Medical expert of the article

New publications
Shingles
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Shingles (Herpes zoster, shingles, zona) are the result of the reactivation of the varicella-zoster virus from the latent state in the ganglia of the posterior roots of the spinal cord.
Acute CNS damage; is characterized by vesicular rashes and neuralgic pains in the areas of the skin innervated by peripheral sensory nerves ascending to the affected ganglia. Treatment of herpes zoster includes antiviral drugs and, possibly, glucocorticoids up to 72 hours after the onset of rashes.
Epidemiology
People who had previously suffered chicken pox are ill. Shingles - a secondary endogenous infection in relation to chicken pox.
Shingles are observed in people of all age groups - from children of the first months of life to people of elderly and senile age who had previously transferred chicken pox. 75% of cases are for people over 45, while children and adolescents are less than 10%. The incidence is 12-15 per 100 000 population. Patients with shingles are considered a source of infection for those who did not suffer from chicken pox. The index of contagiosity is not higher than 10%, because unlike chicken pox, the virus on the surface of the mucous membrane of the respiratory tract is not detected continuously.
Cases of the herpes zoster are recorded throughout the year, the season has no pronounced seasonality.
Causes of the shingles
Shingles caused by the same virus as chicken pox (human herpes virus - type 3). Varicella is an acute invasive phase of the virus, herpes zoster (shingles) is the reactivation of the latent phase. There are inflammatory changes in the spinal ganglia and associated dermatomes. In some cases, the inflammatory process captures the hind and fore horns of gray matter, soft meninges, back and front roots. Activation of the pathogen leads to local lesions affecting the ganglia of the posterior roots of the spinal cord; systemic diseases, especially Hodgkin's disease; reception of immunosuppressants. Disease shingles occurs at any age, most often in the elderly, HIV-infected patients; most heavily occurs in immunocompromised individuals. Sometimes the causes of herpes zoster are unknown.
Pathogens
Pathogenesis
Tinea develops as a secondary endogenous infection in persons who have suffered varicella in a clinically expressed, erased or latent form due to the reactivation of the Varicella zoster virus, integrated into the genome of cells in the cranial and spinal sensory ganglia. The interval between primary infection and clinical manifestations of herpes zoster is tens of years, but may be short and can be several months. The mechanism of reactivation of the varicella-zoster virus has not been sufficiently studied. Risk factors include the elderly and senile age. Associated diseases, especially oncological, hematological, HIV infection, drug addiction, use of glucocorticoids, cytostatics, radiation therapy. The risk group includes recipients of transplant organs. Reactivation of the virus can be triggered by stressful conditions, physical trauma, hypothermia, infectious diseases, alcoholism. Reactivation of the virus is associated with conditions accompanied by immunosuppression, especially with partial loss of specific immunity.
As a result of the activation of the varicella zoster virus (Varicella zoster virus), ganglionvritis develops with damage to the intervertebral ganglia, ganglia of the cranial nerves and damage to the posterior roots. The process can involve autonomic ganglia, substance and membranes of the brain and spinal cord. Internal organs can be affected. Spreading centrifugally along the nerve trunks, the virus enters the epidermal cells and causes inflammatory-degenerative changes in them, which is manifested by corresponding rashes within the zone of innervation of the corresponding nerve, i.e. Dermatome. It is possible and hematogenous spread of the virus, as evidenced by the generalized form of the disease, polyorganism lesions.
The pathoanatomical picture of the herpes zoster is caused by inflammatory changes in the spinal ganglia and associated parts of the skin, as well as in the hind and anterior horns of the gray matter, the posterior and anterior roots of the spinal cord and the soft meninges. The morphology of the vesicles is identical to that of chicken pox.
Symptoms of the shingles
3-4 days before the symptoms of herpes zoster appear such prodromal signs as chills, fever, malaise and gastrointestinal disorders. However, in the area of future rashes, pain can be felt. Approximately on the 3-5th day in the zone of innervation of one or several spinal ganglia, characteristic accumulations of vesicles appear on the erythematous base. In the affected area, hyperesthesia is usually noted, and the pain can be severe. Eruptions appear most often in the thoracic region and spread along one side of the body. Approximately 5 days after the appearance of the bubbles begin to dry out with the formation of a scab. The lesion can become generalized, with lesions of other skin areas and visceral organs, especially in immunocompromised patients.
