Medical expert of the article

New publications
Melanoma
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Melanoma is a malignant skin neoplasm that develops from melanocytes - cells that migrate in the early embryonic period from the neuroectoderm to the skin, eyes, respiratory tract and intestines.
Melanocytes are capable of forming peculiar "nests" of cells with different degrees of differentiation. Externally, clusters of melanocytes appear as nevi (birthmarks). Melanoma was first described in 1806 by René Laennec.
Epidemiology
The incidence rate in all age groups is currently about 14 cases per 100,000 population per year. At the same time, according to estimates by the National Cancer Institute, the probability of developing the disease for the white population of the United States is 1:100. In black people, this tumor is extremely rare, so its risk for this category is not determined.
Melanoma is extremely rare in children: its incidence in them is about 1% of cases of this tumor in all age groups. The incidence of its development increases with age. However, two peaks of incidence of this tumor are distinguished in children: 5-7 and 11-15 years.
Causes melanomas
In the development of melanoma, two main predisposing factors are distinguished - trauma and insolation. Both of these types of impacts provoke malignant degeneration of skin elements. This dictates the need for planned removal of nevi from areas where they are subject to the greatest trauma from clothing and footwear, and also requires giving up excessive sunbathing and solariums.
Other predisposing factors for the development of malignant skin neoplasms are white race (the lighter the skin, the higher the risk), a family history of this tumor, the presence of a large number of nevi on the skin, and for adults, age under 45. Short but intense doses of insolation are more dangerous for melanoma than constant insolation.
As a preventative measure, the most effective is to reduce the time spent in direct sunlight and wear hats and clothing that cover the skin as much as possible; sunscreens are less effective.
Symptoms melanomas
In 70% of cases, melanoma develops from nevi, in 30% - on "clean" areas of the skin. The localization of the neoplasm can be any part of the body. Most often (50% of cases) it occurs on the skin of the extremities, somewhat less often (35%) - in the torso area and least often (25%) on the head and neck.
What does melanoma look like?
- Superficial spreading - develops from an existing nevus, has a slow growth rate over several years. This is the most common form of malignant neoplasm.
- Nodular is a loose node on the skin. Often ulcerates, has a rapid growth rate. It is in 2nd place in frequency after superficial spreading.
- Malignant lentigo (Hutchinson's melanotic freckle) - similar to superficial spreading, typical for elderly people. Usually localized on the face.
- Peripheral lentigo - affects the palms, soles of the feet, and can be localized on the nail bed. Most common in non-whites. The prognosis is usually unfavorable, since the tumor may remain undiagnosed until it reaches a significant size.
There are three early and four late signs of melanoma.
Early signs:
- high growth rates;
- proliferation of one of the areas of skin with its deformation:
- ulceration and spontaneous bleeding.
Late signs:
- the appearance of satellites (intradermal tumor seedings) around the primary tumor:
- enlargement of regional lymph nodes (in case of metastatic lesions);
- tumor intoxication;
- visualization of distant metastases using instrumental methods.
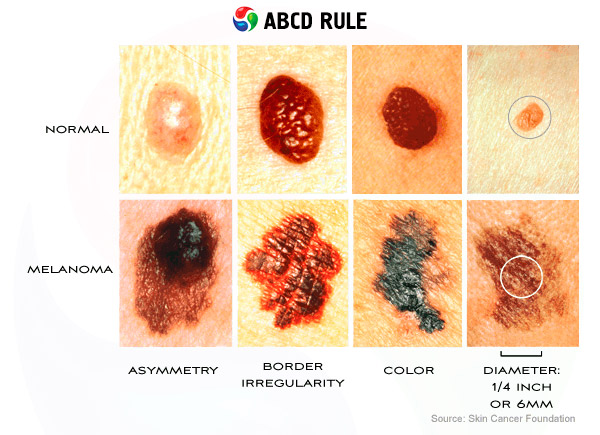
In English-speaking countries, the acronym ABCD is used to remember the signs of a neoplasm:
- A (Assymetry) - asymmetry of shape and pigment distribution. The letter "A" also means that the appearance of the tumor must be assessed.
- B (Borders) - the edges of the cancer often have an irregular star-shaped shape and bleed (Bleed).
- C (Change) - if any characteristics change, the birthmark must be examined for malignancy.
- D (Diameter) - the diameter of most melanomas is greater than 6 mm, although smaller neoplasms are also possible.
Melanoma is characterized by lymphogenous metastasis with damage, primarily, of regional lymph nodes and hematogenous metastasis with damage to the lungs, brain, and other organs. The risk of metastasis increases with an increase in the thickness of the neoplasm and the depth of its invasion into the dermis and subcutaneous tissue.
Where does it hurt?
Stages
When assessing the primary tumor, the depth of cancer invasion into the skin and underlying tissues is important. In clinical practice, the Clark classification (Clark. 1969) is used, which provides for five degrees of invasion.
- Clark's grade I invasion (melanoma in situ) - cancer is located in the epithelium without penetrating the basement membrane.
- Clark's grade II invasion - the neoplasm penetrates the basement membrane and spreads into the papillary layer of the dermis.
- Clark's grade III invasion - cancer spreads into the papillary layer of the dermis, with tumor cells accumulating at the border of the papillary and reticular layers without penetrating into the latter.
- Clark's grade IV invasion - the neoplasm spreads into the reticular layer of the dermis.
- Clark grade V invasion - cancer spreads to subcutaneous fat and other structures.
