Medical expert of the article

New publications
Abnormalities of the uterus
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

By incorrect position of the genitals we mean a persistent deviation from their typical ("normal") position, usually accompanied by pathological phenomena. The position of the genitals changes with age. In childhood, the uterus is located higher than during puberty. In old age, on the contrary, it is lower, often deviating backwards.
Causes uterine anomalies
In the position of the female genitals, there are relatively often violations (anomalies), which are mainly secondary and depend on various pathological processes that occur both in the genitals and outside the uterus and its appendages. The disorders observed in this case are not only determined by the displacement of the uterus, but also depend on the underlying disease that caused this anomaly. Less often, incorrect positions of the uterus are congenital.
Hyperanteflexia may also be caused by shortening of the uterosacral ligaments due to a long-term chronic inflammatory process. In such cases, due to the shortening of the uterosacral ligaments, the area of their attachment to the uterus is pulled back, and the body approaches the cervix.
The causes of retroflexion include organic (decreased tone of the uterus and its ligaments due to infantilism, asthenic syndrome, birth trauma, inflammation, tumors of the uterus and ovaries) and constitutional (15% of healthy sexually mature women have retrodeviation).
Risk factors
Factors that ensure the normal position of the female genital organs are:
- own tone of the genitals;
- the relationship between internal organs and the coordinated activity of the diaphragm, abdominal wall and pelvic floor;
- suspending, fixing and supporting the uterine apparatus.
Pathogenesis
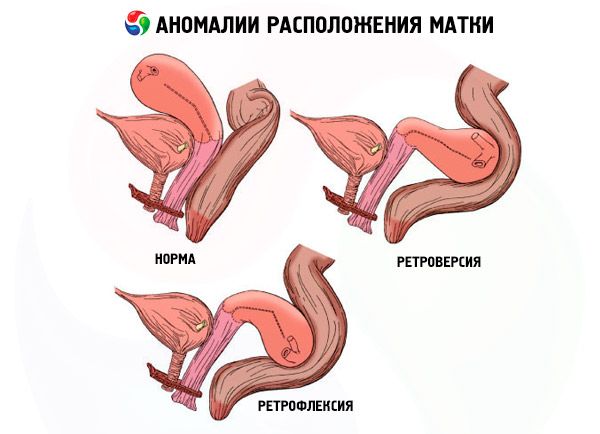
The typical position is conventionally considered to be the position of the genitals in a healthy, sexually mature, non-pregnant and non-lactating woman, in a vertical position with an empty bladder and rectum. In this case, the uterus occupies a middle position in the small pelvis, the fundus of the uterus does not protrude above the plane of the entrance to the small pelvis, the vaginal part of the cervix is at the level of the plane passing through the sciatic spines. The fundus of the uterus is directed upward and forward, the vaginal part of the cervix is directed downward and backward. The entire axis of the uterus is slightly inclined forward (anieversio). A bend is formed between the body and the cervix. The resulting angle is obtuse and open forward (anteflexio).
The proper tone of the genitals depends on the correct functioning of all body systems. A decrease in tone may be associated with a decrease in the level of sex hormones, a violation of the functional state of the nervous system, and age-related changes.
The relationships between the internal organs (intestine, omentum, parenchymatous and genital organs) form a single complex due to their direct contact with each other. In this case, capillary adhesion is formed, which, together with the gaseous contents of the intestine, helps to balance the weight of the internal organs and limits their pressure on the genital organs.
The suspensory apparatus consists of the round and broad ligaments of the uterus, the proper and suspensory ligaments of the ovary.
The fixing apparatus includes the sacrouterine, cardinal, uterovesical and vesicopubic ligaments.
The supporting apparatus is represented by the muscles of the pelvic floor, the vesicovaginal septum, the rectovaginal septum and dense connective tissue located at the lateral walls of the vagina.
Symptoms uterine anomalies
The symptoms of hyperanteflexia correspond to those of the underlying disease (symptoms of infantilism, inflammatory process, etc.). Since retroflexion is not an independent disease, its clinical picture is determined by the symptoms of the disease that caused retroflexion - pain, dysfunction of adjacent organs, menstrual and secretory dysfunction. Constitutional retroflexion is asymptomatic and is discovered accidentally during preventive examinations.
