Medical expert of the article

New publications
Proptosis: Causes, Diagnosis, Treatment, and Prognosis in Children and Adults
Last updated: 04.04.2026

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
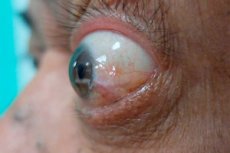
Proptosis is an anterior displacement of the eyeball, causing the eye to appear bulging. In clinical practice, it is not a disease in itself, but an important symptom that may indicate inflammation, infection, vascular anomaly, hemorrhage, endocrine orbitopathy, or orbital tumor. Therefore, proptosis always requires not only a description of the external sign but also a search for its cause. [1]
The terms "proptosis" and "exophthalmos" are often used interchangeably. However, in a more strict sense, exophthalmos is more often associated with thyroid eye disease, while proptosis is associated with any anterior displacement of the eye, regardless of cause. For the physician, the clinical context is more important than the word itself: whether the process is unilateral or bilateral, the rate of development, the presence of pain, fever, double vision, decreased vision, and pulsation. [2]
In adults, the most common cause of bilateral proptosis is thyroid eye disease associated with Graves' disease. In children, the most common cause of proptosis is orbital cellulitis, an infection of the orbital tissue behind the orbital septum. This distinction is important because sudden proptosis in a child is often interpreted as a potentially dangerous infection, while in adults, it is a reason to primarily rule out endocrine orbitopathy, while also considering tumors and vascular causes. [3]
From a practical standpoint, proptosis poses a danger beyond its cosmetic defect. It can lead to incomplete closure of the eyelids, corneal dryness and ulceration, limited eye movement, double vision, increased intraocular pressure, and, in severe cases, optic nerve compression with irreversible vision loss. In some cases, such as orbital compartment syndrome, the consequences can be measured in minutes or hours. [4]
A separate problem is pseudoproptosis, when the eye appears to bulge, but there is no true anterior displacement. This can occur with severe eyelid retraction, severe hyperthyroidism without orbital infiltrative lesions, severe obesity, and also with an enlarged eyeball, such as in congenital glaucoma. Therefore, the external impression must be confirmed by objective measurement and visualization. [5]
| Key fact | Why is this important? |
|---|---|
| Proptosis is a symptom, not a definitive diagnosis [6] | Treatment is chosen based on the cause, not just on external signs. |
| In adults, a common cause is thyroid eye disease [7] | Thyroid function assessment and orbital imaging are needed. |
| In children, a common cause is orbital cellulitis [8] | Urgent evaluation for infection and vision threat is required. |
| Acute proptosis can be an emergency condition [9] | Examination and treatment cannot be postponed. |
Code according to ICD-10 and ICD-11
In the International Classification of Diseases, Tenth Edition, proptosis is classified under section H05.2—Exophthalmic conditions. For clinical detail, a number of systems additionally use subcategories, such as for unspecified exophthalmos, constant, intermittent, or pulsating exophthalmos. This emphasizes that coding here is often based not only on the symptom but also on its clinical form. [10]
The International Classification of Diseases, Eleventh Edition, uses code 9A20.00—anterior displacement of the eyeball—which explicitly includes proptosis and exophthalmos. This edition allows for postcoordination, meaning the ability to add clarifying elements, such as lateralization. This is convenient in practice, as the same symptom can be unilateral, bilateral, constant, or associated with a specific cause, which also requires separate coding. [11]
| Classification | Code | What does it mean? |
|---|---|---|
| ICD-10 | H05.2 [12] | Exophthalmic conditions |
| ICD-10, clinical detailing | H05.20 [13] | Unspecified exophthalmos |
| ICD-11 | 9A20.00 [14] | Anterior displacement of the eyeball, including proptosis and exophthalmos |
| ICD-11 | Post-coordination [15] | It is possible to clarify the side and clinical context |
Epidemiology
Proptosis itself, as a symptom, has no unified global epidemiological statistics because it occurs in a wide variety of diseases. Therefore, in real-world clinical practice, the epidemiology is assessed based on the underlying causes. The most significant contributors in adults are thyroid eye disease, and in children, orbital cellulitis and certain tumors. [16]
Thyroid eye disease develops in approximately 25%–50% of patients with Graves' disease. Modern reviews also estimate an overall incidence of thyroid eye disease of approximately 155 per 100,000 population and an average annual incidence of approximately 5 per 100,000 person-years, although figures vary between countries and depend on the database used.[17]
