
Ovarian hyperstimulation syndrome
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Ovarian hyperstimulation syndrome (OSS) is an iatrogenic complication based on a hyperergic uncontrolled ovarian response to the administration of gonadotropins in ovulation stimulation cycles and assisted reproductive technologies.
The syndrome can manifest after induction of ovulation with clomiphene or at the onset of pregnancy in a spontaneous cycle.
 [1],
[1],
Epidemiology
The frequency of ovarian hyperstimulation syndrome varies from 0.5 to 14% with different schemes of ovulation stimulation and does not tend to decrease. The disease proceeds with varying degrees of severity and may result in death in connection with the development of thromboembolic complications or ARDS. The expected lethality is 1 for 450-500 thousand women. Heavy forms of the syndrome, requiring hospitalization in the intensive care unit, are met in 0.2-10%. According to the Russian National Register of Methods of Assistive Reproductive Technologies, the frequency of acute hypoxia in 2004 was 5.6%.
Causes of ovarian hyperstimulation syndrome
Risk factors for the development of ovarian hyperstimulation syndrome:
- age less than 35 years,
- asthenic physique,
- the presence of polycystic or multifollicular ovaries,
- maturation of more than ten follicles in the protocol of stimulation of ovulation,
- use of gonadotropin-releasing hormone agonists and high doses of gonadotropins,
- the onset of pregnancy,
- support of luteal phase with drugs HG,
- allergic diseases.
How does the ovarian hyperstimulation syndrome develop?
Ovarian hyperstimulation syndrome occurs against the background of an abnormally high concentration of sex hormones in the blood plasma, which negatively affects the functions of various body systems, primarily the ovaries, and characterizes the increase in the size of the ovaries, sometimes up to 20-25 cm in diameter, with the formation of follicular and luteal cysts against the background of pronounced edema of the stroma. The triggering factor of the syndrome is the introduction of the ovulatory dose of the chorionic gonadotropin. The phenomenon of "increasing vascular permeability" is the basis of the syndrome development, leading to a massive release of protein-rich fluid into the third space, interstitium and its deposition with the development of hypovolemia, hemoconcentration, oliguria, hypoproteinemia, electrolyte imbalance, increased activity of liver enzymes, formation of ascites, hydrothorax, hydropericardia with or without hypovolemic shock phenomena. However, the "factor X" leading to fluid transudation remains unknown. In severe cases anasarca, arthritis, thromboembolic complications, ARDS occur.
Currently, the ovarian hyperstimulation syndrome is considered from the SSVR perspective, against which there is a massive damage to the endothelium. In patients with CHOS in the peritoneal transudate, high concentrations of interleukins (IL-1, IL-2, IL-6, IL-8), tumor necrosis factors (TNF-a, TNF- (3), enhancing the synthesis of prostaglandins by the ovaries, neovascularization of the ovary and vascular permeability.In the action of proinflammatory cytokines, systemic activation of coagulation processes occurs.The magnitude of leukocytosis correlates with the severity The role of the microbial factor in HNS and its contribution to the development of SSRM is currently being discussed, and it is suggested that microorganisms colonizing the intestine, genito-urinary tract, can penetrate beyond their habitat and have an effect on the body, similar to that of sepsis.
Symptoms of ovarian hyperstimulation syndrome
The severity of the syndrome is directly related to the severity of hemodynamic disorders that determine the clinical picture. The onset of the development of the syndrome can be gradual with an increase in symptoms and sudden (acute), in which for a few hours there is a sharp redistribution of fluid in the body with accumulation in the serous cavities. When the syndrome manifests, complaints of weakness, dizziness, headache, flashing of the "flies" before the eyes, dyspnea at rest and with physical exertion, dry cough, worse lying down, dry mouth, nausea, vomiting, diarrhea, bloating, feeling tension, abdominal pain often without clear localization, rare urination, fever, swelling of the vulva and lower limbs.
