Medical expert of the article

New publications
Thoracocentesis
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
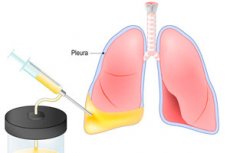
If fluid enters or accumulates in the pleural cavity, it can cause dangerous respiratory problems that can lead to the death of the patient. Thoracentesis, or pleurocentesis, helps to eliminate the danger. The procedure is a puncture of the chest wall with further removal of fluid. Thoracocentesis can carry both therapeutic and diagnostic load - for example, to withdraw and take fluid for research, for the introduction of medicinal solutions. Fluid accumulation in the pleural cavity is associated with poor health, difficulty breathing even in a calm state. After thoracocentesis and removal of fluid, breathing improves, the work of the respiratory and cardiovascular system is restored. [1], [2]
Indications for the procedure
When is a thoracentesis necessary?
The pleural cavity is a space in the thorax bounded by the pleura. In turn, pleura is the smooth serous membrane of the lungs, consisting of two sheets: the parietal sheet shelters the chest inside and the visceral sheet adjoins the lungs. Normally, a small volume of serous fluid is present in the pleural cavity, acting as a lubricant to reduce friction during the respiratory act. If a disease develops, more fluid may accumulate between the pleural sheets - a so-called pleural effusion. However, the fluid can also have other origins, such as:
- Transudate is edematous moisture that leaks into the pleura due to increased blood pressure and decreased osmotic plasma pressure. Such effusion is characteristic of failure of heart function or cirrhosis.
- Exudate is an inflammatory moisture that penetrates into the pleura due to increased permeability of vascular walls. At the same time, some blood cells, proteins and other substances seep out of the plasma. Exudative effusion is a typical sign of oncologic processes, lung inflammation, viral lesions.
If the volume of pleural effusion is small and there is no irritation of the pleural sheets, the person usually does not feel suspicious symptoms. Such a problem is detected accidentally during diagnostic measures for other problems in the body, or during a preventive examination.
If the effusion volume is large enough, the patient has difficulty breathing, a feeling of discomfort and pressure in the chest, pain during inhalation, cough, general weakness, fatigue.
Thanks to thoracocentesis, the fluid is removed, the person's condition improves, there is an opportunity to conduct laboratory diagnostics of the effusion and find out the causes of the violation.
The main indications for thoracocentesis:
- Pulmonary diseases accompanied by the discharge of blood or lymph into the pleural space;
- Exudative pleurisies;
- Air entering the pleural space (Pneumothorax );
- Pleural empyema (pus accumulation in the pleural space).
Thoracentesis for pneumothorax is indicated in patients younger than 50 years of age in first-time spontaneous episodes with a volume of 15 to 30%, without significant respiratory distress. Drainage is performed if thoracentesis is ineffective, as well as in large or secondary pneumothorax, patients with respiratory failure and elderly patients (over 50 years).
Thoracocentesis in hydrothorax is prescribed only for massive volumes of effusion: small hydrothoraxes do not need special treatment, as the resorption of fluid occurs independently, provided competent treatment of the underlying pathology.
Pleurodesis may be used as an adjunct to thoracentesis, i.e., injection of sclerosing agents into the pleural space that adhere both pleural sheets.
Thoracocentesis in hemothorax is indicated in case of prolonged intrapleural bleeding, in case of damage to vital organs, as well as in cases where clotted blood prevents lung expansion. If there is damage to large vessels or thoracic organs, emergency thoracotomy with vascular ligation, suturing of the damaged organ, removal of accumulated blood is indicated. In coagulated hemothorax, videothoracoscopy or open thoracotomy is performed to remove blood clots and sanitation of the pleural space. If the hemothorax becomes suppurative, the treatment is the same as for purulent pleurisy.
Preparation
Before thoracentesis, the patient must undergo an examination, including a medical examination, chest X-ray, ultrasound, CT scan. Obligatorily prescribe laboratory diagnostics - in particular, study of blood coagulation function. If the patient's condition is unstable, there are high risks of decompensated conditions, it may be necessary to conduct additional studies - for example, electrocardiography and determine the degree of blood saturation.
