Medical expert of the article

New publications
Ruptured kidney
Last reviewed: 12.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Violation of the anatomical integrity – kidney rupture – with partial or complete dysfunction of this vital internal organ is a life-threatening condition.
Epidemiology
According to statistics, kidney damage occurs in at least 10% of all significant abdominal injuries, and the prevalence of kidney rupture is 3-3.25%. In 90-95% of cases, kidney injury is closed blunt, and its most common cause (over 60%) is a car accident.
This is followed by kidney rupture due to catatrauma (43%) and as a result of various sports injuries (11%).
According to foreign sources, kidney rupture in children occurs in 30% of cases due to road accidents (in 13% – as pedestrians); in 28% – as a result of blunt trauma when falling while riding a bicycle; in 8% – from falls and bruises on playgrounds and sports grounds.
Causes kidney rupture
The most common causes of kidney injury leading to rupture are related to closed trauma, including sports trauma: a kidney may rupture from a blow (direct blunt) to the upper abdomen, lateral, middle or lower back, lower chest; from a blow during a catatrauma (fall from a height); from hypercompression during a traffic accident, etc.
Trauma can be penetrating with a stab or gunshot wound with profuse bleeding, causing death from kidney rupture or damage to other parenchymatous organs incompatible with life. [ 1 ]
Iatrogenic causes include complications of surgical interventions and procedures, in particular kidney biopsy and shock wave lithotripsy (breaking up kidney stones).
Atraumatic spontaneous or involuntary renal rupture is rare and, as experts note, can be provoked by the rupture of any neoplasm in the kidney, for example, progressive malignant hypernephroma, renal angiolipoma (benign mesenchymal tumor), [ 2 ] as well as hemorrhagic rupture of a renal cyst. [ 3 ]
Risk factors
Factors that partially determine the increased risk of kidney rupture include:
- childhood (due to the lower position of the kidneys relative to the ribs and the small volume of fatty tissue surrounding the kidney);
- renal developmental anomalies;
- disruption of the organ's position - nephroptosis (prolapse of the kidney);
- the presence of neoplasms in the kidneys;
- pathological changes associated with large solitary cyst and polycystic kidney disease; [ 4 ], [ 5 ]
- a whole range of diseases and congenital syndromes with complications in the form of hydronephrosis of the kidney;
- urolithiasis leading to obstruction of the urinary tract;
- renal artery aneurysm;
- autoimmune diseases of connective tissue. [ 6 ]
Pathogenesis
The ribs, abdominal and back muscles, as well as the supporting fascia system and surrounding fatty tissue, protect the kidneys well. However, their lower poles are located below the 12th ribs, and this is the most vulnerable area of the kidneys in case of impact or fall.
The pathophysiology of the rupturing action in such injuries consists of compression and displacement of the organ, as well as deceleration and acceleration forces. They act in different ways, for example, acceleration forces can cause displacement of the kidney and its “collision” with the ribs or transverse processes of the vertebrae (T12-L3). The compression effect during kidney compression is due to a sharp increase in pressure - intraluminal and in the urine accumulation system. [ 7 ]
In the case of a tumor, cyst, stones or hydronephrosis, partial atrophy of the cortex and destructive changes in the renal parenchyma, thinning of the walls of the renal capsule and its stretching are observed.
Symptoms kidney rupture
The first signs of a kidney rupture are hematuria (blood in the urine) and constant back pain - in the lumbar region - with tension in the lumbar muscles. The pain is localized on the right if the right kidney has ruptured, on the left - if the left kidney has ruptured. And its intensity depends on the degree of damage to the integrity of the organ.
In addition, symptoms appear in the form of progressive edema (swelling) in the lumbar region (due to perirenal hemorrhage and hematoma in the retroperitoneal space); decreased blood pressure; general weakness and dizziness; cold sweat and pale skin; nausea and vomiting; fever; decreased or complete cessation of urine output. [ 8 ]
Where does urine go when a kidney ruptures? Due to the disruption of the integrity of the renal pelvis and/or calyces, urine leaks (extravasation) outside the kidney and accumulates in the adjacent area (in the perirenal tissues) and in the retroperitoneal space. Urine entering the perirenal adipose tissue leads to its inflammation with cell death (lipolysis) and their replacement with fibrous tissue. An encapsulated formation is formed in the form of a perirenal pseudocyst - urinoma, which can also cause pain and a feeling of pressure.
