Medical expert of the article

New publications
Examination of cranial nerves. III, IV, VI pairs: oculomotor, block and withdrawal nerves
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

The oculomotor nerve contains motor fibers that innervate the medial, superior, and inferior rectus muscles of the eyeball, the inferior oblique muscle, and the muscle that raises the upper eyelid, as well as autonomic fibers that, interrupted in the ciliary ganglion, innervate the internal smooth muscles of the eye - the sphincter of the pupil and the ciliary muscle. The trochlear nerve innervates the superior oblique muscle, and the abducens nerve - the external rectus muscle of the eyeball.
Causes of diplopia
When collecting anamnesis, it is determined whether the patient has diplopia and, if it is present, how the double objects are located - horizontally (pathology of the VI pair), vertically (pathology of the III pair) or when looking down (lesion of the IV pair). Monocular diplopia is possible with intraocular pathology leading to dispersion of light rays on the retina (with astigmatism, corneal diseases, with incipient cataracts, hemorrhage into the vitreous body), as well as with hysteria; with paresis of the external (striated) muscles of the eye, monocular diplopia does not occur. The sensation of imaginary trembling of objects (oscillopsia) is possible with vestibular pathology and some forms of nystagmus.
 [
[ Eye movements and their study
There are two forms of concomitant eye movements: conjugate (gaze), in which the eyeballs simultaneously turn in the same direction; and vergence, or disconjugate, in which the eyeballs simultaneously move in opposite directions (convergence or divergence).
In neurological pathology, four main types of oculomotor disorders are observed.
- A misalignment of the movements of the eyeballs due to weakness or paralysis of one or more striated muscles of the eye; this results in strabismus and double vision due to the fact that the object being viewed is projected in the right and left eyes not onto similar, but onto disparate areas of the retina.
- Conjugate disorder of conjugate movements of the eyeballs, or concomitant gaze palsies: both eyeballs cease to move voluntarily in one direction or another (to the right, to the left, down or up) in a coordinated manner (jointly); the same movement deficit is detected in both eyes, while double vision and strabismus do not occur.
- Combination of paralysis of the eye muscles and paralysis of gaze.
- Spontaneous pathological movements of the eyeballs, occurring mainly in patients in a coma.
Other types of oculomotor disorders ( concomitant strabismus, internuclear ophthalmoplegia ) are observed less frequently. The listed neurological disorders should be distinguished from congenital imbalance of the tone of the eye muscles ( non-paralytic strabismus or non-paralytic congenital strabismus, ophtophoria), in which the misalignment of the optical axes of the eyeballs is observed both during eye movements in all directions and at rest. Latent non-paralytic strabismus is often observed, in which the images cannot fall on identical places on the retina, but this defect is compensated for by reflex corrective movements of the latent squinting eye (fusion movement). With exhaustion, mental stress or for other reasons, the fusion movement may weaken, and latent strabismus becomes obvious; in this case, double vision occurs in the absence of paresis of the external eye muscles.
Evaluation of parallelism of optical axes, analysis of strabismus and diplopia
The doctor stands in front of the patient and asks him to look straight ahead and into the distance, fixing his gaze on a distant object. Normally, the pupils of both eyes should be in the center of the palpebral fissure. Deviation of the axis of one of the eyeballs inward (esotropia) or outward (exotropia) when looking straight ahead and into the distance indicates that the axes of the eyeballs are not parallel (strabismus), and this is what causes double vision (diplopia). To detect minor strabismus, you can use the following technique: holding a light source (for example, a light bulb) at a distance of 1 m from the patient at eye level, watch for the symmetry of the light reflections from the irises. In the eye whose axis is deviated, the reflection will not coincide with the center of the pupil.
The patient is then asked to fix his gaze on an object that is at eye level (a pen, his own thumb), and to close one eye after the other in turn. If, when closing the "normal" eye, the squinting eye makes an additional movement to maintain fixation on the object ("alignment movement"), then the patient most likely has congenital strabismus, and not paralysis of the eye muscles. With congenital strabismus, the movements of each eyeball, if tested separately, are preserved and performed in full.
