Medical expert of the article

New publications
Valgus ossicle on the foot
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
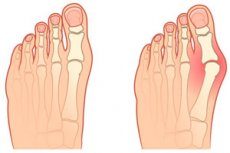
Both a valgus ossicle and an ossicle on the foot (also commonly called a "bump") mean one thing - valgus deformity of the big toe or hallux valgus (in Latin hallux - first toe, valgus - crooked). It is a lateral (lateral) deviation of the toe at the metatarsophalangeal joint that connects it to the foot.
Epidemiology
Some reports suggest that 23-35% of adults have valgus ossicles on the foot, which form between the ages of 30 and 50 years. There is a higher prevalence in women, with different ratios reported in the literature, ranging from 2:1 to 15:1 among affected women for every man. [1]
Risk factors
Risk factors for valgus deformity of the big toe include:
- Stiff, tight and narrow pointed toe shoes, high-heeled shoes;
- Female gender and postmenopausal period in women (with changes in hormonal background);
- Increased load on the feet during "standing" work, chronic Achilles tendon strain;
- Overweight;
- Hereditary predisposition (including brachymorphic body type);
- Disorders of body statics and dynamics, leading to problems with posture and foot position;
- The presence of rheumatoid arthritis;
- Systemic connective tissue diseases.
Causes of the valgus ossicles on the foot
The formation of hallux valgus can be caused by: [2], [3]
- Foot deformity in the form of transverse flatfoot with fan-shaped divergence of the metatarsal (metatarsal) bones of the foot and an increase in its transverse size;
- Deviation of the foot in the case of congenital or acquired equinovarus deformity, i.e. Clubfoot;
- Deforming osteoarthritis of the joints of the foot, specifically the first metatarsophalangeal joint;
- Hypermobility of the first metatarsophalangeal joint (articulating the medial and lateral cuneiform and first metatarsal bones);
- Foot deformities in systemic diseases;
- Foot fracture, ligament and tendon sprain.
Compressive shoes, such as high heels, are considered an external factor predisposing to valgus deformity due to increased stress on the first metatarsal bone and valgus stress at the first metatarsal joint when the foot slides forward into a narrow toe while walking. [4], [5], [6]
The prevalence of valgus deformity increases with age due to changes in joint mechanics and plantar loading patterns that occur with age. [7]
Hallux valgus also has a strong genetic predisposition. In a large level IV study, 90% of patients with valgus deformity had at least one family member with the condition (n = 350). Although the exact nature of inheritance remains unclear, it is assumed that inheritance is autosomal dominant with incomplete penetrance. [8]
Also read - why do bunions form on feet?
Pathogenesis
In humans, the big toe consists not of three but of two phalanges: proximal and distal, which articulate at the interphalangeal joint. The proximal phalanx articulates with the first metatarsal bone (os metatarsale I) at the metatarsophalangeal joint (a. Metatarsophalangeae), and together with the distal phalanx they form the big toe or first toe. [9]
The basic motion of the metatarsophalangeal joint is flexion-extension with minimal extension and adduction; mediolateral motion in the joint is limited by the collateral (lateral) ligaments.
The mechanism of valgus ossicle formation is seen in the curved position of the first toe towards the second toe; an increase in the angle between the first and second metatarsal bones and loss of stability of the first metatarsophalangeal joint. [10]
The tendon that drives the big toe no longer runs parallel to the big toe, but pulls its distal phalanx inward, causing displacement of its base (the big toe is as if turned out of the metatarsophalangeal joint). And part of the head of the first metatarsal bone tilts medially and begins to protrude at its distal end, i.e. Exostosis of the metatarsophalangeal joint is formed. [11]
Symptoms of the valgus ossicles on the foot
This foot deformity is manifested by symptoms such as:
- Deviation of the big toe towards the outer edge of the foot - towards the little finger;
- Hyperemia and edema of the first metatarsophalangeal joint;
- Pain in the area of the protruding part of the head of this joint;
- Formation of dry omosolelloses on the plantar part of the foot;
- Protrusion of the pad of the thumb.