Patients with ovarian hyperstimulation syndrome may develop respiratory failure as a result of the limitation of lung mobility due to ascites, ovarian enlargement or the presence of effusion in the pleural cavities. The course of acute hypoglycemia in the stage of manifestation may complicate acute hydrothorax, ARDS, PE, AL, atelectasis, as well as intra-alveolar bleeding. Exudation in the pleural cavity is diagnosed in about 70% of women with moderate to severe hypoglycemia, while the effusion can be unilateral or bilateral and occurs on the background of ascites. With SHH, displacement and compression of the mediastinal organs are described as a result of massive right-sided pleural effusion with development of shock, as well as death in a woman with HH and hydrothorax due to AL, massive hemorrhage into the alveolar lumen.
Hemodynamic disorders. With HSH of medium and severe degree arterial hypotension, tachycardia.
Ascites. The abdomen is swollen, often tense, painful in all parts, but more often in the hypogastrium in the projection of the ovaries.
Impaired kidney and liver function. Observed delay urination, oliguria, anuria, hepatomegaly.
The course of CHD in 80% of patients with severe syndrome is accompanied by fever. In 20% of women, fever occurs against the urinary tract infection, 3.8% - due to pneumonia, and 3.3% - infection of the upper respiratory tract. Thrombophlebitis due to the installation of an intravenous catheter causes fever in 2%, inflammation of subcutaneous fat at the abdominal puncture site with laparocentesis - in 1% of patients. Infection of the operating wound occurs in 1%, and postinjection abscesses (intramuscular injection of progesterone) in 0.5%. Fever of non-infectious genesis in every second patient with CHD is probably associated with endogenous pyrogenic mechanisms. Single cases of sepsis are described in the severe course of SWS.
Against the background of the development of the syndrome there is an exacerbation of latently current chronic somatic diseases.
What's bothering you?
Classification
There is no uniform classification of the ovarian hyperstimulation syndrome. On the basis of clinical and laboratory symptoms four degrees of severity of the syndrome are distinguished:
- СГЯ of an easy degree. Abdominal discomfort, ovaries up to 8 cm in diameter with or without cysts, laboratory performance in normal HSH of a mild degree is called "controlled ovarian hyperstimulation", since this condition is observed absolutely in all cycles of stimulation of superovulation and is not currently regarded as a pathological syndrome, requiring treatment.
- СГЯ of an average degree. Moderate pain in all parts of the abdomen, nausea, vomiting, diarrhea, ovaries 8-12 cm in diameter with cysts, ultrasound and / or clinical signs of ascites, hematocrit does not exceed 45%, leukocytosis - 10-16x10 9 / L, hypercoagulability (D- dimer - more than 0.5 μg / ml, fibrinogen concentration - more than 400 mg / dl, APTT, MNO - within the limits of the norm).
- HHS severe. Hematocrit is more than 45%, leukocytosis is 17-24x10 9 / L, hypercoagulability (D-dimer is more than 5 μg / ml, fibrinogen is more than 600 mg / dL), ovaries more than 12 cm in diameter with cysts, all clinical and laboratory signs of HHS of medium degree and tension ascites, hydrothorax, liver dysfunction, oliguria [diuresis less than 0.5 ml / (kg h)].
- OSS of a critical degree. Hematocrit more than 55%, leukocytosis more than 25х109 / l, intense ascites, bilateral hydrothorax, hydropericardium, anasarca, ovarian enlargement to 20-25 cm, oliguria or anuria, arthritis, thromboembolic complications, ARDS.
Also, the syndrome of ovarian hyperstimulation is divided into early and late.
If SHH occurs in the luteal phase and implantation does not occur, the syndrome abruptly and spontaneously disappears with the onset of menstruation, rarely reaching a severe form. If the implantation occurs, the deterioration of the patient's condition during the first 12 weeks of pregnancy is most often observed. Late CGR is caused by a significant increase in CG in blood plasma and is usually associated with implantation and early pregnancy.