The smooth tracking test is assessed. The patient is asked to follow an object with his eyes (without turning his head) that is held at a distance of 1 m from his face and slowly moved horizontally to the right, then to the left, then up and down on each side (the trajectory of the doctor's movements in the air should correspond to the letter "H"). The movements of the eyeballs are monitored in six directions: to the right, to the left, down and up when the eyeballs are diverted in turn to both sides. The patient is asked whether double vision has developed when looking in one direction or another. If diplopia is present, it is determined which direction the double vision increases with movement. If a colored (red) glass is placed in front of one eye, it is easier for a patient with diplopia to distinguish between double images, and for the doctor to find out which image belongs to which eye.
Mild paresis of the external eye muscle does not cause noticeable strabismus, but subjectively the patient already experiences diplopia. Sometimes the patient's report of double vision with a particular movement is enough for the doctor to determine which eye muscle is affected. Almost all cases of newly developed double vision are caused by acquired paresis or paralysis of one or more striated (external, extraocular) eye muscles. As a rule, any recently developed paresis of the extraocular muscle causes diplopia. Over time, visual perception on the affected side slows down, and double vision disappears. There are two main rules that must be taken into account when analyzing a patient's complaints of diplopia in order to determine which muscle of which eye is affected:
- the distance between the two images increases when looking in the direction of action of the paretic muscle;
- the image created by the eye with a paralyzed muscle appears to the patient to be located more peripherally, that is, further away from the neutral position.
In particular, a patient whose diplopia increases when looking to the left can be asked to look at an object on the left and asked which image disappears when the doctor's palm covers the patient's right eye. If the image closest to the neutral position disappears, this means that the open left eye is "responsible" for the peripheral image, and therefore its muscle is defective. Since double vision occurs when looking to the left, the lateral rectus muscle of the left eye is paralyzed.
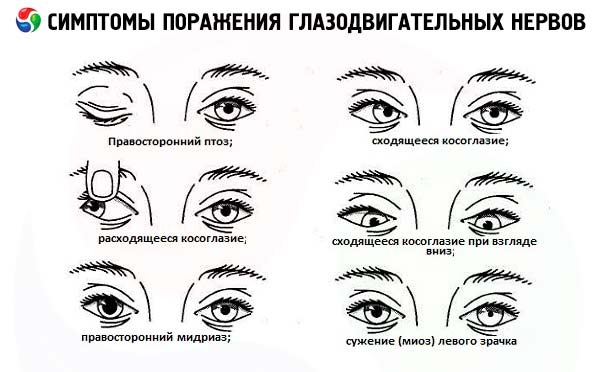
Complete lesion of the oculomotor nerve trunk results in diplopia in the vertical and horizontal planes due to weakness of the superior, medial and inferior rectus muscles of the eyeball. In addition, with complete paralysis of the nerve on the affected side, ptosis (weakness of the muscle that raises the upper eyelid), deviation of the eyeball outward and slightly downward (due to the action of the preserved lateral rectus muscle, innervated by the abducens nerve, and the superior oblique muscle, innervated by the trochlear nerve), dilation of the pupil and loss of its reaction to light (paralysis of the sphincter of the pupil) occur.
Damage to the abducens nerve causes paralysis of the external rectus muscle and, accordingly, medial deviation of the eyeball ( convergent strabismus ). When looking in the direction of the lesion, double vision occurs horizontally. Thus, diplopia in the horizontal plane, not accompanied by ptosis and changes in pupillary reactions, most often indicates damage to the sixth pair. If the lesion is located in the brainstem, in addition to paralysis of the external rectus muscle, paralysis of the horizontal gaze also occurs.
