Medical expert of the article

New publications
Percussion of the heart
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

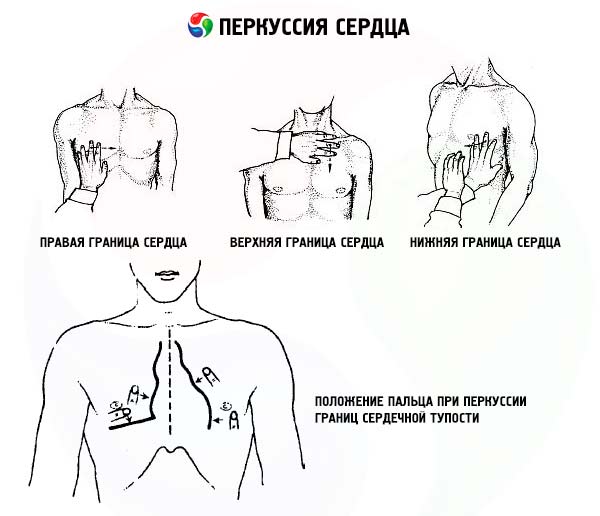
Percussion of the heart supplements the information obtained by palpation. In the area where the heart adjoins the anterior chest wall, dullness is determined by percussion. Since part of the heart contour is covered by the lungs, the percussion sound in this area will be less muffled than in the area where the heart directly contacts the chest wall, therefore, the so-called relative and absolute cardiac dullness are determined. When determining relative cardiac dullness, its right border is found at the level of the fourth intercostal space, along the edge and no further than 1 cm outward from the edge of the sternum. During percussion, the finger (pleximeter) is placed parallel to the desired border and moved along a line perpendicular to it.
The left border of relative cardiac dullness is determined near the apical impulse, and if it is absent, in the fifth intercostal space (percussion is performed in the fifth intercostal space from the anterior axillary line towards the sternum). The left border of relative cardiac dullness is located 1 cm inward from the left midclavicular line.
To determine the upper limit of relative cardiac dullness, the finger-pleximeter is moved along a line parallel to the edge of the sternum, starting to percuss from the 2nd rib. Normally, the upper limit of relative cardiac dullness corresponds to the lower edge of the 3rd rib or the third intercostal space.
The boundaries of absolute cardiac dullness correspond to the following landmarks: left - 1-2 cm inward from the boundary of relative cardiac dullness, right - along the left edge of the sternum at the level of the fourth intercostal space, upper - the fourth intercostal space. When determining these boundaries, percussion begins from the center of the zone of absolute cardiac dullness, percussion blows are made very softly so that the sound in the area of absolute dullness is practically inaudible. In this case, upon reaching the boundary between absolute and relative dullness, the percussion sound becomes audible.
The boundaries of the vascular bundle are determined at the level of the second intercostal space. The finger-pleximeter is moved along a line perpendicular to the edge of the sternum. Quiet percussion is also used. The boundaries of the dullness of the vascular bundle normally correspond to the edges of the sternum.
The right contour of relative cardiac dullness and vascular bundle is formed, starting from above, i.e. from the second intercostal space, by the superior vena cava, then by the right atrium. The left contour of relative cardiac dullness is formed by the aortic arch, then by the pulmonary artery at the level of the third rib, the left atrial appendage, and below by a narrow strip of the left ventricle. The anterior surface of the heart in the area of absolute dullness is formed by the right ventricle.
The informativeness of the data obtained during the examination of the precordial region is currently assessed quite critically. This is due to the fact that as a result of the frequently occurring pulmonary emphysema, most of the heart is covered by the lungs, and determining the boundaries of relative and absolute dullness is practically impossible. The displacement of the apical impulse and the left border of the heart outward can often be associated with an increase in various chambers of the heart, but not the left ventricle. A significant increase in cardiac dullness during percussion is found with a large pericardial effusion. A significant upward displacement of the border can occur with an increase in the left atrium as a result of mitral defects. Expansion of the vascular bundle is observed with an aortic aneurysm.
The impression obtained during the study of the precordial zone is confirmed by the results of modern, highly informative methods, primarily echocardiography.
 [
[