Consequences and complications
Complications of the ovarian hyperstimulation syndrome can occur with the development of thromboembolic complications. The cause of thrombosis with CHD remains unknown, but the main role in the pathogenesis of this condition is attributed to high concentrations of sex hormones, proinflammatory cytokines, hemoconcentration, and a decrease in VCP. Long periods of hospitalization, restriction of motor activity, a decrease in venous return due to ovarian enlargement, an increase in the activity of coagulation factors, inhibitors of fibrinolysis and platelets make an additional contribution to the high risk of thrombotic complications in connection with OHSS. It was demonstrated that in 84% of patients with thromboembolic complications that occurred after induction of ovulation and in programs of assisted reproductive technologies, their development occurred against the background of pregnancy. In 75% of cases, thrombus formation in the venous channel with predominant localization in the vessels of the upper extremities, neck and head 60%). In a number of patients, spontaneous arterial thrombosis was diagnosed with localization in the vessels of the brain. Less often noted the formation of thrombi in the femoral, popliteal, carotid, subclavian, iliac, ulnar, mesenteric arteries and aorta. In the literature, the development of occlusion of the central artery of the retina with loss of vision is observed in patients with ovarian hyperstimulation. The incidence of pulmonary embolism in patients with CHD and deep vein thrombosis of the lower limbs is 29%, while in women with OHSS and deep vein thrombosis of the upper extremities and arterial thrombosis the risk of this complication is significantly lower and is 4% and 8%, respectively.
The severe course of the ovarian hyperstimulation syndrome may be accompanied by complications requiring surgical intervention - rupture of the ovarian cyst and intraabdominal bleeding, torsion of the appendages of the uterus, ectopic pregnancy.
Diagnosis of ovarian hyperstimulation syndrome
Diagnosis of the ovarian hyperstimulation syndrome is established on the basis of data from anamnesis, a comprehensive clinical laboratory and instrumental examination that reveals an increase in ovaries with multiple cysts, marked hemoconcentration and hypercoagulation in the patient who used in this cycle methods of assisted reproductive technology or controlled induction of ovulation to achieve pregnancy.
Laboratory research
Clinical blood test
Hematocrit more than 40%, hemoglobin concentration more than 140 g / l, leukocytosis up to 50x10 9 / l without shift to the left, thrombocytosis up to 500-600x10 6 / l. Hemoconcentration (hematocrit more than 55%) indicates a potential threat to life.
Blood chemistry
Violation of the electrolyte balance, including hyperkalemia (more than 5.3 mmol / l) and hyponatremia (more than 135 mmol / l), leading to a decrease in plasma osmolality. Hypoproteinemia (total protein more than 66 g / l), hypoalbuminemia (albumin less than 35 g / l), high C-reactive protein level, elevation of hepatic transaminases up to 800 U / l, in some cases increased GGT or alkaline phosphatase, in some patients - an increase in the creatinine concentration of more than 80 μmol / l and urea more than 8.3 mmol / l.
Coagulogram
Increased fibrinogen levels of more than 400 mg / dL, von Willebrand factor more than 140%, lower antithrombin III concentrations less than 80%, D-dimer more than 0.5 μg / ml. Normal indicators of APTT, PTI, INR.
[24]
Immunoglobulins of blood
Reduction of the concentration in blood plasma IgG and IgA The analysis of urine is general. Proteinuria.
Analysis of ascites fluid composition
High protein content (more than 42 g / l) and albumin (more than 23 g / l), low white blood cell count, relatively high number of red blood cells, high concentrations of all pro-inflammatory cytokines, C-reactive protein up to 135 mg / l (normal 0-8 , 2 mg / l), the globulin fraction of proteins.
[25], [26], [27], [28], [29], [30], [31]
Oncoproteins in the blood plasma
The concentration of CA-125, reflecting the massive proliferation of ovarian tissue, reaches its maximum values (up to 5125 U / ml) by the second week of development of OHSS, when both ovaries are most enlarged. Elevated levels of the oncomarker persist until 15-23 weeks after the appearance of symptoms of ovarian hyperstimulation syndrome, despite ongoing treatment.
Procalcitonin in serum is determined in 50% of patients in the range of 0.5-2.0 ng / ml, which is regarded as a systemic inflammatory reaction of moderate degree.
Microbiological examination
In the study of urine, separated from the vagina, the cervical canal is isolated atypical pathogens Pseudomonas, Proteus, Klebsiella, Enterobacter, E coli in the amount of more than 10 000 cfu / ml.