The attending physician preliminarily consults the patient, clarifies important points regarding the procedure, voices possible risks and side effects. The patient must sign his consent to perform thoracentesis (if the patient is unable to do so, the document is signed by his closest relatives, family members). If the patient has taken anticoagulants, if there is a tendency to allergic reactions, it is important to inform the doctor about it.
Immediately before the manipulation of thoracocentesis, an additional examination of the patient is performed, pulse and blood pressure are measured.
Thoracocentesis instrument set
Thoracocentesis requires this set of instruments and supplies:
- Kit for local step-by-step anesthesia (a pair of sterile syringes of 10 ml capacity, sterile needles for subcutaneous and intramuscular injection, sterile tray and dressing materials, antiseptic solution and anesthetic, medical glue and plaster, several sterile gloves, masks, antishock medications);
- A sterile Dufault needle or puncture needle measuring 70-100 mm with a sharp oblique cut and an internal diametral dimension of 1.8 mm;
- Sterile extension tube of 20 cm or more (Reson or polyvinyl chloride) with standard adapters;
- A tube clip designed to prevent air from entering the pleural space;
- Sterile scissors and tweezers;
- A rack with sterile corked tubes for placing in them the fluid withdrawn during thoracentesis from the pleural cavity for further bacteriological examination.
Technique of the thoracentesis
It is optimal to perform thoracentesis under ultrasound guidance to find out the optimal point for needle insertion.
Before the procedure, the doctor determines the level of effusion (preferably by ultrasonography), which is marked on the skin with appropriate marks. Next, the site for the puncture is determined:
- In order to remove fluid - between the VII and VIII ribs, adhering to the conditional line from the scapular edge to the armpit;
- To remove air - in the II subcostal region below the clavicle.
The area of the proposed thoracocentesis is treated with antiseptic and anesthetized layer by layer. The puncture itself is performed using a needle, which is replaced by a puncture needle after entering the pleural space. Thanks to it, the specialist releases air or effusion, then treats the puncture area with antiseptic to prevent the development of infectious complications.
Diagnostic thoracocentesis involves visual evaluation of the extracted biomaterial with further referral for laboratory examination. It is important to clarify the physicochemical, microbiological, cytological parameters of pleural contents, which will help to clarify the causes of pathology.
Therapeutic thoracocentesis involves treatment of the pleural cavity with antiseptic solutions to prevent the development of purulent infectious process. The simultaneous use of antibiotic solutions, enzyme substances, hormonal and antitumor drugs is possible.
Thoracocentesis of the pleural cavity can be performed both in the inpatient and outpatient setting. During the procedure, the patient sits with his back straightened and slightly leaning forward. It is also possible to perform manipulations in the supine position - in particular, if the patient is connected to an artificial lung ventilation device. In such a situation, the patient is placed on the edge of the couch, the arm on the side of thoracentesis is placed behind the head, a roller (towel) is placed under the area of the opposite shoulder.
The procedure is performed using local stepwise (layer-by-layer) anesthesia: anesthetic (anesthetic solution) is infiltrated into the skin, followed by subcutaneous tissue, rib periosteum, intercostal muscles and parietal pleura. In some cases, light sedation may be required with the administration of medications to help the patient remain calm and relaxed throughout the procedure and afterwards.
Thoracocentesis and pleural puncture are minimally invasive procedures that can be both diagnostic and therapeutic and are performed routinely or urgently. The biomaterial obtained during the procedure is labeled and sent for laboratory analysis. If the amount of effusion is small and blood is present, it is transported together with an anticoagulant to avoid clotting (clotting).
Laboratory tests are performed on the following indicators:
- PH level;
- Gram staining;
- Cell number and differentiation;
- Glucose, protein, lactic acid dehydrogenase;
- Cytology;
- Creatinine, amylase (if esophageal perforation or pancreatic inflammation is suspected);
- Triglyceride index.
The transudative fluid is usually clear, while the exudative fluid is turbid, yellowish-brownish, and sometimes bloody.
If the pH factor is less than 7.2, this is an indication to perform drainage after thoracentesis.
Cytology is necessary to identify tumor structures in the pleural space. Thanks to immunocytochemical analysis, it is possible to determine their characteristics and prescribe the most optimal treatment.
Microflora seeding is important for the diagnosis of microbial infection.