Damage to the trochlear nerve causes paralysis of the superior oblique muscle and is manifested by limited downward movement of the eyeball and complaints of vertical double vision, which is most pronounced when looking down and in the direction opposite to the lesion. Diplopia is corrected by tilting the head toward the shoulder on the healthy side.
The combination of paralysis of the eye muscles and gaze paralysis indicates damage to the structures of the pons or midbrain. Double vision, which intensifies after physical exertion or by the end of the day, is typical of myasthenia gravis.
With a significant decrease in visual acuity in one or both eyes, the patient may not notice diplopia even in the presence of paralysis of one or more extraocular muscles.
Assessment of coordinated eye movements
Gaze palsy is caused by supranuclear disorders, not by damage to the 3rd, 4th, or 6th pairs of cranial nerves. Normally, gaze is a friendly conjugated movement of the eyeballs, i.e. their coordinated movements in one direction. There are two types of conjugated movements: saccades and smooth pursuit. Saccades are very precise and fast (about 200 ms) phase-tonic movements of the eyeballs, which normally occur either during a voluntary look at an object (on command "look to the right", "look to the left and up", etc.), or reflexively, when a sudden visual or auditory stimulus causes the eyes (usually the head) to turn toward this stimulus. Cortical control of saccades is performed by the frontal lobe of the contralateral hemisphere.
The second type of conjugated eye movements is smooth tracking: when an object moves and enters the visual field, the eyes involuntarily fixate on it and follow it, trying to keep the image of the object in the zone of the clearest vision, that is, in the area of the yellow spots. These eye movements are slower than saccades and, compared to them, are more involuntary (reflexive). Their cortical control is carried out by the parietal lobe of the ipsilateral hemisphere.
Gaze disorders (if nuclei 3, 4 or 6 pairs are not affected) are not accompanied by a disorder of isolated movements of each eyeball separately and do not cause diplopia. When examining gaze, it is necessary to find out whether the patient has nystagmus, which is detected using the smooth pursuit test. Normally, the eyeballs move smoothly and in unison when tracking an object. The occurrence of jerky twitching of the eyeballs (involuntary corrective saccades) indicates a disorder of the ability to smooth tracking (the object immediately disappears from the area of best vision and is found again using corrective eye movements). The patient's ability to hold the eyes in an extreme position when looking in different directions is checked: to the right, to the left, up and down. Pay attention to whether the patient develops gaze-induced nystagmus when looking away from the middle position, i.e. nystagmus that changes direction depending on the direction of gaze. The fast phase of gaze-induced nystagmus is directed toward the gaze (when looking to the left, the fast component of nystagmus is directed to the left, when looking to the right - to the right, when looking up - vertically upward, when looking down - vertically downward). Impaired smooth tracking ability and the occurrence of gaze-induced nystagmus are signs of damage to the cerebellar connections with neurons in the brainstem or central vestibular connections, and may also be a consequence of the side effects of anticonvulsants, tranquilizers, and some other drugs. If the lesion is in the occipito-parietal region, regardless of the presence or absence of hemianopsia, reflex slow tracking eye movements toward the lesion are limited or impossible, but voluntary movements and movements on command are preserved (i.e., the patient can make voluntary eye movements in any direction, but cannot follow an object moving toward the lesion). Slow, fragmented, dysmetric pursuit movements are observed in supranuclear palsy and other extrapyramidal disorders.
To test voluntary eye movements and saccades, the patient is asked to look to the right, left, up and down. The time required to start performing the movements, their accuracy, speed and smoothness are assessed (a slight sign of dysfunction of the concomitant eye movements in the form of their "stumbling" is often detected). The patient is then asked to alternately fix his gaze on the tips of two index fingers, which are located at a distance of 60 cm from the patient's face and approximately 30 cm from each other. The accuracy and speed of voluntary eye movements are assessed.