According to large reviews, the disease is more common in women, especially in middle age, but severe forms are more often observed in older patients. The risk of vision-threatening progression is low, but not zero: severe enlargement of the orbital contents with the risk of optic nerve compression or severe exposure keratopathy is described in approximately 2%-8% of patients with thyroid eye disease. [18]
Childhood is characterized by a different pattern of causes. Infectious processes, primarily orbital cellulitis, occupy a prominent place. Furthermore, depending on age, the differential diagnosis includes dermoid cysts, rhabdomyosarcoma, metastatic neuroblastoma, leukemic infiltrates, and vascular malformations. [19]
The rate of symptom development is also important epidemiologically. Acute unilateral proptosis is more often associated with infection, hemorrhage, or vascular accident, whereas slowly progressing chronic unilateral proptosis is more suggestive of a tumor. This is not an absolute rule, but it is a useful clinical guideline even at the initial examination. [20]
| Epidemiological landmark | What is known |
|---|---|
| In adults, the leading cause of proptosis is | Thyroid eye disease [21] |
| In children, the leading cause of proptosis is | Orbital cellulite [22] |
| The prevalence of thyroid eye disease among Graves' disease | About 25%-50% [23] |
| Estimated annual incidence of thyroid eye disease | About 5 per 100,000 person-years [24] |
| Severe forms with threat to vision | Approximately 2%-8% [25] |
Reasons
The causes of proptosis are conveniently divided into inflammatory, infectious, endocrine, vascular, traumatic, and neoplastic. This approach is important because the same external symptom may require urgent antibiotics, immediate decompression, anti-inflammatory therapy, surgery, or oncological treatment. [26]
In adults, the main cause of bilateral proptosis remains thyroid eye disease. It involves enlargement of the extraocular muscles, orbital fat, and connective tissue, causing the orbital contents to literally "not fit" within the bony orbit and pushing the eye forward. This same cause can also produce an asymmetrical picture, although bilateral involvement is more typical. [27]
Infectious causes are particularly important due to the risk of rapid deterioration. Orbital cellulitis usually occurs with the spread of infection from the paranasal sinuses, most often the ethmoid labyrinth, but odontogenic spread, trauma, bites, foreign bodies, and hematogenous spread are also possible. Patients with diabetes mellitus and immunodeficiency are most vulnerable to fungal orbital infections. [28]
Vascular causes include carotid-cavernous fistula, cavernous sinus thrombosis, and orbital compartment syndrome secondary to retrobulbar hemorrhage. Clues include ocular pulsation, orbital bruit, severe pain, rapid worsening of symptoms, decreased vision, and ophthalmoplegia. These conditions are among the most dangerous. [29]
Neoplastic causes depend on age. In children, rhabdomyosarcoma, metastatic neuroblastoma, and leukemic infiltrates should be considered. In adults, orbital lymphoma, meningioma, mucocele, cavernous venous malformations, lacrimal gland tumors, and secondary tumor spread from the paranasal sinuses and intracranial structures are more common. In tumors, the diagnosis is suspected based on examination and neuroimaging, but confirmation often requires biopsy. [30]
Pseudoproptosis and conditions that mimic true ocular protrusion are separate. These include eyelid retraction in thyrotoxicosis without orbital infiltrative disease, severe obesity, Cushing's syndrome, and enlargement of the eyeball itself, such as in congenital glaucoma. Overlooking this point can lead to misjudgment of the severity of the condition and unnecessary treatment. [31]
| Group of reasons | Examples |
|---|---|
| Endocrine | Thyroid eye disease [32] |
| Infectious | Orbital cellulitis, fungal orbital infection [33] |
| Vascular and emergency | Carotid-cavernous fistula, cavernous sinus thrombosis, orbital compartment syndrome [34] |
| Tumor | Lymphoma, meningioma, mucocele, tumors of the lacrimal gland, rhabdomyosarcoma [35] |
| False proptosis | Eyelid retraction, obesity, congenital glaucoma [36] |
Risk factors
Risk factors vary depending on the cause, but for thyroid eye disease, the best-studied factors are smoking, thyroid dysfunction, high levels of thyroid-stimulating hormone receptor antibodies, and radioactive iodine therapy in some patients. Smoking is considered one of the most important modifiable factors: it is associated with a more severe course and a poorer response to treatment. [37]
The risk of severe progression is higher in patients with uncompensated thyroid status. Maintaining euthyroidism is considered one of the basic principles for preventing orbitopathy progression. This is especially important in patients who already have eyelid retraction, dry eyes, diplopia, or mild proptosis. [38]
Risk factors for orbital cellulitis include sinusitis, dental infections, eyelid and orbital trauma, bites, foreign bodies, and conditions that weaken the immune response. Patients with diabetes and immunodeficiency are more likely to develop a severe and complicated course of the disease, including invasive fungal infections. [39]