Contraindications to the procedure
There are no absolute contraindications to performing thoracentesis. Relative contraindications include the following:
- Lack of clear information about the area of fluid localization;
- Blood clotting disorders, treatment with anticoagulants;
- Deformities, anatomical changes in the thorax;
- Extremely small amount of fluid (in this case, therapeutic thoracentesis is inappropriate, and diagnostic thoracentesis is problematic);
- Dermatologic infectious pathologies, shingles in the area of the puncture;
- Decompensated conditions, severe pulmonary pathologies;
- Severe uncontrollable coughing fits;
- Mental instability that prevents adequate performance of the procedure;
- Artificial ventilation with positive pressure (increased risk of complications).
Each case of contraindication is evaluated individually, taking into account the urgency of thoracentesis.
Complications after the procedure
Such a consequence of thoracocentesis as cough and chest pain is considered normal and goes away after a few days. If the problem persists for a long time or worsens, it is necessary to consult a doctor. Consultation with a specialist will also be required if dyspnea or severe chest pain occurs after thoracocentesis. In some cases, anti-inflammatory drugs will be required.
To avoid the development of unfavorable consequences after thoracentesis, in some cases, radiography is performed. This is necessary to exclude pneumothorax, to determine the volume of remaining fluid and the state of lung tissue. Radiography is especially recommended if:
- The patient is on a ventilator;
- The needle was inserted twice or more;
- Air was removed from the pleural space during thoracentesis;
- After thoracentesis, there were signs of pneumothorax.
It should also be understood that mechanical removal of effusion from the pleural cavity during thoracentesis has no effect on the cause of its accumulation. Conversely, in breast or ovarian cancer, small cell lung cancer and lymphoma, systemic chemotherapy in almost half of cases contributes to the normalization of the outflow of fluid from the pleural space.
The risks of problems during and after thoracentesis depend on many factors - first of all, on the qualifications and knowledge of the doctor. If the specialist is careful and has sufficient experience in performing such manipulations, the probability of complications is minimized. Nevertheless, it is impossible to completely exclude such a possibility.
Complications following a thoracentesis procedure can be threatening or non-threatening. The most common threatening complications include:
- Pneumothorax - accumulation of air in the pleural space with subsequent lung collapse (observed in 11% of all complications);
- Hemothorax - accumulation of blood in the pleural space (less than 1% of cases);
- Injury to the spleen or liver (less than 1% of cases);
- Pleural purulent processes, empyema;
- Metastasis (in malignant tumors).
Non-threatening complications of thoracentesis:
- Chest pain (more than 20% of cases);
- Inability to aspirate pleural effusion (in 13% of cases);
- Cough (more than 10% of cases);
- Subcutaneous hemorrhages (in 2% of cases);
- Subcutaneous fluid accumulation - seroma (less than 1%);
- Stress fainting as a result of arrhythmias and decreased blood pressure.
To minimize the risks of complications after thoracentesis, it is recommended to entrust the procedure to qualified specialists with sufficient experience in performing such manipulations. Professional approach, accuracy, care and responsibility towards each patient can reduce the likelihood of problems to a minimum.
Care after the procedure
Immediately after completion of thoracentesis, the rehabilitation period begins. In order to make its course easy and comfortable, to reduce the risk of complications, the patient should be aware of the peculiarities of the recovery phase. In addition, it is necessary to adhere to some recommendations:
- For several hours after completion of thoracocentesis, you should not leave the hospital. It is advisable to lie down and rest. During 3-4 hours it is necessary to monitor vital signs such as blood pressure, heart rate, blood oxygen saturation.
- If a cough appears, but it does not last long and disappears on its own, you should not worry. If the cough increases, shortness of breath, chest pain, you need to see a doctor as soon as possible.
- Analgesics, non-steroidal anti-inflammatory drugs can be used to reduce post-procedure pain.
- A hematoma may occur in the puncture area. It usually does not require any specific treatment and disappears on its own within a few days.
- It is important to limit physical activity, do not run or jump, and do not lift heavy objects.
- It is advisable to review the diet and drinking regimen.
- The wound after thoracocentesis should be treated twice a day, avoid contact with water.
- It is not recommended to visit swimming pools, beaches, sauna, baths.
If the above recommendations are followed, the development of complications can be avoided.
Thoracocentesis is one of the main procedures for intensive care physicians, intensive care and emergency room staff. Manipulation has many more benefits than possible risks. The development of complications is extremely rare.