Medical expert of the article

New publications
Arthrotomy
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Exposure of the joint and opening of its cavity is performed surgically, and this manipulation in orthopedic and traumatological surgery is defined as arthrotomy, which can be performed using various surgical approaches. [ 1 ]
Indications for the procedure
Indications for arthrotomy are the need for any operation on joints that requires access to their structures – for the surgical elimination of existing problems in patients, in particular:
- joint fracture, which requires open reposition of bone fragments and their internal fixation in the correct position;
- ligament ruptures - for their reconstruction;
- accumulation of purulent exudate in the joint capsule in inflammatory joint diseases. For example, arthrotomy in purulent arthritis or synovitis of any joint, purulent bursitis of the knee joint, shoulder or elbow joints is performed to remove pus from the joint cavity - drainage, when there is no improvement after arthrocentesis (intra-articular puncture).
It is impossible to do without wide surgical access to the joint:
- when removing osteophytes, bone and cartilage fragments, intra-articular cysts or tumors;
- when excision of the synovial membrane is required - synovectomy of joints, which can be resorted to in cases of rheumatoid and reactive arthritis, osteoarthrosis, osteochondromatosis;
- in cases of intra-articular arthrodesis – artificial stabilization of a joint in case of its deformation or pathological mobility;
- in arthroplasty – restoration of joint mobility in patients with ankylosis or congenital articular defects;
- if the installation of joint implants is planned – joint endoprosthetics.
Preparation
As a rule, surgical intervention on joints is carried out on a planned basis, therefore all necessary examinations are carried out at the stage of identifying and determining the problems that patients have – clinical diagnostics of joints – and choosing a treatment strategy. Often, orthopedic surgery becomes inevitable when medication and physical therapy are ineffective. [ 2 ]
Before an arthrotomy operation performed in a clinical hospital setting, preparation necessarily includes clarification of the condition of a specific joint, for which its preoperative visualization is carried out: X-ray, ultrasound, CT or MRI.
Patients also undergo a general blood test; tests for hepatitis, RW and HIV; a coagulogram and a general clinical analysis of synovial fluid.
A week before the surgery, you should stop taking anticoagulants, including those containing acetylsalicylic acid, and your last meal should be no less than 10-12 hours before the surgery.
Technique arthrotomies
The technique for performing this surgical manipulation depends on the specific diagnosis, the purpose of the intervention and the access method used by the surgeon on various joints, which have their own characteristics of bone and ligament anatomy. [ 3 ]
To provide pain relief for the operation (depending on its volume and location), both general anesthesia and regional or local anesthesia are used.
Arthrotomy of the hip joint
For surgical drainage of septic arthritis of the hip joint or performing synovectomy in cases of synovitis of the hip joint, the following standard approaches are used: Smith-Petersen arthrotomy - anterior (iliofemoral) approach; Watson-Jones anterolateral approach; Langenbeck posterolateral approach - with an incision of soft tissues from the posterior superior iliac spine to the greater trochanter (the tubercle at the top of the femur - Trochanter major) and opening the joint capsule with a T-shaped incision.
In total hip arthroplasty, the most common approaches are posterior, direct anterior, and direct lateral. For example, direct lateral hip arthrotomy is an incision that the surgeon begins making 3 cm closer to the middle third of the greater trochanter, continues along the line of the femur to its tubercle (several centimeters short of it); an incision of the skin and subcutaneous tissues is made to the Fascia lata (wide fascia of the thigh), which is also longitudinally incised in front of the lateral protrusion of the Trochanter major. Next, to reach the joint capsule, the gluteal muscles (m. gluteus medius and m. gluteus maximus) are exposed and separated by blunt dissection at the level of the greater trochanter.
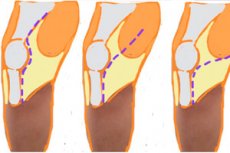
Arthrotomy of the knee joint
Depending on the diagnosis and the purpose of the surgical intervention, knee joint arthrotomy can be performed using different techniques: Langenbeck, Tieling, Textor. [ 4 ]
Thus, Textor's arthrotomy is performed by making a transverse arc-shaped incision that begins at one condyle of the femur and ends at the opposite one - below the patella (kneecap), with the intersection of the patellar ligaments (Retinaculum patellae mediale and Ligamentum patellae).
Arthrotomy according to Voino-Yasenetsky or arthrotomy through the lateral parapatellar approach is performed using two longitudinal incisions on the sides of the kneecap.
In case of meniscus rupture, for removal of the patella, and also for total arthroplasty in cases of osteoarthritis of the knee joint (gonarthrosis), medial parapatellar arthrotomy is used to access the joint. In this case, four incisions are made: two anterior longitudinal ones - on both sides of the patella, one through the lateral supporting ligament and another longitudinal one - above the edge of the upper part of the patella to the middle of the border of the Tuberculum medialis (medial tubercle of the tibia). [ 5 ]
Ankle arthrotomy
Surgical fixation of a fracture with displacement in the area of the external or internal malleolus is recognized as the most adequate surgical treatment, ensuring normal biomechanics of the ankle joint after such injuries.
Surgical approaches to ankle arthrotomy: anterior (medial) and anterolateral, lateral and posterolateral.