For orbital compartment syndrome, the risk increases after facial trauma, surgery, retrobulbar injections, massive hemorrhage, and some rare causes of increased orbital pressure. For tumoral proptosis, the main risk factor is not a single external trigger, but the age profile of the disease and a history of malignancy. Therefore, when collecting complaints, questions about previous cancer, thyroid disease, recent trauma, and sinus infections are always important. [40]
| Risk factor | What is the reason for this? |
|---|---|
| Smoking | More severe thyroid eye disease and poorer response to treatment [41] |
| Thyroid dysfunction | Development and progression of thyroid eye disease [42] |
| Radioactive iodine in some patients | May increase the risk of worsening orbitopathy [43] |
| Sinusitis, trauma, bites, foreign bodies | Orbital cellulite [44] |
| Trauma and retrobulbar hemorrhage | Orbital compartment syndrome [45] |
Pathogenesis
The pathogenesis of proptosis generally boils down to a single mechanical principle: within the limited space of the bony orbit, the amount of tissue, fluid, blood, or inflammatory infiltrate increases. Since the orbit is virtually incapable of expansion, the excess volume displaces the eyeball anteriorly. This is why the same clinical sign can occur with inflammation, tumor, and hemorrhage. [46]
In thyroid eye disease, autoimmune inflammation, activation of orbital fibroblasts, accumulation of glycosaminoglycans, edema, and orbital tissue remodeling play a leading role. Fibroblasts are activated through thyroid-stimulating hormone and insulin-like growth factor receptors, followed by increased cytokine inflammation, adipogenesis, and fibrosis. As a result, extraocular muscles and orbital adipose tissue enlarge. [47]
In orbital cellulitis, proptosis is caused by tissue swelling, inflammatory exudate, sometimes a subperiosteal abscess, and increasing intraorbital pressure. If the process progresses, eye movement, venous outflow, and perfusion of the optic nerve and retina are impaired. This is how infectious inflammation can quickly progress from a localized problem to a threat to vision and even life. [48]
In tumors, the mechanism is usually slower. The mass gradually occupies space in the orbit, displacing the eye in the direction opposite the lesion, or causing axial proptosis if located deep behind the eyeball within the conus muscularis. The direction of displacement provides an important clue about the localization of the process even before tomography. [49]
In orbital compartment syndrome, the mechanism is most dramatic: a sharp increase in orbital pressure leads to decreased perfusion of the optic nerve and retina. Ischemia can quickly become irreversible, so imaging should not delay decompression. This pathogenetic principle explains why, if this condition is suspected, lateral canthotomy and cantholysis are performed immediately. [50]
| Mechanism | Result |
|---|---|
| Increasing tissue volume in a closed orbit | Anterior displacement of the eye [51] |
| Autoimmune inflammation of orbital fibroblasts | Edema, adipogenesis, fibrosis, thyroid proptosis [52] |
| Infection and abscess formation | Rapid increase in pressure, pain, deterioration of vision [53] |
| Tumor growth | Slow displacement of the eye, sometimes with a change in direction [54] |
| A sharp increase in pressure in the orbit | Ischemia of the optic nerve and retina [55] |
Symptoms
The main symptom is a sensation or visible bulging of the eye. Sometimes, it is not the patient themselves who first notices it, but relatives or a doctor, based on facial asymmetry. If the process is unilateral, the difference is usually more noticeable; with a bilateral, slow-onset variant, the patient may perceive the change for a long time as a "tired" or "wide-open" look. [56]
Proptosis is often accompanied by dryness, lacrimation, irritation, photophobia, and a foreign body sensation. These symptoms arise from incomplete closure of the eyelids and a larger area of the cornea exposed to air. If the ocular surface is poorly protected, epithelial defects and the risk of corneal ulceration develop. [57]
Another important set of symptoms is associated with impaired ocular motility: double vision, pain with movement, and limited upward, downward, or sideward gaze. Pain and tenderness with eye movements are particularly characteristic of infectious processes, while thyroid eye disease is characterized by progressive limited movement and diplopia against a background of muscle enlargement. [58]
Particularly worrisome signs include decreased vision, changes in color perception, field symptoms, severe headache, fever, ocular pulsation, and ophthalmoplegia. These findings suggest optic nerve compression, cavernous sinus thrombosis, carotid-cavernous fistula, severe orbital infection, or compartment syndrome.[59]
The rate of development is also part of the symptom complex. Sudden or very rapid proptosis is more characteristic of hemorrhage, infection, and vascular causes. Slow progression over weeks and months is more consistent with a tumor or chronic inflammatory process. [60]
| Symptom | What could it mean? |