The first episode of herpes zoster usually creates immunity (recurrence is noted in no more than 4% of cases). However, postherpetic neuralgia can persist for months and years, especially in old age. Infection of the trigeminal nerve leads to a strong permanent pain. Pain in postherpetic neuralgia can be acute, persistent or episodic, debilitating.
In adults, the earliest symptoms of herpes zoster are the appearance of radicular pain. Pain can be intense, has a paroxysmal nature, often accompanied by local hyperesthesia of the skin. In children, pain syndrome is less pronounced and occurs 2-3 times less often. In the prodromal period, the appearance of rashes is preceded by such symptoms of herpes zoster as weakness, malaise, fever, cognition, pain in the muscles and joints, headache. In the area of affected dermatome, there may be a feeling of numbness, tingling, or burning. The duration of the prodromal period varies from 1 to 7 days.
Symptoms of herpes zoster during the period of clinical signs are characterized by skin and / or mucous membrane damage, intoxication and neurological symptoms.
Vesicles are considered the main element of local and generalized skin rashes with shingles, they develop in the germ layer of the epidermis.
First, the exanthema has the appearance of a pink-red spot, which quickly turns into closely grouped vesicles ("bunches of grapes") with transparent serous contents, located on the hyperemia and edema base. Their size does not exceed a few millimeters. The contents of the vesicles quickly grow turbid, then the condition of the patients improves, the temperature normalizes, the vesicles dry up and become crusted, after which there is no scar left. Complete healing occurs within 2-4 weeks. In herpes zoster, the rash has a segmental, one-sided character, usually capturing 2-3 dermatomes. The predominant localization of skin lesions with shingles is noted in the innervation zone of the trigeminal nerve branches, then, in a decreasing sequence, in the region of the thoracic, cervical, lumbosacral, cervico-thoracic segments. In 10% of patients, the distribution of exanthem is observed beyond the boundaries of affected dermatomes. Dissemination may be accompanied by the appearance of multiple or single elements of the rash, with a shorter period of reverse development. Genitalization of the exanthema is noted 2-7 days after the onset of rash in the area of the dermatome, it may be accompanied by a worsening of the general condition. In addition to typical vesicular rashes, in weakened patients, exanthema can be transformed into a bullous form, acquire a hemorrhagic character and be accompanied by necrosis. Necrotic eruptions are observed in persons with immunodeficiency (HIV infection, oncological diseases). In these cases, rashes remain on the site of the rashes. In the zone of rashes, the prevalent flushing of the skin is determined, the edema of the underlying tissues is expressed. When localizing the rash in the zone of the first branch of the trigeminal nerve, a marked edema is often observed. Exanthemum is accompanied by an increase and a moderate soreness of the regional lymph nodes. Children may have signs of acute respiratory disease. Elevated body temperature lasts several days, accompanied by mild symptoms of intoxication. In this period of the disease, cerebral and meningeal symptoms of herpes zoster in the form of adynamia, drowsiness, diffuse headache, dizziness, vomiting are possible. Symptoms of shingles appear on average 2-3 weeks.
Postherpetic neuralgia develops immediately after 2-3 weeks after the illness. Pain, as a rule, is paroxysmal and intensifies at night, becoming unbearable. Severity of pain after a while decreases, or it completely disappears within a few months. Chronicity of postherpetic neuralgia is rarely seen only in immunocompromised individuals.
Shingles can only occur with symptoms of radicular pain, with single vesicles or without any rashes. The diagnosis in such cases is established on the basis of the increase in antibody titres to the varicella zoster virus (Varicella zoster virus).
Repeated cases of shingles are characteristic for patients with HIV infection or oncological diseases (leukemia, lung cancer). With this, the localization of the rash may correspond to the localization of the tumor, so the secondary herpes zoster is considered a signal for an in-depth examination of the patient. In the pathology of herpes zoster, eye damage (keratitis) occupies a significant place, which determines the severity of the disease and causes the patients to be transferred to the ophthalmologic department.
Stages
Shingles are divided into four periods:
- prodromal (prehepatic neuralgia);
- stage of herpetic rashes;
- convalescence (after the disappearance of exanthema);
- residual phenomena.