In the beginning, the valgus bone only hurts with specific tension and pressure on the first metatarsophalangeal joint. In later stages, there may be excruciating pain in the big toe even at rest.
The bulge of the head of the metatarsal bone gradually increases, pressing against the shoe, and the pressure can cause inflammation of the valgus ossicle. Pain along with swelling and redness may also occur on the inner edge of the foot above the first metatarsal bone.
Depending on the angle between the long axis of the proximal phalanx and the first metatarsal bone of the big toe, the angle of valgus deformity is determined, i.e. The stage of valgus ossicle. Grade I deformity is determined at an angle of more than 15-18°, grade II - at an angle of more than 25°, and grade III - at an angle of more than 35°.
The pain and symptoms of valgus deformity do not necessarily depend on the degree of deformity. Severe valgus deformities of the big toe are often still painless, while some patients experience severe foot pain even with grade I-II valgus.
Complications and consequences
Complications of valgus deformity of the big toe include:
- Recurrence is the most frequent complication, with rates ranging from 8% to 78%; [13], [14]
- Inflammation of the articular bag of the first metatarsophalangeal joint - bunion of the big toe;
- Pain in the metatarsophalangeal joints - metatarsalgia - due to weight transfer from the big toe to the overstretched other toes while walking;
- Deformity of the neighboring toes of the foot;
- Crossed second toe (which is deflected laterally toward the valgus deformity due to the pressure of the thumb), there may also be an overlap of the thumb on the second toe;
- Arthritis of the metatarsophalangeal joint.
The unnatural shape of the metatarsophalangeal joint and forefoot in valgus deformity disrupts normal foot function.
Diagnostics of the valgus ossicles on the foot
Differential diagnosis
Differential diagnosis includes gout, arthritis of the metatarsophalangeal joint, rheumatoid arthritis of the foot, and intertarsal neuroma.
Treatment of the valgus ossicles on the foot
Physiotherapy is used to treat a minor degree of valgus deformity of the big toe: therapeutic massage of the valgus ossicle; exercises for valgus ossicle that strengthen the ligaments and improve the mobility of the joints of the foot, etc. Read more:
How to treat valgus ossicle at home?
The metatarsophalangeal joint is used to correct the metatarsophalangeal joint and fix the big toe in the correct anatomical position:
- A valgus splint;
- Valgus bandage or silicone valgus corrector for the big toe ossicle (with a soft pad between the first two toes);
- Kinesiology tape taping of valgus ossicles.
- Valgus Patch (Epitact Activ, Hallux Valgus Protection, Instant Pain Relief Compeed) - to protect the valgus deformity of the big toe from chafing and for pain relief.
When valgus ossicle hurts, it is recommended to apply pain relieving ointments. Ointments for valgus ossicle, which would correct or at least reduce the deformity of the thumb, does not exist. And almost all external remedies belong to non-steroidal anti-inflammatory drugs, for more information - ointments for joint pain
Folk remedies for valgus ossicles are also used, for more information see. - how do I get rid of bunions on my feet?
But all of these treatments address the symptoms but do not correct the actual deformity.
In some cases, surgical treatment is used to correct valgus deformity, using various methods of metatarsal osteotomy, arthroplasty, fixation (with a plate, screws or a spoke), removal of valgus ossicles with laser, and others. [17]
All the details are in the publications:
Rehabilitation after the removal of valgus ossicles lasts at least two to two and a half months (depending on the type of surgical intervention), during which patients are limited in movement and must wear orthopedic shoes, as well as undergo prescribed physical therapy procedures.
Prevention
To reduce the risk of valgus ossicles on the foot, doctors recommend wearing comfortable shoes (not squeezing the foot), every day do not wear shoes with high heels, if flat feet use orthopedic insoles, as often as possible to walk barefoot and do leg exercises that strengthen the muscles of the foot.
More information:
Forecast
Depending on the stage of deformity and the age of the patient, the prognosis of Hallux valgus varies. It is certainly better in the young than in the elderly, because at a young age there are good prospects for correcting the valgus position of the big toe with physical therapy of the foot and conservative treatment.
In old age, valgus ossicle on the foot is no longer amenable to active recovery, and surgeries only slow down the process of deformity development.