|---|---|
| Bulging eye | True proptosis, requiring measurement and search for the cause [61] |
| Dryness, photophobia, irritation | Corneal exposure due to incomplete closure of the eyelids [62] |
| Double vision and limited movement | Lesions of the extraocular muscles or growth of volume in the orbit [63] |
| Pain, fever, redness | Infection or acute inflammation [64] |
| Pulsation, noise, sudden decrease in vision | Vascular pathology or compartment syndrome [65] |
Classification, forms and stages
There is no universal stage for proptosis as a symptom, as stages depend on the cause. In clinical practice, proptosis is typically described using several parameters: unilateral or bilateral, acute or chronic, axial or non-axial, constant, intermittent, or pulsatile. This description format is much more useful than attempting to mechanically assign a general stage. [66]
Axial proptosis refers to a strictly anterior displacement of the eye and is more common with processes located deep behind the eye within the muscular cone. Non-axial proptosis indicates a superior, inferior, medial, or lateral displacement and helps to identify which part of the orbit or adjacent anatomical zone the process is originating from. [67]
Based on the time of development, it is useful to distinguish between acute, subacute, and chronic proptosis. The acute form is characteristic of orbital hemorrhage, compartment syndrome, orbital cellulitis, and some vascular accidents. The chronic form is more common in tumors and endocrine orbitopathy. [68]
If the cause is thyroid eye disease, then it's appropriate to talk about an active inflammatory phase and an inactive fibrotic phase. This is crucial because anti-inflammatory and targeted therapies are more effective during the active phase, while rehabilitation surgery, strabismus correction, and eyelid surgery are more effective during the inactive phase. [69]
| Classification feature | Options |
|---|---|
| On the side | One-sided, two-sided [70] |
| In the direction | Axial, non-axial [71] |
| By tempo | Acute, subacute, chronic [72] |
| By character | Constant, intermittent, pulsating [73] |
| For thyroid eye disease | Active phase and inactive fibrotic phase [74] |
Complications and consequences
The most common local complication is damage to the ocular surface. When the eyelids do not close completely, the cornea dries out, loses its protection, and becomes vulnerable to erosions, infections, and ulcers. In severe cases, this is no longer just discomfort, but a path to permanent vision loss. [75]
The second major set of complications is associated with limited eye movement and diplopia. Even if vision is preserved, persistent double vision can dramatically reduce quality of life, limiting reading, driving, and work. For patients with thyroid eye disease, cosmetic changes and diplopia often become the main cause of chronic psychological distress. [76]
The most dangerous complication is optic nerve compression with vision loss. This is rare in thyroid eye disease but requires urgent treatment. In the presence of orbital compartment syndrome, severe infection, or cavernous sinus thrombosis, the threat to vision and life can mount very quickly. [77]
Infectious proptosis poses a risk not only to the eye. Orbital cellulitis can be complicated by cavernous sinus thrombosis, meningitis, brain abscess, central retinal artery or vein thrombosis, and optic neuropathy. Therefore, such patients require prompt imaging, hospitalization, and observation. [78]
| Complication | What is dangerous? |
|---|---|
| Exposure keratopathy | Erosions, corneal ulcers, decreased vision [79] |
| Restricted eye movements | Diplopia and persistent functional impairment [80] |
| Optic nerve compression | Irreversible vision loss [81] |
| Intracranial complications of infection | Meningitis, brain abscess, cavernous sinus thrombosis [82] |
When to see a doctor
Any new proptosis, even if it seems "minor" and is painless, should be seen by a doctor. True proptosis is rarely a harmless finding, and visual impressions often underestimate the severity of the cause. The earlier measurement and imaging are performed, the lower the risk of missing a tumor, infection, or optic nerve compression. [83]
Urgent treatment is required if proptosis develops rapidly, especially on one side. This scenario requires excluding orbital cellulitis, retrobulbar hemorrhage, carotid-cavernous fistula, cavernous sinus thrombosis, and compartment syndrome. In these situations, waiting for a scheduled appointment is dangerous. [84]
Urgent signs include eye pain or redness, headache, decreased vision, double vision, fever, a pulsating bulge, and proptosis in a newborn. This is a list of warning signs that require urgent examination. [85]
In patients with Graves' disease, new changes in the appearance of the eyes, a feeling of pressure behind the eye, dryness, double vision, decreased vision, and an inability to fully close the eyelids are reasons for an urgent visit. Even if thyroid indicators are already being treated, orbitopathy may require a separate ophthalmological approach. [86]