 [22]
[22]
Forms
Tinea can flow in a mild, moderate and severe form. Possibly abortive or protracted course. Criteria for severity are the severity of intoxication, signs of CNS damage, the nature of local manifestations (the type of exanthema, the intensity of the pain syndrome).
Herpes of the cranial node of the facial nerve (Ramsay-Hunt syndrome) develops when the cranial nodule of the facial nerve is affected and is characterized by pain in the ear, paralysis of the facial nerve, and sometimes vestibular disorders. Vesicular rashes appear in the external auditory canal, in the anterior third of the tongue, taste can be lost.
Ophthalmoherpes - the eye form of herpes zoster, develops in the defeat of the ganglion of the trigeminal nerve - gasser node, characterized by pain and vesicular rashes along the eye branches of the V nerve, around the eyes. Bubbles at the tip of the nose (Hutchinson's symptom) reflect the defeat of the nasociliary branch of the V nerve. It should be remembered that eye damage can develop in the absence of nose tip damage.
Herpes mucosa of the oral cavity is infrequent, but can cause acute one-sided lesion; prodromal symptoms of herpes zoster are usually absent.
In the structure of clinical manifestations of shingles, a significant place is occupied by a variety of syndromes affecting the central and peripheral parts of the nervous system.
Sensory disorders in the zone of rashes: radicular pain, paresthesia, segmental disorders of surface sensitivity are constantly observed. The main symptom - local pain, the intensity of which varies widely. Pain has a pronounced vegetative color (burning, paroxysmal, intensifying at night). Often it is accompanied by emotional and affective reactions.
Radicular paresis is topically confined to certain zones of eruptions: lesions of the oculomotor nerves, facial nerve (variants of the Hunt syndrome), paresis of the upper limbs, abdominal wall muscles, lower extremities, sphincter of the bladder. These symptoms of herpes zoster develop, as a rule, on the 6th-15th day of the disease.
Poliradiculoneuropathy is a very rare syndrome in patients with shingles; only a few dozen observations are described.
Serous meningitis is one of the main syndromes in the herpes zoster picture. In the study of cerebrospinal fluid in early terms, there are two- or three-digit lymphocytic or mixed pleocytosis, including in the absence of cerebral and meningeal phenomena (clinically "asymptomatic" meningitis).
Encephalitis and meningoencephalitis are observed in an acute period. Symptoms of CNS damage occur on the 2-8th day of rashes in the dermatome. CT scan reveals foci of destruction of the brain tissue from the 5th day of encephalitis.
Diagnostics of the shingles
To recognize shingles in the prodromal period is difficult, but after the appearance of characteristic rashes, the diagnosis does not cause difficulties. Diagnosis of herpes zoster is based on the recognition of a typical rash. If the diagnosis is doubtful, it is possible to perform a Tzank test with detection of multinucleated giant cells. Sometimes the herpes simplex virus can cause almost the same lesions that occur in herpes zoster. However, herpes simplex, as a rule, gives relapses, and herpes zoster recurs rarely, rashes are located along the course of dermatomes. Viruses can be identified by cultivation and analysis of a biopsy material.
For laboratory confirmation of the diagnosis, virus antigen detection is used with microscopy or with the help of immunofluorescence method, serological diagnosis of herpes zoster. PCR is promising.
What do need to examine?
What tests are needed?
Differential diagnosis
Diagnosis of herpes zoster in the vast majority of cases does not cause difficulties. The leading position retains clinical criteria, the main of which is the presence of a characteristic exanthema with a kind of segmental topography, almost always one-sided.
