Medical expert of the article

New publications
What is marsupialization?
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
During surgical interventions, including laparoscopic ones, performed to treat cystic formations of various organs, a surgical method called marsupialization (from the Greek marsyppion – small bag) is used.
Indications for the procedure
The main indications for marsupialization are the presence of:
- Bartholin's gland cysts;
- large or inflamed cysts of the duct, canal or Gartner's tract;
- pancreatic cysts, as well as pseudocysts against the background of pancreatic necrosis;
- simple cystic formation of the kidney or liver.
The marsupialization technique can also be used for:
- pilonidal cyst - cyst of the coccyx;
- odontogenic cyst of the jaw; [ 1 ]
- sublingual salivary gland cyst (ranula); [ 2 ], [ 3 ]
- large intranasal cyst with congenital dacryocele - accumulation of fluid or mucin in the lacrimal sac or its inflammation (dacryocystitis);
- lacrimal duct cysts (tear ducts);
- nasopharyngeal (nasopharyngeal) Thornwaldt's cyst;
- vocal fold cyst.
Preparation
As with any surgical intervention, preparation for this operation requires an ECG and a general blood test, coagulogram, RW; a general urine test is taken. Before marsupialization of the Bartholin gland cyst or Gartner's ducts, a blood test is taken for infections that cause STIs, and the vaginal microflora is examined (by taking a smear).
Also, preoperative examinations carried out by specialized specialists include: ultrasound, computed tomography scanning or magnetic resonance imaging of the relevant organ.
The optimal method of pain relief is selected in advance: local or epidural anesthesia or general anesthesia. [ 4 ]
Technique marsupialization
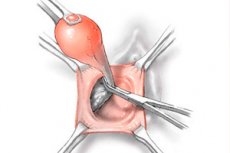
In general, the technique of marsupialization involves opening the cyst (cutting its wall) and removing its contents (a sample of which is sent to the laboratory for microbiological testing). Then the edges of the cut wall of the opened cyst are sutured to the edges of the surgical wound or nearby tissues to form an open artificial "sac" or "bag" (the cyst shell remains deep in its open cavity). The healing process of the "sac" occurs through granulation with the formation of scar tissue in its place.
It should be borne in mind that marsupialization of the omental bursa (bursa omentalis) is one of the stages of laparotomy operations - through an incision in the abdominal wall - in purulent complications of acute pancreatitis and infected necrotic pancreatitis, in inflammation of false cysts of the pancreas (which form in chronic pancreatitis). During the abdominal intervention, the omental bursa is opened, fixed with the gastrocolic ligament and drained, cleaning the parapancreatic area. [ 5 ]
In addition, specific surgical manipulations and techniques depend on the location of the cystic formation.
Marsupialization of the Bartholin gland cyst (located at the base of the labia minora - in the vestibule of the vagina) is performed when attempts to get rid of it by other methods (for example, puncture) have been unsuccessful and there is a large amount of suppuration - a secondary abscess.
Therefore, marsupialization of the Bartholin gland abscess can be performed simultaneously under local anesthesia: the surgeon widely opens the wall of the abscess cavity (i.e. the gland itself) and evacuates its contents. Then the abscess membrane is attached laterally to the skin of the introitus and medially to the vaginal mucosa with absorbable sutures, and granulation and re-elitization of the wound occur in this area over time.
As clinical practice shows, both the healing rate and the recurrence rate are the same for marsupialization, fistulization and sclerotherapy (using ethanol or silver nitrate).
Marsupialization of the Gartner's duct cyst, a rare cavity formation in the vaginal walls in the area of the embryological remnant of the mesonephric duct, is performed only in the presence of symptoms: pain or pressure in the pelvic area, dysuria, dyspareunia, tissue protrusion. And if the cyst is large enough, it is removed to avoid obstetric complications. [ 6 ]
Marsupialization of pancreatic, kidney, liver cysts
Marsupialization of a pancreatic cyst is most often used if the cyst is false, formed during chronic pancreatitis, and removal of the cyst is technically impossible. During the operation, the gastrocolic ligament is dissected and the omental bursa is opened to gain access to the gland; then the cyst is drained through a puncture in its capsule, after emptying the cavity, part of the anterior wall of the capsule is opened, and its edges are sutured to the edges of the wound.
This operation is not advisable if the cyst has thin walls or does not have formed walls, as well as if there is a connection between the cystic formation and the pancreatic ducts.
Laparoscopic intrarenal marsupialization of renal cysts – along with transdermal puncture and aspiration or subsequent sclerotherapy – is an alternative to open surgical methods for the treatment of simple cysts associated with renal failure, pain, hematuria and infection. [ 7 ]
As a rule, a liver cyst is asymptomatic, and if symptoms are present, it is most often subjected to percutaneous aspiration of the contents under ultrasound control. However, in rare cases, laparoscopic or laparotomic marsupialization of a liver cyst is used, including a giant one, which in many patients is complicated by rupture and bleeding.
Contraindications to the procedure
The clinical application of marsupialization is limited to cystic lesions with liquid contents and cannot be used for most dermoid and teratoid cysts. This method is unacceptable in cases of parasitic cysts, such as echinococcal cysts.
In addition, marsupialization is contraindicated when conservative treatment attempts have failed and if complete resection is necessary.
Contraindications also include: severe heart failure, exacerbation of existing diseases and acute infectious diseases, poor blood clotting, bleeding, and oncological diseases.
Consequences after the procedure
Common consequences noted after the marsupialization procedure include pain, bleeding, tissue swelling, and hematoma formation.
Complications after the procedure are associated with infection of the surgical wound (patients develop a fever) and its suppuration.
Complications may also occur after surgery for pancreatic, renal, and hepatic cysts. For example, bile leakage may occur after marsupialization of a liver cyst. The splenic artery may be damaged during the procedure on a pancreatic cyst, and patients with pancreatitis may experience localized fluid accumulation in the left paracolic gutter (requiring surgical drainage). Later, there is a risk of developing an abdominal hernia and chronic duodenal fistula.
Experts also consider a relapse of the cyst to be a remote complication that is a consequence of an unsuccessful operation.
Care after the procedure
The main principle of proper postoperative care and successful rehabilitation is compliance with antiseptic rules and all recommendations of doctors. Patients have their temperature measured, an increase in which allows for timely detection of the inflammatory process, for the suppression of which antibiotics are prescribed after surgery.
Specific recommendations depend on the location of the surgical intervention. Thus, after marsupialization of a Bartholin gland cyst or a Gartner duct cyst, the genitals should be treated with antiseptic solutions; kept clean and dry; any physical activity and bathing (shower only) should be avoided for two weeks, and sexual intercourse should be avoided for at least a month.
In addition, to prevent complications during the recovery period, you should take the prescribed medications, eat properly (especially after marsupialization of a pancreatic, liver or kidney cyst), and drink enough water.