| Situation | Urgency |
|---|---|
| Any new-onset proptosis | In-person examination is mandatory [87] |
| Rapid unilateral proptosis | Urgently, often on the day of symptom onset [88] |
| Pain, redness, fever, decreased vision | Emergency care [89] |
| Eye pulsation or noise | Emergency exclusion of vascular pathology [90] |
Diagnostics
Diagnosis begins with three questions: is it true proptosis or pseudoproptosis, how quickly it developed, and whether there is an immediate threat to vision. At this stage, the doctor already evaluates the affected side, pain, temperature, diplopia, visual acuity, color perception, pupillary response, eye movement, and corneal condition. A history of recent trauma, sinusitis, thyroid disease, or cancer can immediately narrow the search for the cause. [91]
The next step is objective measurement. This is done using exophthalmometry, most commonly by Hertel. Normal values vary by age, gender, and ethnic group in different sources, but a protrusion of approximately 12-21 millimeters is generally considered normal, while a difference between the eyes of more than 2 millimeters is considered abnormal. Some manuals also specify a more conservative guideline of "usually less than 20 millimeters," further emphasizing the importance of comparison with the opposite eye and the specific type of instrument. [92]
The laboratory examination is determined by the suspected cause. If the doctor suspects thyroid eye disease, thyroid-stimulating hormone, free thyroid hormones, and thyroid-stimulating hormone receptor antibodies become key, as this autoimmune pathway is associated with the severity of the disease. If an infectious process is suspected, a complete blood count, blood cultures, and, as appropriate, other inflammatory markers are typically added to the inpatient evaluation. [93]
Imaging is almost always necessary unless the cause is obvious. Computed tomography and magnetic resonance imaging of the orbits help confirm proptosis itself and evaluate muscles, fat, optic nerve, sinuses, and the presence of abscesses, tumors, hemorrhages, or bony changes. If pulsatile proptosis and vascular anomalies are suspected, magnetic resonance angiography or other vascular imaging may be necessary. [94]
There are also important clinical patterns. In orbital cellulitis, proptosis, pain with eye movement, limited mobility, redness, chemosis, and decreased vision are alarming; CT imaging often reveals orbital tissue inflammation, sinus changes, and sometimes a subperiosteal abscess. In tumors, the diagnosis is often advanced by a combination of a slow progression, neuroimaging data, and, if necessary, biopsy. [95]
Diagnosis of emergency conditions is a separate issue. If orbital compartment syndrome is suspected, clinical diagnosis and decompression are more important than waiting for imaging, as delay can cost vision. If compressive dysthyroid optic neuropathy is suspected, urgent treatment and very careful monitoring of visual function are required. [96]
| Diagnostic step | What are they looking for? |
|---|---|
| Examination and anamnesis | Rate of progression, pain, diplopia, decreased vision, thyroid and infectious history [97] |
| Exophthalmometry | Confirmation of true proptosis and asymmetry greater than 2 millimeters [98] |
| Tests | Thyroid hormones, antibodies, in case of infection - general clinical and bacteriological tests [99] |
| Computer and magnetic resonance imaging | Muscle, fat, abscess, tumor, hemorrhage, sinuses [100] |
| Vascular studies | In case of pulsating proptosis and suspected fistula [101] |
| Biopsy | Confirmation of some tumor and atypical inflammatory processes [102] |
Differential diagnosis
The first differential diagnosis is true proptosis or pseudoproptosis. True proptosis is confirmed by measurement and visualization. Pseudoproptosis is possible with eyelid retraction, a large eyeball, severe obesity, and certain endocrine conditions without actual increase in orbital tissue volume. An error at this stage can lead to either overdiagnosis or missed orbital pathology. [103]
The second key differential diagnosis is orbital and preorbital cellulitis. Preorbital inflammation is characterized by swelling and redness of the eyelid with normal eye position, preserved vision, and normal mobility. Orbital cellulitis, on the other hand, is characterized by proptosis, painful eye movements, limited mobility, decreased visual acuity, and a higher risk of intracranial complications. [104]
The third block is thyroid eye disease versus orbital tumor. Thyroid orbitopathy is more characterized by bilaterality, eyelid retraction, dryness, diplopia, and a combination with thyroid dysfunction. Tumors are more often characterized by slow progression, sometimes unilaterality, ocular displacement in a certain direction, and confirmation by tomography and then biopsy. [105]
The fourth block is vascular causes. Pulsatile proptosis with orbital bruit particularly suggests carotid-cavernous fistula. Ophthalmoplegia, headache, ptosis, fever, and visual impairment require the exclusion of cavernous sinus thrombosis. Rapid, painful bulging after trauma or surgery primarily suggests retrobulbar hemorrhage and compartment syndrome. [106]
