Medical expert of the article

New publications
Uroflowmetry
Last reviewed: 07.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Uroflowmetry is a noninvasive screening test to detect possible lower urinary tract dysfunction. It measures urine flow parameters.
The function of the lower urinary tract is to accumulate and evacuate urine. The bladder passively accumulates urine, then the act of urination occurs, associated with a reflex relaxation of the sphincter and contraction of the detrusor (urination is the main event of the corresponding reflex).
Indications for the procedure
Today, uroflowmetry is actively used in a wide range of urological diseases:
- prostate adenoma,
- prostate cancer,
- chronic prostatitis,
- urethral stricture in men,
- chronic cystitis and symptoms of urinary dysfunction in women,
- vesicoureteral reflux,
- lower urinary tract infections,
- enuresis in children,
- neurogenic dysfunction of micturition (NMD),
- urinary incontinence in all categories of patients.
Methodology for conducting uroflowmetry
The principle of uroflowmetry is to record the volumetric speed of urine flow during urination. To measure urination parameters, weight sensors are most often used, less often - rotary or electronic sensors. The sensor is installed on a stable platform. The device is also equipped with an electronic recording device with a microprocessor. The latest models of uroflowmeters can transmit data to a personal or pocket computer via wireless WiFi or BlueTooth channels. The device must be calibrated periodically (usually using a special device).
The patient comes for the examination with an average bladder filling, which corresponds to a normal urge to urinate of moderate intensity (urine volume 150-500 ml). The patient is first explained the meaning and method of the examination. Urination should be as natural and free as possible, without any additional effort. Men are asked to urinate standing up, women - sitting (for which a special chair is installed above the device). After the examination is completed, the volume of residual urine is determined by ultrasound scanning or catheterization. The most convenient way to measure residual urine is with a special portable standardized ultrasound device.

Decoding the results
The following parameters are used to interpret the study:
- maximum urination rate - Qmax (ml/s);
- average urination rate - Qcp (ml/s);
- time to reach maximum speed (s);
- urination time (s);
- flow time (s):
- volume of urine excreted or volume of urination (ml);
- residual urine volume (ml).
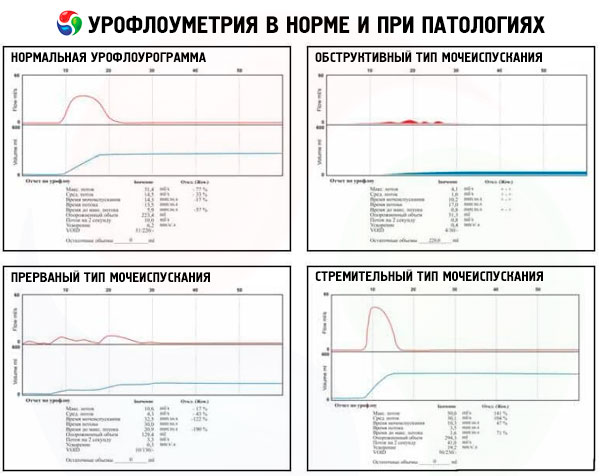
An important stage in assessing the results of the study is the analysis of the urine output graph (urination curve) and digital information. The normal curve has a bell shape. In case of urethral stricture, the curve is in the form of a "plateau". The uroflowmetric curve in case of obstruction or weakness of the detrusor is characterized by a decrease in the maximum flow rate of urination. A curve with a rapid rise to Qmax, less than 1 s from the start of urination ("rapid urination") is typical of overactive bladder (OAB). It is characteristic that in single-phase urination, the urination time is equal to the urine flow time, and in case of urination in several stages, the urination time is longer than the urine flow time.
The main digital uroflowmetric indicator is Qmax. Qmax values exceeding 15 ml/s are usually considered normal. Uroflowmetry is assessed with a urine volume of 150 to 450 ml. In adults, with volumes less than 150 ml and more than 500 ml, the results of the study are uninformative.
The lower limit of the norm for the maximum urine flow rate depending on age and gender (according to Abrams P., 2003)
Age, years |
Minimum urine output, ml |
Men, ml/s |
Women, ml/s |
4-7 |
100 |
10 |
10 |
8-13 |
100 |
12 |
15 |
14-45 |
200 |
18 |
21 |
46-65 |
200 |
12 |
15 |
66-80 |
200 |
9 |
10 |
It has been established that the maximum urine flow rate depends on the patient's gender, age, volume of urination and conditions of the study. As early as 1984, Abrams demonstrated the existence of a nonlinear relationship between the excreted urine volume and Q.
There are additional factors that affect the rate of urination: abdominal pressure and physiological delay due to patient anxiety and discomfort caused by the need to urinate among testing equipment in the presence of medical personnel. In this situation, voluntary abdominal tension to facilitate urination provokes the appearance of abnormally high Q max surges against the background of a characteristic intermittent curve. In this regard, to obtain more reliable data, uroflowmetry is recommended to be performed at least twice under conditions of functional filling of the bladder (for adults 150-350 ml) when a natural urge to urinate occurs. In a number of clinical observations, uroflowmetric monitoring over a longer period of time can be recommended to obtain a clear picture.
One of the most common clinical problems in which uroflowmetry is used is the diagnosis of infravesical obstruction (IVO) in elderly men. The works of Abrams and Grifith showed the dependence of the presence of infravesical obstruction on the Q max index.
It should be noted that the specificity of uroflowmetry for determining infravesical obstruction is low (especially at Qmax values within 10-15 ml/s), since in some elderly men, symptoms of impaired urination may be due to detrusor weakness or neurogenic dysfunction.
To compare the results of uroflowmetry conducted at different times with different volumes of urination or in patients of different ages, special nomograms are used. The most common of them are: Siroki (1979) - for men, Liverpool (1989) - for men and women. At present, modified nomograms adapted by gender and for each age group are proposed.
To increase the information content, uroflowmetry assessment should be carried out not only by the Qmax value, but also taking into account all the indicators. As a result of uroflowmetry, a conclusion is made about what type of urination is observed in a given patient:
- obstructive;
- non-obstructive;
- ambiguous;
- "swift";
- intermittent.
Despite the fact that uroflowmetry is only a screening test, the method provides the specialist with extremely important objective information about the nature of urination disorders, allowing in a number of observations to carry out differential diagnostics of various conditions and to identify groups of patients for further urodynamic studies. In other words, uroflowmetry is an objective indicator of urination disorders, often determining the further diagnostic path. At present, uroflowmetry has become a mandatory examination method in the protocols for the management of the vast majority of lower urinary tract diseases in adults and children. That is why the presence of uroflowmetric equipment is necessary in all offices and departments with urological reception.
 [
[ What do need to examine?
What tests are needed?