Medical expert of the article

New publications
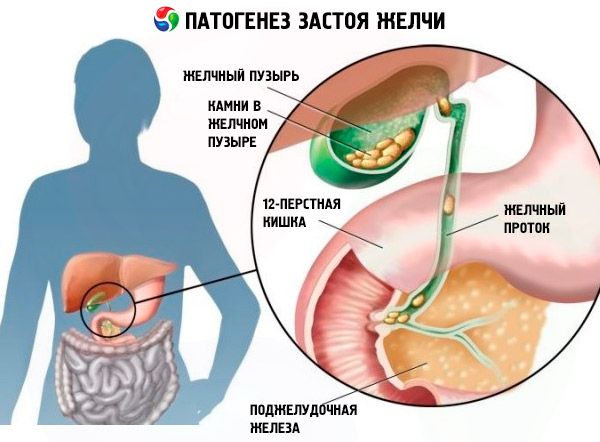
Bile stasis
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Among digestive pathologies, gastroenterologists distinguish bile stasis, which is a syndrome indicating problems in the functioning of the hepatobiliary system: the liver, which produces bile, the gallbladder (a bile depot where it becomes more concentrated) or the biliary transport network (intra- and extrahepatic bile ducts).
Why is bile stagnation dangerous?
This pathology is diagnosed more and more often, so you should know how dangerous bile stagnation is for the body. After eating, the fats contained in it begin to emulsify, but in order for lipids to be digested and lipophilic vitamins to be fully absorbed, in addition to gastric juice and pancreatic enzymes, bile acids and their salts are needed - the main components of bile. From the gallbladder, they enter the duodenum, where the process of emulsification and colloidal hydrolysis of fats continues.
If bile stagnates (i.e. does not enter the intestinal section of the digestive tract), the activity of the intestinal enzyme lipase decreases, and fats are not completely broken down and enter the blood in significant quantities, complicating the transformation of glucose into glycogen (which is fraught with the development of diabetes). Stagnation of bile is dangerous due to the reduction in the removal of excess cholesterol, which is present in the bile itself: it causes hypercholesterolemia (high cholesterol in the blood) and accelerates the development of atherosclerosis.
Stagnation of bile in the gallbladder often leads to its inflammation (secondary cholecystitis) or cholelithiasis. It is in the presence of stones in the gallbladder that acute and chronic cholecystitis with bile stagnation most often develops.
Gastritis and bile stasis can be diagnosed simultaneously when the mucous membrane of the esophagus and stomach is exposed to bile acids that enter there “backwards” from the duodenum – with chronic duodenogastric reflux (arising from weakness of the cardiac sphincter of the esophagus).
Stagnation of bile in the ducts can lead to so-called sclerosing cholangitis – inflammation, fibrosis and strictures of the bile ducts.
When the circulation of bile acids in the gastrointestinal tract is disrupted, the absorption of fats (fat malabsorption) and fat-soluble vitamins is reduced: retinol (vitamin A), ergocalciferol (vitamin D), tocopherol (vitamin E), phylloquinones (vitamins of group K). The most well-known consequences and complications of vitamin A deficiency are deterioration of twilight vision, and vitamin D deficiency is osteomalacia (when a decrease in bone mineralization leads to their softening). At the same time, the simultaneous deficiency of vitamins A and D interferes with the absorption of calcium, which makes bone tissue even less dense, i.e. osteoporosis develops. And vitamin K deficiency threatens to reduce blood clotting and the occurrence of hemorrhagic diathesis and bleeding.
A very real threat posed by chronic bile stagnation is increased intestinal acidity, because bile, due to the presence of calcium cations, reduces the acidity of the stomach contents saturated with gastric juice, which passes into the intestinal stage of digestion. With bile stagnation (cholestasis), an acid-base imbalance in the gastrointestinal tract is observed, and the result of acidification is ascites (dropsy) and poor intestinal function due to the proliferation of pathogenic microbes.
When there is prolonged stagnation of bile in the liver, an increase in the level of chenodeoxycholic bile acid produced in the liver can lead to the death of hepatocytes and focal necrosis of the parenchyma. This is a very serious complication, since the liver is responsible for very important functions.