Finally, the differential diagnosis in children differs from that in adults. In early childhood, dermoid, vascular lesions, rhabdomyosarcoma, neuroblastoma, and leukemia are important. Therefore, in a child, even without severe pain and fever, unilateral or bilateral proptosis cannot be interpreted as simple eyelid swelling. [107]
| It is necessary to distinguish | Distinguishing features |
|---|---|
| True proptosis and pseudoproptosis | Measurement, visualization, absence of real displacement in facial expressions [108] |
| Preorbital and orbital cellulitis | With orbital there is proptosis, pain during movement, limited mobility, and possible decreased vision [109] |
| Thyroid orbitopathy and tumor | Thyroid background and bilaterality versus slow local growth and need for biopsy [110] |
| Vascular pathology and inflammation | Pulsation, noise, acute course, severe neurological symptoms [111] |
| Childhood tumors and infections | Age profile and tomography data decide a lot [112] |
Treatment
Treatment of proptosis is always cause-based. There is no universal "pill for eye bulging." The doctor's first decision is to determine whether there is a threat to the cornea, optic nerve, or the patient's life. If there are signs of an emergency, treatment begins in parallel with further examination, rather than after a full search has been completed. [113]
Almost any cause requires measures to protect the ocular surface. Moisturizers, nighttime protective masks, or mechanical corneal protection are used, while in cases of severe lagophalmos, more aggressive methods of covering the ocular surface are used. This is especially important when the protrusion itself has not yet resolved and the cornea is already suffering. [114]
For mild active thyroid eye disease, the mainstays are local measures, observation, smoking cessation, and maintaining normal thyroid function. For some patients in areas with insufficient selenium intake, a course of selenite (100 micrograms) twice daily for 6 months may be considered. Clinical guidelines emphasize that this strategy is appropriate for mild active disease, not for severe proptosis that threatens vision. [115]
If thyroid eye disease is characterized by predominantly inflammatory activity without significant proptosis or pronounced diplopia, intravenous glucocorticosteroid therapy is considered the preferred option. The American Thyroid Association and European Thyroid Association consensus describes the standard regimen as a total dose of 4.5 grams of intravenous methylprednisolone over approximately 3 months. An important limitation is that a total dose greater than 8 grams is avoided due to toxicity. [116]
For active, moderate to severe thyroid eye disease with significant proptosis and/or diplopia, if the drug is available, teprotumumab is considered the preferred current option. In randomized trials, patients receiving this drug achieved a reduction in proptosis of at least 2 millimeters significantly more often than those receiving placebo, and in the OPTIC study, such a response was observed in 83% versus 10% of the comparison group. A pooled analysis showed improvements not only in proptosis but also in diplopia and quality of life. [117]
However, teprotumumab cannot be considered a foolproof solution. The consensus document notes worsening glucose control, muscle spasms, nausea, hair loss, and hearing impairment, and more recent reviews further confirm the drug's association with otologic side effects. Therefore, before initiating treatment, the benefits, cost, availability, and risk profile should be discussed, particularly in patients with diabetes and preexisting hearing problems. [118]
Mycophenolate, rituximab, and tocilizumab are considered as other systemic options for active moderate to severe thyroid eye disease. According to the consensus document, mycophenolate has improved composite outcomes and some activity measures in several studies, while rituximab and tocilizumab may be considered in patients with glucocorticosteroid resistance. It is important to understand that the effect of these drugs is better documented for inflammatory activity than for gross mechanical protrusion of the eye. [119]
Orbital radiation therapy has been used for decades. It is not a universal treatment for all proptosis, but it can reduce periorbital inflammation and improve ocular motility in active thyroid orbitopathy. It is most appropriate to consider it as part of a combination strategy in carefully selected patients, rather than as a treatment for late, inactive fibrotic stage. [120]
Surgical treatment plays a different role for different causes. For tumors, its goal is removal or biopsy of the lesion, sometimes followed by radiation or drug oncotherapy. In thyroid eye disease, orbital decompression is used to reduce proptosis, treat exposure keratopathy, and, most importantly, in dysthyroid optic neuropathy, when it is necessary to relieve the orbital apex and relieve pressure on the optic nerve. This typically involves decompression of the deep medial wall and orbital floor, while other combined approaches are possible in cases of severe cosmetic or mechanical proptosis. [121]