Tachycardia, severe cyanosis, blurred vision and confusion against the background of falling blood pressure indicate the development of a state of shock.
Based on the location of the damage, experts distinguish the following types of ruptures:
- rupture of the renal capsule (capsula adiposa) – its thin fibrous membrane with partial damage to the cortical layer (and the formation of a perirenal hematoma);
- subcapsular rupture of the kidney - a rupture of the renal parenchyma, that is, its internal tissues, that does not affect the structure of the urine accumulation system (the calyceal-pelvic complex);
- rupture of the renal parenchyma with damage to its cups and pelvis, accompanied by thrombosis of part of the renal artery;
- crushed (total) rupture of the kidney.
Complications and consequences
A kidney rupture can have complications and consequences in the form of:
- secondary arterial hemorrhage due to the formation of a pseudoaneurysm or arteriovenous fistula;
- formation of urinary or hemorrhagic kidney cysts;
- urinary fistula;
- inflammation of the perirenal tissues, which can lead to abscess and pyelosepsis;
- focal cicatricial changes (fibrosis) of the parenchyma with the development of obstructive nephropathy and severe renal failure;
- post-traumatic hydronephrosis;
- renal ischemia with nephrogenic hypertension;
- secondary pyelonephritis with pyonephrosis;
- formation of stones.
Diagnostics kidney rupture
In both traumatic and spontaneous renal ruptures, timely diagnosis based on visualization of the organ is very important.
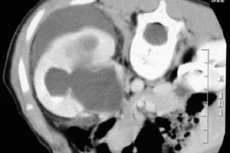
Therefore, instrumental diagnostics come first: X-ray of the kidneys and excretory urography; ultrasound of the kidneys and computed tomography (CT) with contrast. [ 9 ]
Conventional renal ultrasonography has certain limitations, since its sensitivity in such cases is no higher than 22%, and parenchyma damage may be isoechoic. Renal rupture on ultrasound shows heterogeneous echogenicity at the site of parenchyma damage, hematoma and accumulation of fluid component outside the kidney - in the retroperitoneal space. However, ultrasound cannot accurately differentiate blood from urine.
However, the sensitivity of contrast-enhanced ultrasound in detecting kidney damage is 63-69% and has a fairly high specificity (over 90%).
Today, in cases of acute kidney injury with its rupture, more complete anatomical and physiological information is provided by computed tomography (multispiral).
Magnetic resonance imaging (MRI) of the kidneys is performed if there are multiple injuries to the abdominal organs or if there are contraindications for the introduction of a contrast agent during CT.
Necessary tests: urine analysis and clinical blood test.
Differential diagnosis
CT is used to perform differential diagnostics with damage to other abdominal organs, in particular, the spleen, pancreas and liver.
Who to contact?
Treatment kidney rupture
The treatment tactics for kidney rupture are determined depending on the degree of organ damage and the patient's condition, including the hematocrit level.
Conservative treatment is used for minor parenchymal damage. It includes bed rest (for two to three weeks) with monitoring of vital signs and laboratory tests of urine and blood; calcium chloride (orally and by injection); intravenous administration of systemic antibiotics. Continued bleeding requires blood and plasma transfusion.
In case of deterioration of the general condition and in cases of more prolonged hematuria, angioembolization by means of X-ray vascular occlusion and drainage of the hematoma is effective, and in case of urine extravasation – drainage of the urinoma and, if necessary, endourological stenting. [ 10 ]
An initially high degree of kidney damage (determined upon admission of the patient), as well as hemodynamic instability and the presence of signs of internal bleeding are indications for emergency surgical intervention: an operation is performed to restore the kidney (by suturing the ruptures), surgical removal of the non-viable part of the kidney (resection) or - if the second kidney is intact - nephrectomy (removal), the frequency of which, according to some data, ranges from 3.5 to 9%. [ 11 ]
More information in the material - Kidney injuries and damage
Prevention
Preventive measures for kidney rupture include preventing injuries that lead to disruption of the anatomical integrity of the organ, as well as identifying and treating diseases that increase the risk of kidney damage.
Forecast
In each specific case, the prognosis depends on the degree of damage to the kidney during its rupture and on the timely provision of adequate medical care.