If there is stagnation of bile in the intestine, the toxicity of conjugated metabolic products and exogenous toxins (including bacterial origin) increases. Consequences and complications also concern the synthesis of hormones, which is significantly reduced, since lipids are needed for their production.
Epidemiology
According to research, up to 70% of cases are due to extrahepatic bile stasis. This syndrome is more common among women, especially during pregnancy. Due to the immaturity of the liver enzyme system, newborns and children in the first two to three years of life are more prone to bile stasis.
Causes bile stasis
In clinical gastroenterology, the causes of bile stagnation are associated with the destruction of hepatocytes due to primary biliary or alcoholic cirrhosis of the liver (hepatocellular congestion); with liver damage due to infections or parasites (viral hepatitis A, C, G; hepatic tuberculosis; amebiasis, opisthorchiasis, giardiasis, etc.); with the effect on the liver of various toxins or components of drugs (including sulfonamides, penicillin antibiotics, analgesics, hormones).
As experts note, bile stagnation in the liver occurs if there is a liver cyst, malignant neoplasms or metastases.
The reasons why bile stagnation occurs in the gallbladder and bile ducts include:
- gallbladder dyskinesia;
- gallstones;
- kink of the gallbladder;
- tumors of the gallbladder or bile ducts;
- inflammation in the area of the neck of the gallbladder;
- cystic formations of the common bile duct or its compression by a cyst localized in the pancreas;
- compression and narrowing of the initial section of the common hepatic duct (Mirizzi syndrome);
- dysfunction of the valve system of the biliary tract (sphincter of Oddi, Lutkens, Mirizzi, Heister);
- failures of the endocrine and paracrine mechanisms of the gastroduodenal stage of digestion associated with an imbalance of secretin, cholecystokinin, neurotensin and other intestinal hormones.
Risk factors
Hypodynamia and bile stasis are closely related: the less a person moves, the slower the metabolic processes in his body are and the higher his risk of developing biliary dyskinesia or the formation of gallstones.
And specialists call bile stagnation after gallbladder removal part of the typical postoperative consequences that arise due to the formation of scar tissue that narrows the lumen of the bile ducts.
An important dietary risk factor for biliary obstruction due to gallstones may be excessive sugar consumption, as well as fatty foods that cause bile stasis.
Also real risk factors for bile stasis are alcohol abuse, overeating, obesity, and inherited genetic predisposition to metabolic disorders.
Pathogenesis
The pathogenesis of bile stagnation in intrahepatic ducts is associated with infections, endocrine disorders, genetic metabolic disorders (thyrotoxicosis, liver or intestinal amyloidosis) and iatrogenic effects. And the pathogenesis of bile stagnation in extrahepatic ducts (cystic, common hepatic and common bile) is due to changes in the composition of bile and an increase in its lithogenicity, anomalies of the bile ducts and their partial or complete obstruction.
 [ 12 ]
[ 12 ]
Symptoms bile stasis
First of all, it should be borne in mind that this condition can be asymptomatic. And the intensity and sequence in which the symptoms of bile stagnation appear depend on the specific cause and individual characteristics of the hepatobiliary system of the body. But the first signs are skin itching and changes in feces and urine. It is believed that skin itching with bile stagnation is a reaction to an increase in the level of bile acids in the blood plasma, where they get as a result of damage to liver cells by chenodeoxycholic acid.
Stool with bile stagnation has a characteristic discoloration due to the disruption of the elimination of the bile pigment bilirubin (which is normally oxidized into stercobilin, which colors the stool brown and the urine straw-yellow). Urine with bile stagnation, on the contrary, becomes dark, because the level of urobilin (urine stercobilin) increases in it.
Constipation and diarrhea with bile stagnation are typical symptoms of this condition. Since bile acids play an important role in intestinal motility, their contraction in the intestinal lumen leads to constipation. And diarrhea with stagnation is associated either with an increased content of unsplit fats in feces (steatorrhea) or with changes in the intestinal microflora.
Changes in skin color – jaundice – are not observed in all patients, but with sufficiently high plasma levels of conjugated bilirubin, the skin, sclera, and mucous membranes become yellow. Yellow spots (xanthelasma) may appear on the eyelids, and focal skin lesions with cholesterol inclusions (xanthomas) may appear around the eyes, in the palmar folds, under the breast, on the neck, and in the diaper area of infants.