Saccadic dysmetria, in which voluntary gaze is accompanied by a series of jerky, jerky eye movements, is characteristic of damage to the cerebellar connections, although it can also occur with pathology of the occipital or parietal lobes of the brain - in other words, the inability to reach a target with the gaze (hypometria) or the gaze "skipping" over the target due to excessive amplitude of eye movements (hypermetria), corrected with the help of saccades, indicate a deficiency in coordination control. Marked slowness of saccades can be observed in diseases such as hepatocerebral dystrophy or Huntington's chorea. Acute damage to the frontal lobe (stroke, traumatic brain injury, infection) is accompanied by paralysis of horizontal gaze in the direction opposite to the lesion. Both eyeballs and the head are deviated toward the lesion (the patient "looks at the lesion" and turns away from the paralyzed limbs) due to the intact function of the opposite center of head and eye rotation to the side. This symptom is temporary and lasts only a few days, since the gaze imbalance is soon compensated. The ability to reflexively track with frontal gaze palsy may persist. Horizontal gaze palsy with frontal lobe damage (cortex and internal capsule) is usually accompanied by hemiparesis or hemiplegia. When the pathological lesion is localized in the midbrain roof region (pretectal lesions involving the posterior commissure of the brain, which is part of the epithalamus), vertical gaze palsy develops, combined with impaired convergence ( Parinaud syndrome ); upward gaze is usually affected to a greater extent. When the pons and medial longitudinal fasciculus, which provides lateral concomitant movements of the eyeballs at this level, are affected, horizontal gaze paralysis occurs toward the lesion (the eyes are diverted to the side opposite the lesion, the patient "turns away" from the brainstem lesion and looks at the paralyzed limbs). Such gaze paralysis usually persists for a long time.
Evaluation of disconjugated eye movements (convergence, divergence)
Convergence is tested by asking the patient to focus on an object that is moving toward his eyes. For example, the patient is asked to fix his gaze on the tip of a mallet or index finger, which the doctor smoothly brings to the bridge of his nose. When the object approaches the bridge of the nose, the axes of both eyeballs normally turn toward the object. At the same time, the pupil narrows, the ciliary muscle relaxes, and the lens becomes convex. Due to this, the image of the object is focused on the retina. This reaction in the form of convergence, pupil narrowing, and accommodation is sometimes called the accommodative triad. Divergence is the reverse process: when the object is removed, the pupil dilates, and the contraction of the ciliary muscle causes the lens to flatten.
If convergence or divergence is impaired, horizontal diplopia occurs when looking at nearby or distant objects, respectively.
Convergence palsy occurs when the pretectal area of the midbrain roof is affected at the level of the superior colliculi of the lamina quadrigemina. It may be associated with upward gaze palsy in Parinaud's syndrome. Divergence palsy is usually caused by bilateral damage to the 6th pair of cranial nerves.
The isolated pupillary response to accommodation (without convergence) is tested in each eyeball separately: the tip of a neurological hammer or finger is placed perpendicular to the pupil (the other eye is closed) at a distance of 1-1.5 m, then quickly brought closer to the eye, while the pupil narrows. Normally, the pupils react vividly to light and convergence with accommodation.
Spontaneous pathological movements of the eyeballs
Spontaneous rhythmic gaze disorder syndromes include oculogyric crises, periodic alternating gaze, gaze "ping-pong" syndrome, ocular bobbing, ocular dipping, alternating oblique deviation, periodic alternating gaze deviation, etc. Most of these syndromes develop with severe brain damage and are observed mainly in patients in a coma.
- Oculogyric crises are sudden upward and, less commonly, downward deviations of the eyeballs that develop and persist for several minutes to several hours. They are observed in cases of intoxication with neuroleptics, carbamazepine, lithium preparations; in cases of brainstem encephalitis, third ventricular glioma, traumatic brain injury, and some other pathological processes. An oculogyric crisis should be distinguished from tonic upward gaze deviation, sometimes observed in comatose patients with diffuse hypoxic brain damage.