Breslow (1970) proposed to evaluate the depth of melanoma penetration into the skin and underlying tissues by the thickness of the removed tumor. Both principles (Clark and Breslow) are combined in the classification proposed by the American Joint Committee on Cancer Classification (AJCCS) (while it is recommended to give preference to the criteria according to Breslow).
- Stage Ia - the thickness is 0.75 mm and/or the degree of invasion according to Clark II (pT1), regional (N0) and distant (M0) metastases are absent.
- Stage Ib - thickness is 0.76-1.50 mm and/or the degree of invasion according to Clark III (pT2): N0. M0.
- Stage IIa - thickness 1.51-4.00 mm and/or degree of invasion according to Clark IV (pT3). N0. M0.
- Stage IIb - thickness more than 4.00 mm and/or degree of invasion according to Clark V (pT4); N0, MO.
- Stage III - metastases to regional lymph nodes or metastases in-transit (satellites); any pT, N1 or N2, MO.
- Stage IV - distant metastases: any pT. any N. Ml.
Forms
There are four types of pigmented formations on the skin.
- Non-melanoma-hazardous: true pigmented nevus, intradermal nevus, papillomas, warts, hairy nevus.
- Melanocarcinoma: borderline nevus, blue nevus, giant pigmented nevus.
- On the border of malignancy: juvenile (mixed nevus, Spitz nevus) - does not metastasize, but has a tendency to recur.
- Malignant neoplasm - melanoma.
 [ 17 ]
[ 17 ]
Diagnostics melanomas
A diagnostic feature is a categorical ban on aspiration and incisional biopsy (partial excision of this tumor or suspicious nevus). Such intervention gives impetus to intensive growth and metagassing of the tumor. In relation to melanoma, only complete removal within healthy tissues with subsequent histological examination is permissible. Thermography is a preoperative method for assessing the malignancy of a skin formation. In the presence of a bleeding, ulcerated tumor, it is possible to make an imprint from its surface with subsequent cytological examination.
The diagnosis of possible lymphogenous and hematogenous metastases is based on the standard examination plan for an oncological patient.
[ 18 ], [ 19 ], [ 20 ], [ 21 ]
Mandatory diagnostic tests
- Complete physical examination with assessment of local status
- Clinical blood test
- Clinical urine analysis
- Blood biochemistry (electrolytes, total protein, liver function tests, creatinine, urea, lactate dehydrogenase, alkaline phosphatase, phosphorus-calcium metabolism)
- Coagulogramia
- Thermography
- Ultrasound of the affected area Ultrasound of the abdominal organs and retroperitoneal space
- X-ray of the chest organs in five projections (spinal, two lateral, two oblique)
- ECG
- The final stage is histological verification of the diagnosis. It is possible to make prints from the preparation for cytological examination.
[ 22 ]
Additional diagnostic tests
- In the presence of an ulcerated bleeding tumor - cytological examination of the imprint from the surface of the tumor
- If metastases to the lungs are suspected - CT of the chest organs
- If metastases in the abdominal cavity are suspected - ultrasound, CT of the abdominal cavity
- If brain metastases are suspected - EchoEG and CT of the brain
What do need to examine?
How to examine?
Differential diagnosis
Differential diagnosis of melanoma and non-malignant elements on the skin of a child is often difficult. The diagnostic criteria may include the rapid growth rate characteristic of this type of cancer, outpacing the child's growth, irregular or jagged shape of the tumor edges, often bleeding, and a change in the color of the nevus when it degenerates into a malignant neoplasm. The variability of the color of this tumor also complicates the diagnosis. In addition to the typical brown, its surface may have shades of blue, gray, pink, red, or white.
Who to contact?
Treatment melanomas
The leading method of treatment is radical surgical removal of melanoma - excision to the fascia within healthy tissues with a significant reserve of unchanged skin along the tumor periphery. The reserve of healthy tissues along the periphery is selected depending on the tumor thickness: intraepithelial neoplasm - 5 mm; with a tumor thickness of up to 1 cm - 10 mm; more than 1 cm - 20 mm. When diagnosing regional lymph nodes affected by metastases, lymph node dissection is performed simultaneously with the removal of the primary tumor.
Conservative treatment
Melanoma is considered to be one of the most resistant to chemoradiotherapy neoplasms. However, conservative treatment is used for metastases of this tumor for palliative purposes. In recent years, encouraging results have been obtained with the use of interferon preparations at stages III-IV of the neoplasm.
[ 27 ], [ 28 ], [ 29 ], [ 30 ], [ 31 ], [ 32 ], [ 33 ], [ 34 ]
Tactics in relation to formations
Any skin formation suspicious for melanoma, as well as nevi, in the presence of at least one of the above-mentioned signs of malignancy, must be removed with a scalpel within healthy tissues to the fascia with subsequent histological examination. Cryolaser surgery methods are applicable to unchanged nevi - for cosmetic purposes or when they are localized in areas of potential injury and/or increased insolation on open areas of the skin.
Forecast
The prognosis for melanoma progressively worsens depending on the degree of invasion and the stage of the tumor. The depth of invasion affects the 10-year survival rate as follows: stage I - survival approaches 100%, stage II - 93%, stage III - 90%. stage IV - 67%, stage V - 26%. The dependence of 10-year survival rates on the stage of the process is as follows: at stage I, up to 90% of patients survive, at stage II - up to 70%, at stage III, according to various estimates, from 20 to 40%, at stage IV the prognosis is fatal. By localization, there are groups with a favorable prognosis (head and neck), unfavorable (torso) and uncertain (limbs). It can be considered that more distal localizations are associated with a better prognosis compared to proximal and central ones. Melanoma on an area of the skin usually covered by clothing indicates a less favorable prognosis.