In thyroid dysthyroid optic neuropathy, treatment is urgent. The patient requires immediate treatment with intravenous glucocorticosteroids and close vision monitoring. If the response is incomplete or temporary, surgical decompression should be considered early. Delay is dangerous because late surgery may not fully restore original visual function. [122]
Orbital cellulitis is treated in a hospital setting with broad-spectrum intravenous antibiotics, with consultation with an ophthalmologist and often an ear, nose, and throat specialist. If examination and tomography reveal the formation of a subperiosteal or orbital abscess, if vision deteriorates, or if there is no clear improvement with therapy, surgical drainage is considered. The key to success here is prompt initiation of treatment and reassessment of the condition over time. [123]
In cases of orbital compartment syndrome, treatment should not wait for imaging studies to be completed. Lateral canthotomy with inferior cantholysis for orbital decompression is considered the primary emergency procedure. Reviews emphasize that delay increases the risk of irreversible blindness, and favorable outcomes are more common with intervention within the first few hours. [124]
After stabilization of the underlying cause, a rehabilitation phase is often required. Some patients experience persistent diplopia, eyelid retraction, cosmetic deformity, or residual proptosis. In this case, during the inactive phase of the disease, orbital decompression, muscle surgery, and eyelid surgery are considered in stages. This sequence is particularly typical for thyroid eye disease and allows not only to save vision but also to restore function and appearance. [125]
| Treatment method | When to use |
|---|---|
| Moisturizing and protecting the cornea | For almost any reason, with incomplete closure of the eyelids [126] |
| Selenium and observation | Mild active thyroid eye disease in selected patients [127] |
| Intravenous methylprednisolone | Active moderate to severe thyroid eye disease with inflammatory phenotype [128] |
| Teprotumumab | Active moderate to severe disease with significant proptosis and either diplopia if available [129] |
| Mycophenolate, rituximab, tocilizumab | Isolated active or resistant cases [130] |
| Radiation therapy | In some patients with active disease, often as part of a combination strategy [131] |
| Orbital decompression | Significant proptosis, exposure keratopathy, optic neuropathy [132] |
| Intravenous antibiotics and drainage | Orbital cellulitis and abscesses [133] |
| Lateral canthotomy and cantholysis | Orbital compartment syndrome [134] |
Prevention
Prevention of proptosis as a symptom is always secondary, aimed at preventing its underlying causes and severe progression. The most well-documented preventative measure for thyroid eye disease is smoking cessation. At the same time, it is essential to maintain stable thyroid function and monitor even mild eye symptoms in patients with Graves' disease. [135]
If a patient is scheduled for radioactive iodine therapy, orbitopathy prophylaxis should be discussed in advance. Consensus documents note that, in some patients, steroid prophylaxis can reduce the risk of ocular deterioration. This is especially relevant if there are already active orbital symptoms or a high risk of their progression. [136]
For infectious causes, prompt treatment of sinusitis and dental infections, caution in facial injuries, the use of protective equipment when working with a risk of orbital injury, and early referral for pain, fever, and eyelid swelling are important. For patients with diabetes and immunodeficiency, the threshold for referral should be even lower. [137]
Secondary prevention of complications of established proptosis includes early corneal protection, regular examinations, visual function monitoring, and timely referral to a specialized center if moderate, severe, or vision-threatening orbitopathy is suspected. This often prevents the progression from reversible changes to permanent vision loss or complex reconstructive surgery. [138]
| Preventive step | What is it for? |
|---|---|
| Quitting smoking | Reduces the risk of more severe thyroid eye disease [139] |
| Maintaining euthyroidism | Slows down the progression of orbitopathy [140] |
| Thoughtful tactics for radioactive iodine | May reduce the risk of deterioration of the eye process [141] |
| Early treatment of sinusitis and injuries | Reduces the risk of orbital cellulitis and its complications [142] |
| Early corneal protection | Prevents ulcers and scarring [143] |
Forecast
The prognosis for proptosis is determined not by the degree of protrusion itself, but by the cause, the speed of its recognition, and whether visual function is affected. With timely detection, many causes respond well to treatment, and some changes may regress completely or partially. However, if optic nerve compression, severe infection, or compartment syndrome are missed, the prognosis worsens dramatically. [144]