- The "ping-pong" syndrome is observed in patients in a comatose state; it consists of periodic (every 2-8 seconds) simultaneous deviation of the eyes from one extreme position to another.
- In patients with severe damage to the pons or posterior cranial fossa structures, ocular bobbing is sometimes observed - rapid jerky downward movements of the eyeballs from a mid-position followed by a slow return to the central position. Horizontal eye movements are absent.
- "Ocular dipping" is a term used to describe slow downward movements of the eyeballs, followed after a few seconds by a rapid return to their original position. Horizontal eye movements are maintained. The most common cause is hypoxic encephalopathy.
Pupils and eye slits
The reactions of the pupils and eye slits depend not only on the function of the oculomotor nerve - these parameters are also determined by the state of the retina and optic nerve, which make up the afferent part of the reflex arc of the pupil's reaction to light, as well as the sympathetic effect on the smooth muscles of the eye. Nevertheless, pupillary reactions are examined when assessing the state of the 3rd pair of cranial nerves.
Normally, the pupils are round and equal in diameter. Under normal room lighting, the pupil diameter can vary from 2 to 6 mm. A difference in pupil size (anisocoria) of no more than 1 mm is considered normal. To check the direct reaction of the pupil to light, the patient is asked to look into the distance, then a pocket flashlight is quickly turned on and the degree and stability of the constriction of the pupil of this eye is assessed. The turned-on bulb can be brought to the eye from the side, from the temporal side, to exclude the accommodative reaction of the pupil (its constriction in response to the approach of an object). Normally, when illuminated, the pupil constricts, this constriction is stable, that is, it remains the entire time the light source is near the eye. When the light source is removed, the pupil dilates. Then the consensual reaction of the other pupil is assessed, which occurs in response to illumination of the eye being examined. Thus, it is necessary to illuminate the pupil of one eye twice: during the first illumination, we look at the reaction of the illuminated pupil to light, and during the second illumination, we observe the reaction of the pupil of the other eye. The pupil of the unilluminated eye normally constricts at exactly the same rate and to the same extent as the pupil of the illuminated eye, that is, normally both pupils react in the same way and simultaneously. The test of alternate pupil illumination allows us to detect damage to the afferent part of the reflex arc of the pupillary reaction to light. Illuminate one pupil and note its reaction to light, then quickly move the lamp to the second eye and again evaluate the reaction of its pupil. Normally, when the first eye is illuminated, the pupil of the second eye initially constricts, but then, at the moment of moving the lamp, it slightly dilates (a reaction to the removal of illumination consistent with the first eye) and, finally, when a beam of light is directed at it, it constricts again (a direct reaction to light). If, during the second stage of this test, when the second eye is directly illuminated, its pupil does not constrict but continues to dilate (paradoxical reaction), this indicates damage to the afferent pathway of the pupillary reflex of this eye, i.e., damage to its retina or optic nerve. In this case, direct illumination of the second pupil (the pupil of the blind eye) does not cause it to constrict. However, it continues to dilate in concert with the first pupil in response to the cessation of illumination of the latter.
To test the pupillary reflexes of both eyes for convergence and accommodation, the patient is asked to first look into the distance (for example, at the wall behind the doctor), and then move his gaze to a nearby object (for example, at the tip of a finger held directly in front of the patient's nose). If the pupils are narrow, the room is darkened before the test. Normally, fixation of the gaze on an object close to the eyes is accompanied by a slight narrowing of the pupils of both eyes, combined with convergence of the eyeballs and an increase in the convexity of the lens (accommodative triad).
Thus, normally the pupil constricts in response to direct illumination (direct pupillary response to light); in response to illumination of the other eye (companionate pupillary response to light); when focusing the gaze on a nearby object. Sudden fright, fear, pain cause dilation of the pupils, except in cases where the sympathetic fibers to the eye are interrupted.