 [ 19 ]
[ 19 ]
Forms
The displacement of the uterus can occur along the vertical plane (up and down), around the longitudinal axis and along the horizontal plane.
Displacement of the uterus along the vertical plane includes uterine elevation, prolapse, prolapse and eversion. When elevated, the uterus moves upward, its fundus is located above the plane of the entrance to the small pelvis, and the vaginal part of the cervix is above the spinal plane. Pathological elevation of the uterus occurs when menstrual blood accumulates in the vagina due to atresia of the hymen or lower part of the vagina, with large tumors of the vagina and rectum, with encapsulated inflammatory effusions in the Douglas space. Elevation of the uterus can also occur when it adheres to the anterior abdominal wall after laparotomy (cesarean section, ventrofixation).
With prolapse (descensus uteri), the uterus is located below the normal level, but the vaginal part of the cervix does not protrude from the genital slit even during straining. If the cervix protrudes beyond the genital slit, we speak of prolapse of the uterus (prolapsus uteri). A distinction is made between incomplete and complete prolapse of the uterus. With incomplete prolapse of the uterus, only the vaginal part of the cervix protrudes from the vagina, and the body of the uterus is located above, beyond the genital slit. With complete prolapse of the uterus, its cervix and body of the uterus are located below the genital slit. Prolapse and prolapse of the uterus are accompanied by prolapse of the vagina.
Uterine inversion is extremely rare. In this anomaly, the serous membrane is located inside, and the mucous membrane is outside, the inverted body of the uterus is located in the vagina, and the cervix, fixed in the area of the fornices, is located above the level of the body.
In most cases, eversion of the uterus occurs due to improper management of the postpartum period (squeezing out the placenta, pulling on the umbilical cord to extract the placenta) and, less often, when a tumor with a short, non-stretchable stalk is expelled from the uterus.
The displacement of the uterus around the longitudinal axis has two forms: rotation of the uterus (rotation of the body and cervix from right to left or vice versa) and torsion of the uterus (torsio uteri). When the uterus is torsed, the body of the uterus rotates in the area of the lower segment with the cervix immobile.
There are several types of displacement of the uterus in the horizontal plane: displacement of the entire uterus (antepositio, retropositio, dextropositio and sinistropositio), incorrect inclination of the uterus (retroversio, dextroversio, sinistroversio) and pathological bending of the uterus.
The displacement of the entire uterus can be in four forms: antepositio, retropositio, dextropositio and sinistropositio.
Normally, an obtuse angle, open anteriorly, is formed between the body and the cervix. However, in case of pathological bending, this angle can be acute, open anteriorly (hyperanteflexio) or posteriorly (retroflexio).
Of all the types of anomalies in the position of the genital organs, the most important clinical significance are downward displacement of the uterus (prolapse), retrodeviation (posterior displacement, mainly retroflexion) and pathological anteflexion (hyperanteflexion).
Hyperanteflexia usually accompanies sexual infantilism – the size of the cervix exceeds the length of the uterus. With hyperanteflexia, the uterus does not cover the bladder, intestinal loops penetrate between the bladder and uterus, putting pressure on the bladder. With prolonged exposure, the bladder and vagina may shift downwards.
In retroflexion, the angle between the body and the cervix is open not forward, as in the normal position, but backward. The body of the uterus is directed backward, and the cervix is slightly forward. With this position of the uterus, the normal position of the internal organs is disrupted. The urinary bladder is not covered by the uterus, intestinal loops penetrate the vesicouterine space and press on the wall of the urinary bladder and on the anterior surface of the body of the uterus. Therefore, retroflexion is a risk factor for prolapse of the genitals.
Diagnostics uterine anomalies
Retroflexion diagnostics does not present any difficulties. During vaginal examination it is established that the cervix is facing forward, the body of the uterus is located backwards and is determined through the posterior fornix, between the body and the cervix of the uterus an angle open backwards. With mobile retroflexion it is often possible to bring the uterus into the correct position, with fixed retroflexion it is usually not possible to bring it out.
What do need to examine?
Who to contact?
Treatment uterine anomalies
Treatment of hyperanteflexia is aimed at eliminating the cause that caused its development. Treatment of retroflexion is aimed at eliminating the cause of the underlying disease that caused retroflexion (patients with asymptomatic retroflexion do not require treatment).