Instrumental research
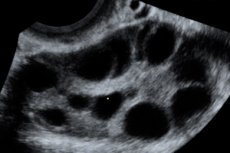
Ultrasound of the pelvic organs
Enlargement of ovaries from 6 to 25 cm in diameter with multiple cysts, uterus of normal size or enlarged, presence of free fluid in the pelvic cavity and normal progressive singleton or multiple pregnancy.
Ultrasound of the abdominal cavity organs
The presence in the abdominal cavity of a free liquid in an amount of 1 to 5-6 liters. Normal size and structure of the liver or hepatomegaly Echoes of dyskinesia of the biliary tract. When studying the kidneys, the cup-and-pelvis complex is not changed.
Ultrasound of the pleural cavities
Presence of free fluid echocardiography. Against the background of hemodynamic disturbances, the decrease in EF, the decrease in the end diastolic volume, the decrease in venous return, in some cases - the presence of free fluid in the pericardial cavity.
ECG
Violation of the rhythm according to the type of ventricular extrasystole, tachycardia, diffuse changes in the myocardium of metabolic and electrolyte character. Radiography of the chest. Conducted with suspicion of ARDS and thromboembolism. A characteristic X-ray finding in ARDS is the appearance of a picture of "frosted glass" and diffuse multifocal infiltrates of rather high density (consolidation) with well-defined air bronchi, the development of extensive lesions of the lung parenchyma. With PE, a high stance of the dome of the diaphragm, discoid atelectasis, fullness of one of the roots of the lungs or a "chopped off" root, a depletion of the pulmonary pattern above the ischemic lung zone, a peripheral triangular shadow of inflammation are detected on the X-ray.
Indications for consultation of other specialists
Due to the involvement of all organs and systems in the pathological process, the therapist must be examined. If there is a suspicion of thrombotic complications, consult a vascular surgeon. In the presence of pronounced hydrothorax - consultation of the thoracic surgeon for solving the problem of performing a puncture of the pleural cavity.
What do need to examine?
How to examine?
What tests are needed?
Treatment of ovarian hyperstimulation syndrome
The absence of a clear conception of the pathophysiology of the OHSS makes it impossible to conduct an effective, pathogenetically substantiated treatment that allows effective and short-term recovery of the syndrome and polyorganic disorders accompanying severe forms of ovarian hyperstimulation syndrome. Currently, there is no specific therapy for ovarian hyperstimulation syndrome, therefore, therapeutic measures for these patients are reduced to pathogenetic therapy until the spontaneous regression of the syndrome as the concentration of CG in the blood plasma decreases within 7 days in cycles where the pregnancy has not occurred, or 10-20 days after the onset of pregnancy. Most patients hospitalized in intensive care units are already diagnosed with CHD after outpatient treatment, consisting of daily weight and diuresis, limiting excessive physical activity and sexual activity, drinking abundantly with the addition of solutions rich in electrolytes, and periodic blood tests. Discussion of the strategy for the treatment of this contingent of patients implies complex symptomatic treatment aimed at preventing the development of MDRs by restoring the cerebral circulation, eliminating hemoconcentration, electrolyte imbalance, prevention of acute renal failure, ARDS, and thromboembolic complications.
1 st stage - assessment of the severity of the condition
The first stage in determining the tactics of managing a patient with ovarian hyperstimulation syndrome is assessment of hemodynamics and respiratory function, and a complete physical examination with a thorough study of the limb, head and neck area to exclude deep vein thrombosis and peripheral venous catheter or catheterization of the central vein, this is the most suitable catheterization of the subclavian vein, since the risk of thrombosis in this case is the smallest. To assess diuresis, a catheterization of the bladder is necessary. Every day it is necessary to investigate the parameters of the clinical blood test, blood plasma electrolytes, protein, liver enzyme activity, creatinine, urea levels, coagulogram indicators of the abdominal ultrasound to determine the extent of ovarian enlargement and ascites.