Signs of damage
By assessing the width of the palpebral fissures and the protrusion of the eyeballs, one can detect exophthalmos - protrusion of the eyeball from the orbit and from under the eyelid. Exophthalmos can be most easily detected by standing behind a seated patient and looking down at his eyeballs. The causes of unilateral exophthalmos may be a tumor or pseudotumor of the orbit, thrombosis of the cavernous sinus, carotid-cavernous fistula. Bilateral exophthalmos is observed in thyrotoxicosis (unilateral exophthalmos in this condition occurs less often).
The position of the eyelids is assessed at different viewing directions. Normally, when looking straight ahead, the upper eyelid covers the upper edge of the cornea by 1-2 mm. Ptosis (drooping) of the upper eyelid is a common pathology, which is usually accompanied by constant contraction of the frontal muscle due to the patient's involuntary attempt to keep the upper eyelid raised.
Drooping of the upper eyelid is most often caused by damage to the oculomotor nerve; congenital ptosis, which can be unilateral or bilateral; Bernard-Horner syndrome; myotonic dystrophy; myasthenia; blepharospasm; eyelid edema due to injection, trauma, venous stasis; age-related tissue changes.
- Ptosis (partial or complete) may be the first sign of oculomotor nerve damage (develops due to weakness of the muscle that raises the upper eyelid). It is usually combined with other signs of damage to the 3rd pair of cranial nerves (ipsilateral mydriasis, lack of pupillary response to light, impaired upward, downward and inward movements of the eyeball).
- In Bernard-Horner syndrome, narrowing of the palpebral fissure and ptosis of the upper and lower eyelids are caused by functional insufficiency of the smooth muscles of the lower and upper eyelid cartilages (tarsal muscles). Ptosis is usually partial and unilateral. It is combined with miosis caused by insufficiency of the pupil dilator function (due to a defect in sympathetic innervation). Miosis is most pronounced in the dark.
- Ptosis in myotonic dystrophy (dystrophic myotonia) is bilateral and symmetrical. The pupil size is unchanged, their reaction to light is preserved. There are other signs of this disease.
- In myasthenia, ptosis is usually partial, asymmetrical, and its severity can vary significantly throughout the day. Pupillary reactions are not impaired.
- Blepharospasm (involuntary contraction of the orbicularis oculi muscle) is accompanied by partial or complete closure of the palpebral fissure. Mild blepharospasm can be confused with ptosis, but with the former, the upper eyelid periodically actively rises and there is no contracture of the frontal muscle.
Irregular attacks of pupil dilation and contraction, lasting for several seconds, are referred to as "hippus" or "undulation". This symptom may occur with metabolic encephalopathy, meningitis, and multiple sclerosis.
Unilateral mydriasis (pupil dilation) combined with ptosis and paresis of the external muscles is observed with damage to the oculomotor nerve. Pupil dilation is often the first sign of damage to the oculomotor nerve when the nerve trunk is compressed by an aneurysm and when the brain stem is dislocated. Conversely, with ischemic lesions of the 3rd pair (for example, in diabetes mellitus), the efferent motor fibers going to the pupil are usually not affected, which is important to take into account in differential diagnosis. Unilateral mydriasis that is not combined with ptosis and paresis of the external muscles of the eyeball is not characteristic of damage to the oculomotor nerve. Possible causes of this disorder include drug-induced paralytic mydriasis that occurs with local use of atropine solution and other M-anticholinergics (in this case, the pupil stops constricting in response to the use of a 1% solution of pilocarpine); Adie pupil; spastic mydriasis caused by contraction of the pupillary dilator when the sympathetic structures innervating it are irritated.
Adie pupil, or pupillotonia, is usually observed on one side. Typically, the pupil on the affected side is dilated ( anisocoria ) and its abnormally slow and prolonged (myotonic) response to light and convergence with accommodation. Since the pupil eventually responds to light, anisocoria gradually decreases during the neurological examination. Denervation hypersensitivity of the pupil is typical: after instillation of 0.1% pilocarpine solution into the eye, it sharply narrows to a pinpoint size.
