Medical expert of the article

New publications
Chest
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The thoracic cage (compages thoracis) is a bone-cartilaginous formation consisting of 12 thoracic vertebrae, 12 pairs of ribs and the sternum, connected to each other by joints, synchondroses, ligaments. The thoracic cage is the skeleton of the walls of the chest cavity, which contains the heart and large vessels, lungs, esophagus and other organs.
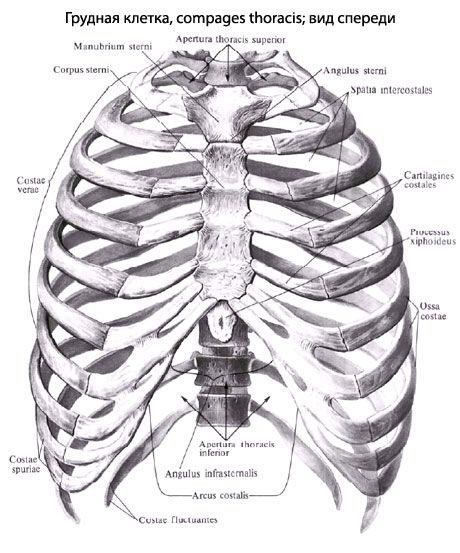
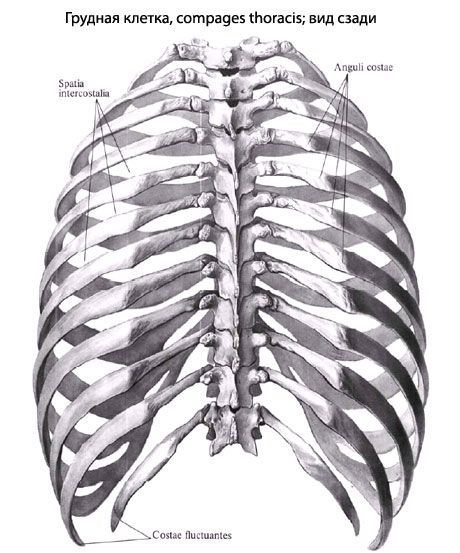
The thorax is flattened in the anteroposterior direction and has the shape of an irregular cone. It has 4 walls (anterior, posterior, lateral, and medial) and 2 openings (superior and inferior). The anterior wall is formed by the sternum and costal cartilages, the posterior wall by the thoracic vertebrae and the posterior ends of the ribs, and the lateral walls by the ribs. The ribs are separated from each other by intercostal spaces (spatia intercostalia). The superior opening (aperture) of the thorax (apertura thoracis superior) is limited by the 1 thoracic vertebra, the inner edges of the first ribs, and the upper edge of the manubrium of the sternum. The anteroposterior size of the superior aperture is 5-6 cm, the transverse size is 10-12 cm. The inferior aperture of the thoracic cage (apertura thoracis inferior) is limited at the back by the body of the 12th thoracic vertebra, at the front by the xiphoid process of the sternum, and on the sides by the lower ribs.
The median anteroposterior size of the inferior aperture is 13-15 cm, the largest transverse size is 25-28 cm. The anterolateral edge of the inferior aperture, formed by the junctions of the VII-X ribs, is called the costal arch (arcus costalis). The right and left costal arches in front limit the infrasternal angle (angulus infrasternalis), open downwards. The apex of the infrasternal angle is occupied by the xiphoid process of the sternum.
The shape of the chest depends on many factors, especially the body type. People with a brachymorphic body type have a conical chest. Its upper part is significantly narrower than the lower part, the substernal angle is obtuse. The ribs are slightly inclined forward, the difference between the transverse and anteroposterior sizes is small. With a dolichomorphic body type, the chest has a flattened shape. Its anteroposterior size is significantly smaller than the transverse one, the ribs are strongly inclined forward and downward, the substernal angle is acute. People with a mesomorphic body type are characterized by a cylindrical chest. In shape, it occupies an intermediate position between conical and flattened. In women, the chest is usually more rounded, shorter than in men. In newborns, the anteroposterior size of the chest prevails over the transverse size. In old age, the chest flattens, becomes longer. This is due to an age-related decrease in muscle tone and the lowering of the front ends of the ribs. Some diseases and professions affect the shape of the chest. Rickets increases the anteroposterior size of the chest, the sternum protrudes significantly forward ("chicken breast"). Trumpet players have a wide chest that is convex forward.
Chest movements
The movements of the chest are associated with breathing, i.e. with the processes of inhalation and exhalation. When inhaling, the front ends of the ribs rise together with the sternum. This leads to an increase in the anterior-posterior and transverse dimensions of the chest, an expansion of the intercostal spaces and a corresponding increase in the volume of the chest cavity. When exhaling, the front ends of the ribs and the sternum drop, the dimensions of the chest decrease, the intercostal spaces narrow. This leads to a decrease in the volume of the chest cavity.
The lowering of the ribs occurs not only due to the work of the corresponding muscles, but also due to the heaviness of the chest and the elasticity of the costal cartilages.
 [
[ What's bothering you?
What do need to examine?
How to examine?