Stage 2 - infusion therapy
Drug treatment for patients with OHSS should be aimed at maintaining hemodynamics and mobilizing fluid contained in the abdominal cavity by creating a negative balance of sodium and water. The primary task is to recover the volume of circulating fluid to reduce hemoconcentration and maintain sufficient renal filtration. For infusion therapy of the syndrome of ovarian hyperstimulation, crystalloid and colloidal solutions are used.
The choice of crystalloid solution determines electrolyte imbalance. When determining the number of crystalloids administered, it should be taken into account that in the conditions of generalized endothelial damage, the volume of these solutions should be 2-3 times smaller than the volume of colloidal solutions, since the predominance of crystalloids aggravates the accumulation of fluid in the serous cavities, and in some cases leads to the development of anasarca.
The drug of choice for restoration and maintenance of intravascular volume in patients with OHSS - hydroxyethyl starch 130/0 42 daily volume - 25-30 ml / kg. Hydroxyethyl starch 200/0 5 with a volume of 20 ml / (kilogram) can also be used in the basic therapy of CHD. However, it is able to accumulate in the body and with prolonged use can cause liver dysfunction and increase the level of hepatic transaminases sometimes up to 800 U / l. In this contingent of patients it is inappropriate to use hydroxyethyl starch 450/0 7 in connection with a high risk of allergic reactions, a negative effect on kidney function, liver, deterioration of hemocoagulation parameters (prolongation of clotting time, risk of hemorrhagic complications). Indications for the use of solutions of dextrans are limited by the high frequency of allergic reactions, the negative effect on the hemostatic system, the ejection of von Willebrand factor, the induction of the proinflammatory cascade, and the lack of influence on the rheological properties of blood in the doses used. Infusion of dextrans in conditions of increased permeability of capillaries can lead to the development of so-called dextran syndrome, accompanied by OL, impaired liver function, kidneys, development of coagulopathy. Gelatin solutions are also not intended for infusion therapy with CHD.
When hypoproteinemia is less than 25 g / l, 20% albumin solution is used daily volume - 3 ml / kg. It is recommended to use only 20% albumin solution, since the oncotic pressure of the 20% solution is about 100 mm Hg, and the oncotic pressure of the 5% solution is about 20 mm. Gt; Art. In conditions of high permeability of the vascular endothelium, the infusion of 5% albumin solution, in contrast to the 20% solution, leads to more intensive exchange with the extravascular pool and a sharp increase in the oncotic pressure in the interstitium, which leads to an increase in interstitial hyperhydration of the lungs.
Diuretics are justified in oliguria, peripheral edema, reaching hematocrit values of 36-38%. Premature or excessive prescription of diuretics can provoke aggravation of hypovolemia and hemoconcentration, increasing the risk of thrombotic complications. Apply mainly furosemide - 20-40 mg once intramuscularly or intravenously slowly for 1-2 minutes.
Principles of the infusion therapy in the syndrome of ovarian hyperstimulation
After the introduction of the initial dose of crystalloid and colloidal solutions, the volume of further infusion therapy is determined by taking into account the following diuresis - less than 1 ml / (kghh), hematocrit less than - 40%, average blood pressure - more than 70 mmHg, the value of CVP - 8-10 mm. Water. Art. When these parameters are reached, the infusion therapy is stopped. The total daily volume of infusion solutions should be administered fractionally within 24 hours. If these approaches are not followed, hemodilution develops, which provokes a rapid accumulation of fluid in the serous cavities and worsening of the patient's condition. A typical mistake in the treatment of women with hypertension is the unreasonable prolongation of the infusion therapy with the normalization of hemodynamic parameters and an attempt to completely stop the development of the HSH as an iatrogenic condition.
Stage 3 - prevention of complications
Prevention of thrombosis and thromboembolism
The basis for the prevention of thrombotic complications in the syndrome of ovarian hyperstimulation is the elimination of hemoconcentration. Antithrombotic therapy is indicated when laboratory signs of hypercoagulability appear. For this, LMWH is used:
- supraparin calcium (daily dose - 100 anti-Ha IU / kg 2 times subcutaneously),
- dalteparin sodium (100-150 anti-Ha IU / kg 2 times subcutaneously),
- enoxaparin sodium (1 ml Dkgsut) 1-2 times subcutaneously).