The characteristic pains associated with bile stasis are dull, paroxysmal pains localized in the right upper quadrant of the abdomen (in the hypochondrium); they can radiate upward and backward (to the collarbone, shoulder, or shoulder blade); acute attacks in the form of colic are possible.
Heartburn due to bile stagnation is often accompanied by a constant feeling of bitterness in the mouth, and dry mouth is also typical of bile stagnation. Bile helps break down proteins and nitrogenous bases contained in food, and bad breath due to bile stagnation occurs due to the deterioration of digestion and absorption of proteins. By the way, bile stagnation after gallbladder removal often manifests itself as bitter belching of bile.
Fever - temperature with bile stagnation - is evidence of infection, for example, phlegmonous or gangrenous cholecystitis with cholelithiasis. High temperature can be caused by sepsis, which develops after endoscopic diagnostic manipulations.
In addition, symptoms of bile stasis include nausea and vomiting; dizziness and a feeling of general weakness; enlarged liver (hepatomegaly); increased pressure in the portal vein system leading to the liver. With bile stasis in children, a deficiency of essential polyunsaturated fatty acids (linoleic, linolenic, arachidonic) can lead to growth retardation, damage to the peripheral nervous system, dermatitis. Alopecia, that is, hair loss due to bile stasis, is also a result of triglyceride deficiency.
Bile stasis during pregnancy
Clinical studies of recent years have shown that bile stasis during pregnancy is initiated by estrogens, which regulate most processes in the body of the expectant mother. Thus, pregnant women produce more secretin hormone, and therefore more bile. But at the same time, the secretion of growth hormone somatotropin (STH) increases, and it blocks the hormone cholecystokinin, which is responsible for the contraction of the gallbladder and common bile duct.
Bile stasis in pregnancy (idiopathic jaundice of pregnancy or obstetric cholestasis) most often presents with excruciating pruritus (especially of the palms of the hands and soles of the feet) in the middle of the second or third trimester, as estrogen levels peak. In addition, serum aminotransferase, alkaline phosphatase, and unconjugated bile acid levels are significantly elevated; other symptoms are rare. Spontaneous relief and resolution of symptoms occurs within two to three weeks after delivery.
The epidemiology of bile stasis in pregnant women shows a 0.4-1% prevalence of this condition in women in most areas of Central and Western Europe and North America, while in Scandinavian and Baltic countries this figure reaches 1-2%, and in some regions of Latin America – up to 5-15%.
In this case, the following consequences and complications of bile stasis in pregnant women are noted: premature birth (20-60%), meconium staining in the amniotic fluid (more than 25%), fetal bradycardia (14%), fetal distress (22-40%), fetal loss (0.4-4%).
Stagnation of bile occurs in 45-70% of women and occurs during all subsequent pregnancies.
By the way, with itching and the absence of jaundice, bile stasis and allergies are often not differentiated, and patients turn to dermatologists who cannot help them in any way.
[ 13 ], [ 14 ], [ 15 ], [ 16 ]
Stagnation of bile in a child
There are many reasons that can cause bile stasis in a child, including:
- absence of gallbladder (agenesis);
- duplication of the gallbladder (complete or rudimentary);
- deepening of the gallbladder into the liver parenchyma;
- diverticulum (protrusion of part of the wall) of the gallbladder;
- congenital dilation of the bile ducts inside the liver (Caroli syndrome);
- congenital strictures in the presence of a cyst of the common bile duct;
- a fairly common congenital (caused by mutations in the gene of serine digestive enzymes) disorder of the synthesis of hepatic alpha-1-antitrypsin;
- genetically determined reduction or complete absence of intrahepatic ducts (biliary atresia);
- heterogeneous disorder of bile formation - progressive familial intrahepatic congestion (Byler's disease); pathogenesis is associated with mutations in the genes of the hepatocellular transport system; is diagnosed in one newborn out of 50-90 thousand.
Read also – Congenital anomalies of the biliary tract
In addition, bile stasis in a preschool and school-age child may have the same causes as in adults (see above). But most often, the etiology is associated with impaired gallbladder motility and functional disorders of the biliary tract.
Where does it hurt?
