Medical expert of the article

New publications
Small-focal myocardial infarction
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Small-focal myocardial infarction is a morphologic variant of damage to the muscle tissue of the heart that involves the subendocardial zone, the layer in the endocardium that connects it to the myocardium, and represents a subendocardial infarction. [1]
Epidemiology
According to clinical statistics, myocardial infarction with acute partial occlusion of coronary arteries and formation of a focus of necrosis in the subendocardium accounts for 5-15% of all cases of acute myocardial infarction.
According to other data, nearly 60% of myocardial infarctions occur in the subendocardial region. [2]
Causes of the shallow myocardial infarction.
Typically, subendocardial or small-focal infarction is the result of a local reduction in blood supply due to partial thrombotic or embolic occlusion (occlusion) of the small epicardial arteries affected by atherosclerosis - coronary arteries, which are located deep in the epicardial fatty tissue.
The subendocardium lies deep within the endocardium (the inner lining lining lining of the heart cavity) and contains thick elastic and collagen fibers and blood vessels (arterioles and capillaries).
A subendocardial infarction is called a small-focal infarction because a small area of the subendocardial wall of the left ventricle, the interventricular septum, or the papillary muscles located in the ventricles of the heart is affected.
Also, this variant of damage to the muscle tissue of the heart in cardiology is defined as intramural infarction or myocardial infarction without ST-segment elevation (or without a Q tooth, reflecting on the ECG excitation of cardiomyocytes of the inner wall of the ventricles and interventricular septum). [3]
Read more:
Risk factors
The most important risk factors for developing a small-focal infarction are:
- Old age;
- Angina pectoris;
- Coronary stenosing atherosclerosis;
- Chronic arterial hypertension;
- Congestive heart failure;
- IBS - coronary heart disease;
- Pulmonary embolism.
Pathogenesis
The mechanism of myocardial damage in small-focal (subendocardial) infarction, as in any infarction, is based on ischemic necrosis of the heart muscle tissue due to a significant reduction or cessation of its blood supply.
Blood supply is impaired by stenosis and/or occlusion of coronary arteries, which in most cases are due to rupture of atherosclerotic plaque with activation and aggregation of blood platelets and thrombus formation in the vessel lumen.
Explaining the pathogenesis of this morphological type of infarction, cardiologists note the increased vulnerability to ischemic necrosis of the subendocardial part of the left ventricle, because high systolic pressure in its cavity during redistribution of blood flow can lead to compression of blood vessels inside the myocardium. In addition, the smaller wall thickness of the vessels located here also plays a role.
But, as studies have shown, shallow focal infarction is characterized by preservation of one or two layers of myofibrils adjacent to the endocardium, although degenerative changes of cardiomyocytes occur in deeper myocardial fibers, and foci of coagulation necrosis of various sizes are formed on top of these fibers.
Symptoms of the shallow myocardial infarction.
In the case of small-focal (subendocardial) infarction, patients may feel the first signs in the form of chest pain, shortness of breath, tachyarrhythmia, nausea, sweating.
All the details are in the publications:
Complications and consequences
Among the possible complications and consequences of small-focal/subendocardial infarction, experts name: recurrent angina pectoris and formation of left ventricular aneurysm; systolic heart failure and dyskinesia of part of the myocardium; disruption of the conduction system of the heart in the form of atrioventricular block.
Also read - myocardial infarction: complications
Diagnostics of the shallow myocardial infarction.
The diagnosis of myocardial infarction is established, first of all, by the results of electrocardiography (ECG). Also an important tool of non-invasive imaging (giving comprehensive information on the presence and localization of reversible and irreversible myocardial damage) is. MRI of the heart. [4]
Instrumental diagnosis is described in detail in the publication - instrumental methods of cardiac examination
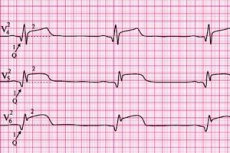
In partial occlusion of the epicardial coronary artery, a small-focal myocardial infarction on the ECG demonstrates ST-segment depression - a shift of the segment showing the period of full ventricular excitation below the isoelectric line, an inverted (flattened) T and the absence of the Q (which reflects excitation of the interventricular septum and the inner surface of the ventricles).
See also - eCG in myocardial infarction
Blood tests for specific cardiac troponins (TnI and TnT) and levels of white blood cells, myoglobin, creatine kinase isoenzyme, and lactate dehydrogenase confirm the diagnosis.
More information - markers of myocardial infarction
And differential diagnosis should distinguish between transmural or large-focal and small-focal myocardial infarction, focal myocarditis, pericarditis, acute heart failure, acute pulmonary embolism. [5]
Read more - myocardial infarction: diagnosis
Who to contact?
Treatment of the shallow myocardial infarction.
All patients with suspected myocardial infarction should take acetylsalicylic acid (Aspirin) at a dose of 162 to 325 mg, chewed for rapid absorption through the mouth. Also, all patients should be given supplemental oxygen.
Nitroglycerin (sublingual and intravenous) is used to relieve symptoms.
But drugs of the group of thrombolytics (Streptokinase, Alteplase, Tenecteplase, etc.) are not used in this variant of infarction.
All details in the material - myocardial infarction: treatment
Prevention
Treatment of atherosclerosis, IBS and other cardiologic diseases, as well as control of blood pressure doctors consider the main methods of prevention of damage to the muscle tissue of the heart in the subendocardial zone. [6]
Forecast
Since the volume of myocardial damage in small-focal infarction is limited, and the associated clinical manifestations and complications are usually less pronounced than in infarcts involving the entire thickness of the myocardial wall, its early or hospital prognosis is considered favorable. However, late complications that may lead to transmural (large-focal) infarction and sudden death should be considered.
See also - myocardial infarction: prognosis and rehabilitation