
Puncture liver biopsy
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

 [
[Indications for a liver biopsy
A puncture biopsy should be used mainly if there is a suspicion of chronic hepatitis or cirrhosis of the liver, in some cases for differential diagnosis of diseases in which the liver is involved in the pathological process (lipoids, fatty hepatoses, glycogenoses, etc.), jaundice and hepatomegaly of unclear etiology .
Indications for liver biopsy are as follows:
- identification of pathology that caused changes in functional liver tests;
- the need to clarify the diagnosis and determine the prognosis for chronic hepatitis;
- confirmation of the presence and prognosis of the course of alcoholic liver disease;
- Diagnosis of systemic diseases, in which the liver is involved in the pathological process;
- assessment of the severity and nature (type) of drug-induced liver damage;
- confirmation of multi-organ infiltrative tumor pathology (lymphoma, leukemia);
- screening of relatives of patients with systemic diseases;
- obtaining tissue for culture;
- diagnosis of Wilson-Konovalov's disease, hemochromatosis, autoimmune hepatitis, chronic viral hepatitis and evaluation of the effectiveness of the therapy;
- Exclusion of graft rejection reaction;
- Exclusion of reinfection or ischemia of the organ after liver transplantation.
To avoid severe consequences caused by parenchymal hemorrhage, it is advisable to perform a puncture biopsy in the conditions of the surgical department. After puncture liver biopsy, the occurrence of bile peritonitis, purulent complications (abscess, phlegmon) and even pneumothorax is described. The development of pleurisy, perihepatitis, formation of intrahepatic hematomas, hemobiology, arteriovenous fistula formation, accidental puncture of the kidney or large intestine, as well as infectious complications occurring as transient bacteremia, rarely - sepsis are described. In general, the complications of biopsy in children are more common than in adults, reaching 4.5%. Mortality with a puncture biopsy is from 0.009 to 0.17%.
How is puncture liver biopsy performed?
There are percutaneous puncture of the liver and aiming, under the control of a laparoscope or ultrasound. Puncture of the liver under the control of a laparoscope or ultrasound is most effective in focal lesions of the liver. With diffuse changes in the tissue of the organ, a blind biopsy can be used, and although the place of obtaining liver tissue can not be determined at this time, a high percentage of positive results is achieved, and ease of execution makes it accessible to any hepatology department.
If there is a clotting disorder, massive ascites, small liver size or lack of contact with the patient, and fulminant liver failure, a transgular liver biopsy is used using a Trucut needle placed in a catheter inserted through the jugular vein into the hepatic vein.
Among the needle puncture systems, the Mengini needle and the Trucut needle (the modification of the Silverman needle) were most widely used. A number of other systems are also used.
A puncture liver biopsy is performed in the patient's position on the back. The skin at the puncture site (usually the ninth and tenth intercostal spaces on the right between the anterior and middle axillary lines) is treated with an antiseptic solution. After that, 2% solution of novocaine is performed by local anesthesia of the skin, subcutaneous fat and liver capsules.
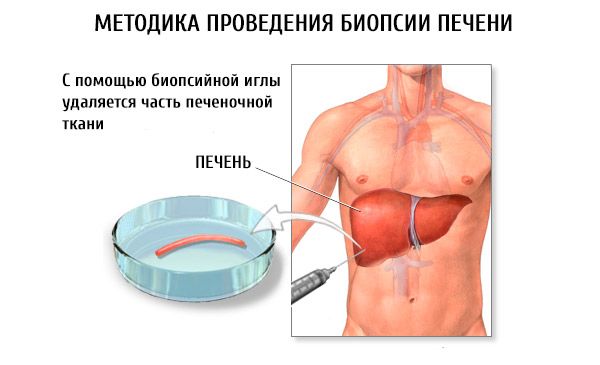
The puncture is made by styling, injecting it to a depth of 2-4 mm. Then, through the stylet, the needle needle of Mengini is inserted (pediatric practice uses a shortened needle) connected to a 10-gram syringe containing 4-6 ml of isotonic sodium chloride solution. The needle is held up to the liver capsule and 2 ml of isotonic sodium chloride solution is released to expel the pieces of adipose tissue from the needle. The needle is injected into the liver parenchyma and pieces of organ tissue are aspirated using a syringe plunger. After the end of the manipulation, a sterile sticker is applied and a bubble with ice is placed in place of the puncture. Within 24 hours the patient keeps bed rest.
It is not advisable to perform a puncture of the liver with congestive jaundice, pustular rash on the skin (especially at the site of the alleged puncture). Do not perform puncture liver biopsy on the background of acute respiratory disease, angina, other acute infections.
According to the tissue column obtained with liver biopsy, it is possible to judge changes in the entire organ, especially in diffuse processes (viral hepatitis, steatosis, reticulosis, cirrhosis, etc.). But biopsy does not always allow to diagnose focal lesions of the liver (granuloma, tumor, abscess, etc.). The reason for the uninformative biopsy may also be the absence in the biopsy of portal tracts and the small dimensions of the tissue sample.
The height of the column of tissue is 1-4 cm and its mass is 10-50 mg. The tissue sample is usually fixed in a 10% formalin solution in an isotonic sodium chloride solution. Preparations are stained with hematoxylin and eosin, the Schick reaction is performed for the presence of connective tissue, etc. In addition, tissue columns derived from paraffin blocks can be retrospectively examined. For adequate interpretation of the results, the tissue sample should be at least 2 cm long and contain four portal tracts.
Contraindications to a liver biopsy
With adequate technique of puncture liver biopsy and strict account of all contraindications, the number of complications during this manipulation is relatively small. The most dangerous of them are: bleeding, development of pleural shock, damage to neighboring organs, infection of the pleural or abdominal cavity. It should be remembered that often after a puncture liver biopsy, patients experience pain at the puncture site, in the epigastric region, the right shoulder and the right supraclavicular area. As a rule, these symptoms are not dangerous and after a while they pass by themselves.
Contraindications to liver biopsy are as follows.
Absolute:
- severe coagulopagia-prothrombin time greater than 3 s or prothrombin index 70% or less;
- the number of platelets in the peripheral blood is 60x10 9 / l and less;
- increased bleeding time;
- anticipated liver echinococcosis;
- anticipated liver hemangioma;
- patient's refusal to perform this manipulation.
Relative:
- marked ascites;
- right-sided pleurisy;
- cholangitis;
- biliary obstruction of any etiology.