Diagnostics bile stasis
In clinical practice, the diagnosis of bile stasis is carried out by means of an examination, during which, in addition to collecting anamnesis and examining the patient, the following tests are taken:
- general blood test;
- biochemical blood test for levels of bilirubin, cholesterol, bile acids, 5-nucleotidase, aminotransferases, as well as liver enzymes - alkaline phosphatase, leucine aminopeptidase (LAP) and gamma-glutamyl transpeptidase (GGT);
- blood test for antibodies to parasites;
- urine analysis for urobilin;
- stool analysis for parasitic infestations.
Instrumental diagnostics of pathologies associated with bile stasis is carried out using:
- ultrasound examination (ultrasound) of the gallbladder, liver and small intestine;
- dynamic cholescintigraphy;
- esophagogastroduodenoscopy;
- radioisotope hepatobiliary scintigraphy;
- endoscopic cholangiography;
- endoscopic retrograde radiography of the bile ducts and pancreas (ERCP).
- CT or MRI of the digestive organs.
What do need to examine?
What tests are needed?
Differential diagnosis
The task that differential diagnostics solves is to clearly distinguish between problems of the hepatobiliary system that cause bile stasis and hereditary defects of bile excretion (Rotor, Dubin-Johnson syndromes), unconjugated hyperbilirubinemia (Gilbert syndrome), parenchymatous jaundice, hematuria, carotenemia, erythropoietic porphyria, hepatic form of infectious mononucleosis, etc.
Who to contact?
Treatment bile stasis
The principles on which the complex treatment of bile stasis is based: if the cause can be eliminated, the treatment is etiological, including surgical treatment; when the cause cannot be eliminated, the therapy is symptomatic with the maximum possible impact on individual pathogenetic components.
If bile stagnation in the gallbladder or liver has not caused duct obstruction, then drugs based on ursodeoxycholic acid, which is part of bile, are used. These include the hepatoprotective drug with choleretic (increasing bile synthesis) and choleretic effects Ursofalk (Ursochol, Holacid, Ursosan, Ursoliv, Ukrliv, Choludexan and other trade names) in the form of capsules and suspension for oral administration. This drug also reduces the production of cholesterol and its absorption in the small intestine, which reduces the likelihood of the formation of cholesterol-containing stones. Capsules and suspension are prescribed at 10-15-20 mg per kilogram of body weight per day (the specific dose is determined by the doctor); treatment is long-term.
Ursofalk should not be used in cases of liver cirrhosis, acute cholecystitis or cholangitis, calcified gallstones and its dyskinesia, as well as in cases of obvious functional insufficiency of the liver, pancreas or kidneys. And among the side effects of ursodeoxycholic acid, the occurrence of pain in the upper abdomen, moderate diarrhea, and the formation of bile calcifications are noted.
Cholagogues are almost always prescribed for bile stasis, such as Allochol, Hofitol (Artichol, Cynarix), Holiver, Odeston (Gimecromon, Cholestil, Holstamin forte, etc.). The most effective hepatoprotector is considered to be the drug Ademetionine (Geptor, Heptral).
Allochol (consisting of dry bile, nettle and garlic extracts and activated carbon) promotes bile production, so it is not used in acute forms of hepatitis, liver dysfunction and obstructive jaundice. Allochol tablets are taken after meals - 2 tablets three times a day. In some people, the drug can cause skin allergies and diarrhea.
Hofitol tablets (and solutions for oral and parenteral administration) contain artichoke leaf extract, which promotes bile flow, increases diuresis and cholesterol metabolism. The drug in tablet form is taken three times a day, 1-2 tablets (before meals), the solution - 2.5 ml (for children - 0.6-1.25 ml). Hofitol can cause urticaria; it is contraindicated for use in gallstones, biliary obstruction and liver failure.
And the choleretic agent Holiver, in addition to artichoke extract, contains extracts of bile and turmeric, stimulating the synthesis of bile acids and the release of hepatic bile. The product is also effective for constipation associated with intestinal dysbiosis and flatulence. Contraindications are similar to Hofitol; the standard dosage is 2-3 tablets 3 times a day (before or after meals).