Laboratory monitoring - determination of anti-Xa activity of plasma 3 hours after LMWH administration, which allows to maintain an effective dose of the drug within the safe therapeutic range and thus minimize the possibility of bleeding. The appointment of antithrombotic drugs is continued until the coagulation parameters of the blood are normalized. Monitoring is carried out to determine the concentration of D-dimer in plasma by a quantitative method. The duration of administration of LMWH is determined individually, and in some cases it may exceed 30 days.
Prevention of infectious complications
Taking into account the positive effect of the appointment of immunoglobulin preparations in the prevention of secondary infections in other diseases accompanied by loss of protein, one can count on the effectiveness of this therapy in patients with OHSS. However, for the final confirmation or refutation of this hypothesis from the standpoint of evidence-based medicine, it is necessary to conduct studies. At present, the indication for carrying out empirical antibiotic therapy is the risk of secondary infection in patients in a critical condition or in unstable hemodynamics. The change of the empirically selected drug is made according to the results of a bacteriological study. When prescribing empirical antibacterial therapy, it is necessary to be guided by information on the severity of the disease, the risk factors for infection, the characteristics of antibiotic resistance in this ICU.
Nutritional support
Conduct per os to all patients with severe and critical OHSS. It is necessary to follow the recommendations:
- the energy value is 25-35 kcal / (kilohsut),
- glucose - less than 6 g / (kghsut),
- lipids - 0.5-1 g / (kilohsut),
- Proteins - 1,2-2 g / (kilohsut),
- a standard daily set of microelements and vitamins.
4 th stage - surgical methods
Indications for laparocentesis in women with ovarian hyperstimulation syndrome:
- progressive tension ascites,
- oliguria less than 0.5 ml Dkgmmin),
- an increase in the creatinine concentration of more than 80 μmol / l or a decrease in its clearance,
- hemoconcentration with a hematocrit value of more than 40%, not amenable to drug correction.
For laparocentesis, transabdominal or transvaginal access can be selected. The technical complexity is created by enlarged ovaries, in connection with which the use of ultrasound control is extremely important. Long-term drainage of the abdominal cavity (transabdominal laparocentesis) from 14 to 30 days with the peritoneal transudate removed portion by the pyrogenic catheter cystoFix® has a number of advantages, since one-stage evacuation of a large volume of peritoneal transudate can be avoided and thus abrupt fluctuations in intra-abdominal pressure causing hemodynamic disturbances, the patient's condition, avoid repeated punctures of the abdominal cavity to remove ascites in this category of patients. The total volume of evacuated ascites fluid during the period of treatment of severe hypoglycemia may range from 30 to 90 liters.
In patients with hydrothorax in the background of the syndrome of ovarian hyperstimulation, expectant management is justified. When forming the hydrothorax, puncture of the pleural cavity is performed only in the case of pronounced progressive respiratory failure.
Criteria for initiating respiratory support in the syndrome of severe and critical ovarian hyperstimulation:
- lack of independent breathing and abnormal breathing rhythms,
- a reduction in the respiratory index of less than 200 mm Hg,
- life-threatening disorders of the heart rhythm,
- persistent tachycardia more than 120,
- severe hypotension,
- tachypnea more than 40,
- involvement of auxiliary respiratory muscles.
With the development of ARDS and the transfer to artificial ventilation use:
- small respiratory volumes (6 ml / kg),
- inspiratory pressure <30 cm of water,
- PEEP (> 10 cm of water),
- apply the maneuver of recruitment of alveoli.
Surgical treatment in the syndrome of ovarian hyperstimulation is justified only in the presence of acute pathology of torsion of the epididymis, rupture of the ovarian cyst, bleeding from the ovarian cyst. When ovarian torsion is most effective laparoscopic untwisting of the ovary. A typical mistake in the treatment strategy for patients with uncomplicated OHR is an emergency surgery and resection of about 30-50% of ovarian tissue or bilateral ovariectomy.