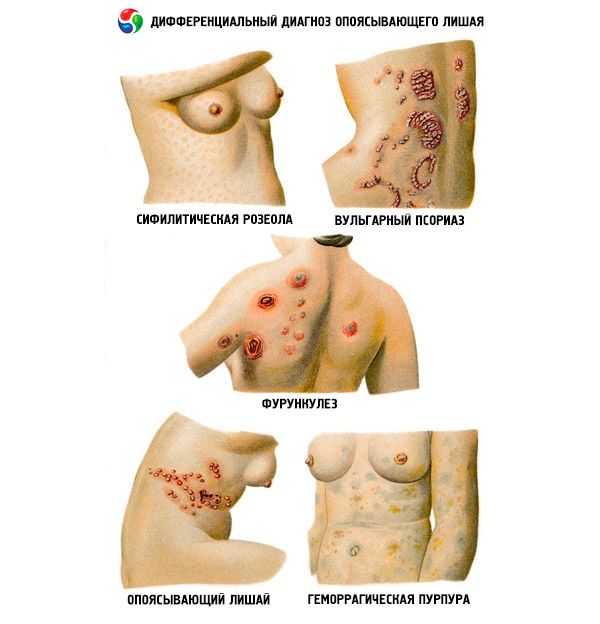
In some cases, differential diagnosis of herpes zoster is carried out with zosteriiform simple herpes. Bullion form of herpes zoster is differentiated with erysipelas, skin lesions with oncological, hematological diseases, diabetes and HIV infection.
Who to contact?
Treatment of the shingles
Hospitalized patients with severe shingles. In compulsory hospitalization, patients with a generalized form of the infectious process, a defeat of the first branch of the trigeminal nerve and CNS, need it.
Tinea is treated with local means that have a calming effect, for example wet compresses, sometimes systemic analgesics. The use of antiviral drugs can reduce the strength and frequency of acute rashes, the frequency of serious impairment in immunocompromised individuals and pregnant women. Treatment of herpes zoster should begin as early as possible, ideally in the prodromal period; it is ineffective if it begins more than 72 hours after the appearance of the first elements of the rash. Apply famciclovir 500 mg orally 3 times a day for 7 days and valaciclovir 1 g orally 3 times a day for 7 days: these drugs have better bioavailability compared with acyclovir ingested (at a dose of 800 mg 5 times a day within 7-10 days) and therefore is preferable. Glucocorticoids help to speed recovery and relief of acute pain, but do not reduce the frequency of postherpetic neuralgia.
Immunocompromised patients are recommended to administer acyclovir 10 mg / kg intravenously every 8 hours for 7 days for adults and 500 mg / m2 intravenously every 8 hours for 7-10 days in children older than 1 year.
Prevention of primary infection is carried out by vaccination of children and sensitive persons. A pronounced booster effect of the vaccine in elderly people who previously had chicken pox (a decrease in the number of cases of the disease) is shown.
Treatment of postherpetic neuralgia sometimes presents considerable difficulties. Apply gabapenin, cyclic antidepressants, local ointments with lidocaine or capsaicin. Sometimes opioid analgesics may be needed. Sometimes the intrathecal use of methylprednisolone is effective.
Pathogenetic treatment of herpes zoster involves the appointment of dipyridamole as a disaggregant at 50 mg 3 times a day, 5-7 days. Dehydration treatment of herpes zoster (acetazolamide, furosemide) is shown. It is advisable to appoint immunomodulators (prodigiozan, imunofan, azoxime bromide, etc.).
In postherpetic neuralgia, NSAIDs (indomethacin, diclofenac, etc.) are used in combination with analgesics, sedatives and physiotherapy. Vitaminotherapy (B1, B6, B12) is possible, it is preferable to carry out a lipophilic modification of vitamins - milgamma "N", which has a higher bioavailability.
In severe cases with severe intoxication, a detoxification treatment of the herpes zoster with intravenous administration of rheopolyglucin, infucol is carried out, dehydration is increased, anticoagulants, corticosteroid hormones are used in small doses. Locally - 1% solution of brilliant green, 5-10% potassium permanganate solution, in the phase of crusts - 5% ointment of bismuth subgallate; at slow processes - methyluracil ointment, solcoseryl. Antibiotics are prescribed only by the patient with shingles with signs of activation of the bacterial flora.
In general, the therapeutic strategy is determined by the stage and severity of the process, the peculiarities of the clinical course of herpes zoster, the general condition and age of the patient.
When treating ophthalmoherpes, consultation of an ophthalmologist, ear herpes - otorhinolaryngologist is necessary.
Approximate terms of incapacity for work
7-10 days.
Clinical examination
Clinical follow-up at a severe course of the disease and the presence of complications for 3-6 months.
Memo for the patient
It is necessary to avoid hypothermia and other stressful conditions, to limit physical activity, to eat in a balanced way. It is also necessary to check the condition of the immune system.