of collapse. Side effects: dizziness, headache. |
Physiotherapy treatment
The massage is recommended for chronic exudative pericarditis, during remission. Massage the area of the back, lower extremities (starting from the proximal regions), chest and abdomen. Techniques used: stroking, rubbing, kneading, muscle shaking, excluding blows and squeezing. The duration of the massage session is about 15 minutes. The course will require 10 to 15 sessions. After the massage, oxygen therapy is performed.
In case of heart rhythm disturbances, physiotherapy exercises, walks, skiing, swimming are indicated. Exercise therapy classes are carried out with musical accompaniment. Before going to bed, massage of the neck area, back and lower extremities is performed. Coniferous and oxygen baths, electrophoresis, electrophoresis, diet therapy with additional food fortification are recommended.
Upon completion of the treatment course, a spa treatment with swimming, walks along the coast, as well as oxygen cocktails is shown.
Herbal treatment
Alternative remedies are a good help in the treatment of pericardial effusion. Homemade and affordable recipes will help strengthen the heart, improve blood circulation, restore well-being and heart function.
- Infusion of elecampane rhizome and oats. Take 100 g of oat grains, wash with the husk, pour 500 ml of drinking water, bring to a boil, remove from heat. Pour in 100 g of chopped elecampane rhizomes, bring to a boil again, remove from heat, cover with a lid and insist for 2 hours. Then filtered, add 2 tsp. Honey. It is taken according to the scheme: three times a day, they drink 100 ml of the drug half an hour before meals, for two weeks.
- Bean broth. Grind the bean pods (2 tbsp. L.), Pour 1 liter. Water, bring to a boil and boil for five minutes. Add 1 tbsp. L. Hawthorn, motherwort, mint, lily of the valley, boil for another 3 minutes. Cover with a lid, infuse for 4 hours, and then filter. Store the product in the refrigerator. Take 4 tbsp. L. Three times a day, half an hour before meals.
- Hawthorn decoction. Take 500 g of hawthorn fruit, pour 1 liter of water, bring to a boil and boil for 15 minutes, filter and cool. Add 20 g of honey, mix. Within a month, take 2 tbsp daily. L. Remedies before meals.
- Viburnum infusion. Take 500 g of berries (dry, fresh, frozen), pour 1 liter of boiling water, insist for 1.5 hours. Drink 200 ml twice a day, with honey. The course of treatment is 1 month, then after 2 months the treatment can be repeated.
- Tartar broth. Take 1 tbsp. L. Medicinal raw materials, pour 250 ml of water, boil for 15 minutes. Cool, filter, take 100 ml 4 times a day, but the condition improves.
Surgery
Absolute indications for pericardiocentesis in exudative pericarditis are:
- cardiac tamponade;
- a large amount of exudate in the pericardial space;
- suspicion of purulent or tuberculous pericarditis, neoplastic pericardial effusion.
Aortic dissection is considered a contraindication to the procedure. Uncorrected coagulopathy, anticoagulant therapy, and thrombocytopenia may become relative contraindications.
Pericardiocentesis under fluoroscopic guidance and ECG monitoring is performed by access from under the xiphoid process. A long needle with a mandrel is advanced towards the left shoulder, keeping an angle of 30 ° to the skin surface, which prevents damage to the cardiac, pericardial and internal arteries of the chest. Attempts to aspirate exudate are periodically carried out.
After correct installation of the catheter, the exudate is removed in parts, at a time - no more than 1000 ml, in order to avoid acute expansion of the right ventricle and the development of sudden decompression syndrome. Continue to drain until the volume of effusion decreases to less than 25 ml per day (every 5 hours). [18]
All patients are monitored for the timely detection of decompensation, which is possible after the pericardial drainage procedure. First of all, treatment is directed at eliminating the cause of pericardial effusion, and not at eliminating the effusion as such.
Possible complications of pericardiocentesis:
- myocardial perforation;
- hemothorax, pneumothorax;
- air embolism;
- arrhythmia (often - vasovagal bradycardia);
- accession of infection;
- damage to the abdominal and peritoneal organs.
The only radical treatment for chronic constriction in exudative pericarditis is the operation of pericardiectomy . [19]
Prevention
After the patient recovers after exudative pericarditis, the following preventive rules are established:
- Long-term use of non-steroidal anti-inflammatory drugs with cancellation after elimination of exudate in the pericardium.
- Timely use of corticosteroids in an individually selected dosage.
- Gradual withdrawal of corticosteroids (for at least three months), with a transition to non-steroidal anti-inflammatory drugs.
- Prevention of disorders of the digestive tract associated with prolonged use of non-steroidal anti-inflammatory and corticosteroid drugs.
- Timely pericardiocentesis with signs of cardiac tamponade.
- Timely pericardiectomy for symptomatic constrictive pericarditis.
- Providing treatment for the underlying disease (tumor processes, tuberculosis, systemic diseases, etc.).
- Upon completion of treatment of acute exudative pericarditis for 12 months, the patient is monitored for the timely detection of exacerbation or complications. Once every three months, a blood test, an electrocardiogram, an echocardiogram is performed.
In general, a significant reduction in the risk of developing pericardial effusion is facilitated by the timely diagnosis of heart disease and the treatment of other disease processes that can spread to the heart area.
The main preventive measures are as follows:
- eradication of bad habits;
- good nutrition;
- normalization of work and rest regimes;
- active lifestyle;
- avoidance of stress, hypothermia;
- timely treatment of any pathologies in the body;
- hardening, strengthening the immune defense;
- timely visit to the doctor, including for preventive examinations.
Forecast
The main complication in acute pericardial effusion is cardiac tamponade. In every third patient, the inflammatory process spreads to the heart muscle, which leads to the appearance of paroxysmal atrial fibrillation or supraventricular tachycardia. Pericardial effusion often transforms into a chronic or constrictive form.
Correct and timely treatment in the absence of complications guarantees the onset of recovery in about three months. The patient gradually returns to normal life rhythm. Longer rehabilitation is spoken of with the development of a recurrent disease, when there is a periodic re-accumulation of exudate. [20]
Postoperative recovery is usually longer: within a week the patient is hospitalized, then he is discharged at the place of residence, with further cardiological observation. Full recovery of cardiac function occurs after about 6 months. [21]
With the development of cardiac tamponade, the risk of death of the patient increases significantly. In general, the prognosis depends on the cause of the pathology and the timeliness of diagnosis and treatment. [22]
Pericardial effusion, not complicated by cardiac tamponade, has a relatively favorable prognosis. Full therapy or surgery can restore cardiac function, and the person will be considered practically recovered. Life expectancy can be reduced by the formation of multiple adhesions even after surgery.