Choleretic tablets Odeston (based on 7-hydroxy-4-methylcoumarin) not only accelerate the circulation of bile, but also relieve spasms. It is recommended to take one tablet (0.2 g) three times a day for 10-14 days, half an hour before meals. Odeston is contraindicated in nonspecific ulcerative colitis and any gastrointestinal diseases with ulcers, obstruction of the bile ducts, hemophilia; it is not used to treat children. Side effects of the drug are diarrhea, epigastric pain, increased intestinal gas formation.
The drug Ademetionine (S-adenosyl-methionine) helps to normalize liver function and metabolism. Prescribed 2-3 tablets per day; contraindications of the drug concern individual intolerance, use in the treatment of children and pregnant women (in the first and second trimesters). A possible side effect is discomfort in the hypochondrium.
In addition, in the treatment of bile stagnation, pharmacy choleretic herbal teas are used. For example, choleretic tea No. 2 (flowers of sandy immortelle, yarrow herb, peppermint leaves, coriander seeds) or tea No. 3 (flowers of calendula, tansy and chamomile and mint leaves). A decoction is prepared from dry raw materials - a tablespoon per glass of water (boil for no more than 10 minutes and leave for half an hour in a closed container, strain and add boiled water to the original volume). Choleretic teas should be used after consulting a doctor; drink decoctions before meals twice a day - 100 ml.
Rose hips also have choleretic properties: you can prepare an infusion from dried berries or take the remedy Holosas (a dessert spoon a day, children - half a teaspoon). You should also take vitamins A, C, D, E, K.
Homeopathy
Homeopathic remedies for the treatment of bile stasis include Galstena (sublingual tablets and drops) and Hepar compositum (a solution in ampoules for parenteral use).
Both preparations contain many components, but each contains milk thistle (Silybum marianum) or milk thistle (in the form of an extract of the plant's seeds). Among the active substances of milk thistle, the flavonolignan complex (silibinin, silybins, isosilybins, silychristin, isosilychristin, silydianin and dihydroquercetin) is especially beneficial for the liver. Milk thistle also contains vitamin K and ω-6 fatty linoleic acid.
The drug Galstena stimulates the production of bile and activates its movement from the liver to the gallbladder and further, relieves spasms and inflammation. Doctors recommend taking this remedy one tablet (under the tongue) twice a day; drops - 7-10 drops three times a day (between meals). The instructions note side allergic reactions, and the contraindications only indicate hypersensitivity. However, Galstena contains Chelidonium majus, that is, celandine, and this plant is known to be poisonous (due to the presence of isoquinoline alkaloids) and can cause cramps, intestinal spasms, salivation and contractions of the uterine muscles.
The homeopathic preparation Hepar compositum consists of 24 active substances (one of them is milk thistle). It is used by intramuscular or subcutaneous injections - one ampoule every 3-7 days for 3-6 weeks. Side effects include urticaria and itching.
Surgical treatment
Today, depending on the etiology and localization of bile stasis, surgical treatment includes the following types of surgical intervention:
- laparoscopic removal of stones in cholelithiasis and bile duct stones (endoscopic lithoextraction);
- removal of a cyst or tumor that obstructs the flow of bile;
- installation of stents in the bile ducts;
- balloon dilation of the lumen of the bile ducts when they are obstructed;
- drainage of the common bile duct (choledochostomy);
- expansion of the gallbladder or its ducts with stenting and formation of biliary anastomoses;
- gallbladder sphincter surgery;
- removal of the gallbladder (cholecystectomy).
In case of biliary atresia (see section – Bile stasis in children), ducts in the liver are created surgically: in children of the first two months, reconstructive surgery (portoenterostomy) is performed, but a liver transplant may also be required.
Folk remedies
Among the variety of recipes for folk treatment of this pathology, the most adequate advice can be highlighted:
- Consume a mixture of homemade juices for 1-1.5 months - carrot, apple and beetroot (in equal proportions); you should drink 150 ml of this juice (one hour after eating).
- Drink natural apple cider vinegar by adding a tablespoon to a cup of apple juice or water with lemon juice; you can also add a teaspoon of honey.