In many patients with thyroid eye disease, the active inflammatory phase subsides over time, but residual cosmetic and functional impairments may persist. This is why, even with good inflammation control, patients sometimes later require decompression, strabismus correction, or eyelid surgery. Therefore, a good prognosis does not always mean complete restoration of appearance and visual comfort without additional treatment steps. [145]
With orbital cellulitis, the prognosis is usually better with early hospitalization and prompt initiation of intravenous antibiotic therapy. Conversely, delay increases the risk of abscess formation, intracranial spread, and persistent visual impairment. This is especially important in children because clinical deterioration can occur rapidly. [146]
Orbital compartment syndrome is the most time-sensitive. Here, the outcome depends on how quickly the blood supply to the orbit and optic nerve is restored. Reviews emphasize that the best results are achieved with early intervention, although an attempt at decompression is also justified in cases of later presentation. [147]
| Situation | Forecast |
|---|---|
| Early detection of the cause | Often good with timely therapy [148] |
| Thyroid eye disease | Inflammation may subside, but residual changes are not uncommon [149] |
| Orbital cellulitis | Good with early hospitalization and antibiotics, worse with delay [150] |
| Orbital compartment syndrome | The prognosis depends to a large extent on the time of decompression [151] |
FAQ
Are proptosis and exophthalmos the same thing?
In everyday speech, almost certainly, but in a more strict clinical sense, exophthalmos is more often associated with thyroid eye disease, while proptosis is a broader term for anterior displacement of the eye due to various causes. [152]
Does proptosis always indicate thyroid disease?
No. In adults, it's a common cause, but far from the only one. Infection, tumor, vascular pathology, hemorrhage, and inflammatory diseases of the orbit must be ruled out. [153]
Can proptosis resolve on its own?
Sometimes mild manifestations of thyroid eye disease partially regress, and recommendations describe spontaneous resolution in some patients. However, relying on this without an examination is dangerous, as proptosis may mask a condition requiring urgent treatment. [154]
What are the most dangerous symptoms?
Pain, redness, fever, double vision, decreased vision, headache, pulsating proptosis, and inability to close the eye. These are indications for immediate in-person assistance. [155]
What are the basic tests?
Physical examination, exophthalmometry, vision and eye movement assessment, thyroid function testing if suspected, and computed tomography or magnetic resonance imaging of the orbits. Further testing depends on the cause. [156]
Can drops alone be used for treatment?
No, if we're talking about true proptosis. Moisturizers are needed to protect the cornea, but they won't eliminate infection, tumor, vascular abnormality, or severe thyroid orbitopathy. [157]
When is surgery necessary?
Surgery is required for some tumors, abscesses, severe mechanical proptosis, vision-threatening optic nerve compression, and orbital compartment syndrome. The type of surgery depends on the cause. [158]
Is proptosis dangerous to vision?
Yes, it can be. The danger is associated with corneal exposure, limited movement, increased orbital pressure, and optic nerve compression. Infectious and compartmental causes are particularly dangerous. [159]
Key points from experts
George J. Cahaly, MD, PhD, is Professor of Medicine and Endocrinology and Director of the Endocrinology Outpatient Clinic at the Johannes Gutenberg University Medical Center in Mainz. His work and contributions to consensus documents emphasize the critical importance of early severity stratification, monitoring of thyroid status, and rapid referral to specialized care when vision is compromised in thyroid eye disease. [160]
Terry J. Smith, MD, is a professor of ophthalmology, visual sciences, and internal medicine at the University of Michigan. His research has been instrumental in understanding that orbital tissue in thyroid eye disease has unique molecular features and that the insulin-like growth factor pathway is an important therapeutic target. This understanding formed the basis for the targeted therapy teprotumumab. [161]
Luigi Bartalena, MD, Professor of Endocrinology, Director of the Postgraduate School of Endocrinology and Metabolism at the University of Insubria, is one of the leading authors of the European guidelines on orbitopathy in Graves' disease. His clinical thesis essentially boils down to the following: treatment should be personalized, and the choice between glucocorticosteroids, targeted therapy, radiation therapy, and decompression is determined not only by the diagnosis but also by what is predominant in the patient—inflammation, proptosis, diplopia, or a threat to vision. [162]
If necessary, the next message can be formatted to present this article in a more "website-like" format: with a lead, a "Briefly" section, a "When is it urgent" table, and a separate list of sources for editorial layout.