With the anterior approach, the skin and subcutaneous tissue above the joint are dissected along the midline of the leg – along the tibia (os tibia) and fibula (os fibula) bones with a vertical dissection of the aponeurosis of the leg between the tendons of the long extensors of the fingers and the big toe – with the isolation and protection of the branches of the peroneal nerve (cutaneous and deep), as well as the vessels of the dorsum of the foot. The incision can be made medial to the tendon of the anterior tibial muscle with its lateral abduction (together with the vascular-nerve bundle). Then the joint capsule is incised and the joint is exposed.
Lateral arthrotomy of the ankle joint is performed by an incision in front of or behind the lateral edge of the fibula with its continuation between the muscles of the lower leg - m. peroneus tertius (fibular) and m. peroneus longus (long fibular).
Arthrotomy with a posterior approach - through an incision along the posterolateral border of the calcaneal (Achilles) tendon to its insertion on the calcaneus; two longitudinal incisions can also be made - on both sides of the Achilles tendon. The use of this technique gives the surgeon access to the distal end of the tibia, the back of the ankle, the posterior end of the talus and the talocalcaneal joint.
Arthrotomy of the shoulder joint
Opening the joint cavity for drainage, according to clinical experience, is a more effective method of treating septic arthritis of the shoulder joint; arthrotomy is also used in cases of chronic or habitual shoulder dislocation.
Anterior arthrotomy of the shoulder joint (according to Langenbeck) or deltopectoral approach is performed by an incision that starts from the anterior surface of the lateral end of the scapula (acromion) and then descends approximately 8 cm along the anterior edge of the middle bundle of the deltoid muscle of the shoulder (m. deltoideus) - with dissection of the fascia (to the articular tendon) and division of the muscle by blunt dissection. The joint capsule is exposed after stretching the muscle fibers and dissection of the long tendon of the caput longum (long head) of the biceps brachii muscle passing through the shoulder joint.
Access to the shoulder joint can be anterolateral, when the incision also starts from the acromion, but then goes down along the inner edge of the biceps brachii muscle - along its medial groove (sulcus bicipitalis medialis).
Arthrotomy of the elbow joint
In the Langenbeck elbow arthrotomy, the soft tissues on the dorsal surface of the joint are cut longitudinally - from the lower third of the humerus to the upper third of the forearm; the olecranon process is transected transversely and the medial epicondyle of the humerus is cut off.
Arthrotomy can be performed by cutting between the posterior forearm muscle, the extensor carpi ulnaris (m. extensor carpi ulnaris), and the anconeus muscle. The incision is made along the line connecting the lateral epicondyle of the humerus and the border between the proximal and middle thirds of the ulna. The incision is stretched and the common fascia of the extensor carpi ulna is cut; the tendon of the upper part of the anconeus muscle is exposed, the origin of the extensor carpi ulnaris is disconnected from the lateral epicondyle and the muscles are pulled back to expose the anterolateral surface of the joint capsule. It is cut along the anterior edge of the radial collateral ligament of the elbow joint (collaterale radiale) - from the lateral epicondyle to the annular ligament of the radius.
Contraindications to the procedure
There are such contraindications for arthrotomy as:
- infectious and acute inflammatory diseases with fever;
- exacerbation of chronic diseases;
- infections of the tissues surrounding the joint;
- thrombocytopenia and decreased blood clotting;
- severe cardiac and pulmonary failure;
- deep vein thrombophlebitis – during interventions on the joints of the lower extremities.
Consequences after the procedure
The consequences of this operation include:
- development of inflammation of the inner lining of the joint capsule – synovitis;
- formation of blood clots in the veins of the lower extremities;
- gradual formation of ossifications in the soft tissues adjacent to the operated joint;
- skin necrosis caused by deterioration of blood supply in the area of surgical intervention;
- muscle tissue atrophy;
- joint contractures and limitation of their mobility due to fibrous adhesions and scars.
During arthrotomy of the knee joint, there is a risk of damage to the branches of the common peroneal nerve and the popliteal branches of the saphenous nerve with the development of a postoperative tumor - neuroma. In addition, during this operation - due to excessive stretching of the joint capsule and surrounding tissues - a tear of the patellar tendon from the tibia is possible. [ 6 ]
Complications after the procedure
As with any surgical procedure, complications may occur following arthrotomy, including:
- infection of a surgical wound with the development of an inflammatory process;
- allergic reaction to anesthesia;
- prolonged or constant pain around the joint.
Complications after arthrotomy may be in the form of a hematoma of the periarticular tissues, they may also be associated with damage to blood vessels (with bleeding) or nerve branches. For example, as a result of exposure of the shoulder joint, there is a risk of alteration of the posterior circumflex humeral artery or nerves - suprascapular or axillary. [ 7 ]
Care after the procedure
After arthrotomy, care consists of splinting the operated joint (in case of surgery on the shoulder or elbow joint, an immobilizing orthosis may be used), antiseptic treatment of postoperative sutures, and the administration of antibacterial, anti-inflammatory, analgesic, thrombolytic and anti-edematous drugs.
The duration of immobilization depends on both the initial diagnosis and the extent of the surgery. [ 8 ]
Rehabilitation after arthrotomy is a fairly lengthy process with mandatory therapeutic exercise and various physiotherapeutic procedures. The degree of restoration of the normal range of joint motion varies depending on the condition of each patient.