Pupillotonia is observed in a benign disease (Holmes-Adie syndrome), which is often familial, occurs more often in women aged 20-30 years and, in addition to the “tonic pupil”, can be accompanied by a decrease or absence of deep reflexes from the legs (less often from the arms), segmental anhidrosis (local sweating disorder) and orthostatic arterial hypotension.
In Argyll Robertson syndrome, the pupil constricts when fixing the gaze at a close distance (accommodation response is preserved), but does not react to light. Argyll Robertson syndrome is usually bilateral, combined with an irregular pupil shape and anisocoria. During the day, the pupils have constant sizes, do not respond to instillation of atropine and other mydriatics. This syndrome is observed in lesions of the midbrain tegmentum, for example, in neurosyphilis, diabetes mellitus, multiple sclerosis, pineal tumor, severe craniocerebral trauma with subsequent expansion of the Sylvian aqueduct, etc.
A narrow pupil (due to paresis of the dilator pupillae), combined with partial ptosis of the upper eyelid (paresis of the muscle of the superior cartilage of the eyelid), anophthalmos and impaired sweating on the same side of the face indicates Bernard-Horner syndrome. This syndrome is caused by impaired sympathetic innervation of the eye. The pupil does not dilate in the dark. Bernard-Horner syndrome is most often observed in infarctions of the medulla oblongata (Wallenberg-Zakharchenko syndrome) and the pons, brainstem tumors (interruption of the central descending sympathetic pathways coming from the hypothalamus); spinal cord damage at the level of the ciliospinal center in the lateral horns of the gray matter of segments C 8 -Th 2; in case of complete transverse damage to the spinal cord at the level of these segments (bilateral Bernard-Horner syndrome, combined with signs of impaired sympathetic innervation of organs located below the level of damage, as well as with conduction disorders of voluntary movements and sensitivity); diseases of the apex of the lung and pleura (Pancoast tumor, tuberculosis, etc.); in case of damage to the first thoracic spinal root and lower trunk of the brachial plexus; aneurysm of the internal carotid artery; tumors in the area of the jugular foramen, cavernous sinus; tumors or inflammatory processes in the orbit (interruption of postganglionic fibers running from the superior cervical sympathetic ganglion to the smooth muscles of the eye).
When the sympathetic fibers to the eyeball are irritated, symptoms occur that are the “opposite” of the Bernard-Horner symptom: dilation of the pupil, widening of the palpebral fissure, and exophthalmos (Pourfur du Petit syndrome).
In case of unilateral loss of vision caused by interruption of the anterior sections of the visual pathway (retina, optic nerve, chiasm, optic tract), the direct reaction of the pupil of the blind eye to light disappears (since the afferent fibers of the pupillary reflex are interrupted), as well as the consensual reaction of the pupil of the second, healthy eye to light. The pupil of the blind eye is capable of constricting when the pupil of the healthy eye is illuminated (i.e. the consensual reaction to light in the blind eye is preserved). Therefore, if the flashlight bulb is moved from the healthy to the affected eye, one can observe not a constriction, but, on the contrary, a dilation of the pupil of the affected eye (as a consensual response to the ceased illumination of the healthy eye) - Marcus Gunn's symptom.
During the examination, attention is also paid to the color and uniformity of the iris. On the side where the sympathetic innervation of the eye is impaired, the iris is lighter (Fuchs' symptom), and there are usually other signs of Bernard-Horner syndrome. Hyaline degeneration of the pupillary edge of the iris with depigmentation is possible in elderly people as a manifestation of the involutional process. Axenfeld's symptom is characterized by depigmentation of the iris without accumulation of hyaline in it, it is observed in disorders of sympathetic innervation and metabolism. In hepatocerebral dystrophy, copper is deposited along the outer edge of the iris, which is manifested by yellowish-green or greenish-brown pigmentation (Kayser-Fleischer ring).