- Take mumiyo dissolved in water for two weeks (0.2 g tablet per 500 ml); drink the entire amount per day (in several doses, half an hour before meals). It is recommended to take 5-7 day breaks between courses of use. A full cycle of such mumiyo therapy can last 3-5 months. However, the folk recipe does not mention that with such volumes of use of this biostimulant, there may be diarrhea, increased heart rate and increased blood pressure.
Traditional medicine also suggests using oats and making a decoction from them: pour a tablespoon of whole grains with two glasses of water and boil for about half an hour; drink 15-20 minutes before meals 3-4 times a day (drink the entire amount during the day). However, it should be borne in mind that oats act as a laxative and reduce blood pressure.
Persimmon can help with diarrhea when bile stasis occurs (it is recommended to prepare a decoction for this). Persimmon contains a lot of beta-carotene and vitamin C, as well as manganese, a cofactor for the synthesis of the antioxidant enzyme superoxide dismutase, which increases the resistance of the mucous membranes. Other powerful antioxidants found in persimmon include lycopene and cryptoxanthin. But pomegranate not only promotes hematopoiesis, but also has choleretic properties; however, this fruit contributes to constipation.
So, it is safer to use choleretic herbs for bile stasis: fumitory, sandy everlasting, bird's knotweed (knotweed), bogbean, naked hernia, corn silk, sweet clover, dyer's broom, mountain arnica. Decoctions are prepared and taken like pharmaceutical choleretic mixtures (see above).
[ 28 ], [ 29 ], [ 30 ], [ 31 ], [ 32 ], [ 33 ]
Diet for bile stasis
The therapeutic diet for bile stasis is diet No. 5 and the introduction of certain restrictions and even prohibitions into the diet.
That is, you should exclude fatty foods (animal and cooking fats, rich broths, fatty meat and fish, whole fat milk, cream, butter, sour cream, etc.); canned food and meat delicacies with preservatives; semi-finished products and snacks; refined sugar, fructose and sweets; bread and pastries made from white flour. See also - Diet for gallbladder diseases
You need to eat: fresh vegetables and fruits; boiled, baked or stewed lean meat and poultry, seafood (source of protein); legumes (vegetable protein); healthy fats (walnuts, almonds, flaxseed, pumpkin seeds).
Whole grains such as brown rice, barley, oats, buckwheat are necessary; healthy oils with polyunsaturated fatty acids ω-3 and ω-6 acids: olive oil, sesame oil, flaxseed oil.
Exercises for bile stasis
Doctors warn: without movement, all processes in the body, including bile secretion, are disrupted. Therefore, gymnastics for bile stagnation is necessary, but it should not aggravate the pathology and increase symptoms.
Walking (at least an hour a day) is recommended, as well as exercises for bile stasis, during which you do not need to make low forward bends, sharp turns, strong swinging movements and jumps.
Remember simple morning exercises: most of its elements are suitable for bile stagnation. For example:
- Feet shoulder-width apart, hands on your waist – alternately turn your body to the right and left sides.
- Feet shoulder-width apart, hands behind head – bend to the right and left.
- In the same starting position, bend your right leg at the knee and reach towards it with your left elbow, then bend your left leg and do the same with your right elbow.
- Lie on your back (legs straight, arms extended along the body); as you inhale, bend your right leg at the knee, bringing it closer to your stomach; as you exhale, return to the starting position, and do the same with the other leg.
- Lying on your back, bend your knees, place the palm of one hand on your stomach, take deep breaths with the diaphragm raised and the abdominal wall pushed out; as you exhale, draw in your stomach.
- Perform similar breathing movements while lying on your right and left sides.
By the way, the last exercise is a kind of internal self-massage of almost all organs located exactly where bile stagnation occurs. But a special therapeutic massage for bile stagnation should only be prescribed by a doctor who has the results of an examination of the patient's gallbladder and liver.
More information of the treatment
Prevention
Prevention of bile stasis is possible only in relation to certain causes of its occurrence (alcohol, infections, helminths, tumors, unhealthy diet, lack of physical activity). In case of congenital and genetically determined syndromes, as well as in case of endocrine and hormonal factors of pathologies of the hepatobiliary system, there are no preventive measures.
Forecast
It is difficult to talk about the prognosis for the development of bile stasis in a particular case, taking into account the individual characteristics of each patient, as well as all the complications, consequences and a whole range of associated problems of general metabolism.