Medical expert of the article

New publications
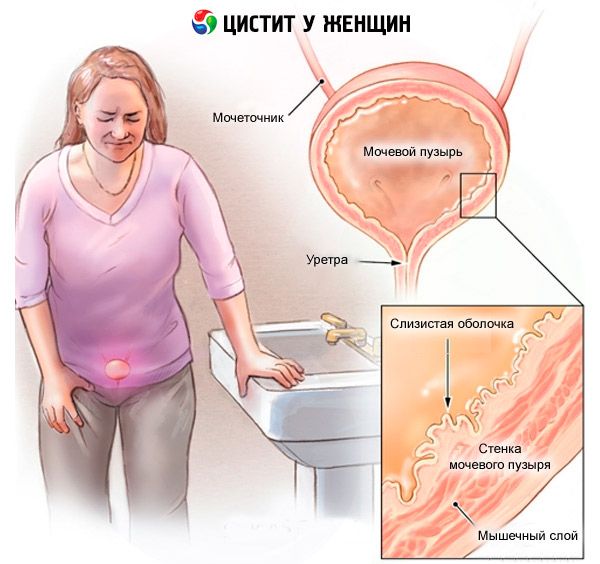
Cervical cystitis of the bladder in women and men
Last updated: 29.03.2026

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Cervical cystitis, or trigonitis, is an inflammatory and metaplastic process in the trigone of the bladder (the area between the ureteral orifices and the neck/internal opening of the urethra). Unlike "regular" cystitis, which can involve any part of the mucosa, trigonitis is localized specifically at the base of the bladder and therefore most often produces symptoms associated with urgency, a burning sensation upon completion of urination, and discomfort above the pubis. Histologically, trigonitis is characterized by non-keratinizing squamous cell metaplasia of the trigone urothelium—an adaptive remodeling of cells under the influence of chronic irritation and hormonal factors. [1]
Trigonitis is significantly more common in women than in men: in some adults, it is a finding during cystoscopy and causes no symptoms, while in others, it is accompanied by symptoms resembling recurrent cystitis or painful bladder syndrome. Observations suggest that trigonitis lesions/associated changes ("cystitis cystica/glandularis") are most often localized in the cervix and trigone. [2]
It's important not to confuse trigonitis with keratinizing squamous metaplasia: they are similar in appearance, but leukoplakia is considered a precancerous condition and is managed differently. A biopsy can help differentiate between the two: trigonitis is characterized by nonkeratinizing metaplasia without dysplasia; leukoplakia is characterized by keratinization, acanthosis, and atypia. [3]
The attitude towards trigonitis is being revised: there is increasing evidence that this is a zonal-specific condition that contributes to chronic lower abdominal symptoms in some patients and requires a phenotype-oriented approach (from correction of irritant factors to instillations of hyaluronate and, in some cases, endoscopic coagulation). [4]
Code according to ICD-10 and ICD-11
In ICD-10, trigonitis is coded under a separate heading, N30.3 “Trigonitis”; in the details of some publications, there are subheadings, N30.30 “Trigonitis without hematuria” and N30.31 “Trigonitis with hematuria”. If necessary, the identified infectious agent and associated conditions (e.g., voiding dysfunction) are additionally coded. [5]
In ICD-11, trigonitis is listed as a separate category, GC00.0 "Trigonitis," in the "Cystitis" section. The system encourages post-coordination—adding details about the cause (infectious/non-infectious), context (pregnancy, radiation therapy), and complications. This allows for more accurate clinical presentation in documents and studies. [6]
Table 1. Trigonite coding
| Essence | ICD-10 | Comment | ICD-11 | Comment |
|---|---|---|---|---|
| Trigonitis (cervical cystitis) | N30.3 | There are subcategories for hematuria. | GC00.0 | Allows post-coordination |
| Infectious cystitis | N30.0/N30.8/N30.9 | By context | GC00.1/GC00.Y/GC00.Z | Add a stimulant |
| Interstitial cystitis | N30.1 | Other nosology | GC00.3 | A distinct phenotype |
Epidemiology
Precise population estimates of symptomatic trigonitis are scarce, but cystoscopic series suggest that metaplastic changes in the trigone are common—some studies report up to 40% of adult women (pseudomembranous trigonitis), with many women asymptomatic. These data emphasize that trigonitis is not uncommon, and its clinical significance depends on symptoms. [7]
Histological variants of reactive mucosal changes ("cystitis cystica/glandularis") are also predominantly localized in the cervix and trigone. They are often associated with chronic irritation and infection, and the finding itself does not indicate a tumor. [8]
High-quality treatment studies are scarce: reviews note a “mosaic” of methods (antibiotics as indicated, instillations of hyaluronic acid/glycosaminoglycan layer components, endoscopic coagulations), while long-term randomized data are limited and standardized prescription criteria have not yet been established. [9]
Trigonitis is more often described in women of reproductive age and perimenopause; in men, the symptomatic variant is less common and is often associated with voiding dysfunction, prostatitis, or catheterization. The EAU 2024 General Guidelines for Urinary Tract Infections help standardize the approach when a bacterial component is present. [10]
Reasons
Triggers for trigonitis include chronic irritation and local hormonal influences. Irritants include recurrent lower urinary tract infections, exposure to spermicides, catheterization, urinary dysfunction (residual urine), and chemical/mechanical irritation. These stimuli maintain inflammation and metaplasia specifically in the trigone area. [11]
The hormonal hypothesis is based on observations of a more frequent occurrence of nonkeratinizing metaplasia in women of childbearing age and its dynamics in the context of changes in estrogen levels. This is an adaptive response of the trigone urothelium, not a tumor process. [12]
Coexisting morphological changes—cystitis cystica/glandularis—are interpreted as a reaction to chronic inflammation/obstruction; they are most often localized in the cervix and triangle. Their detection requires clinical and morphological correlation, but in itself does not dictate aggressive treatment. [13]
A separate line is the differentiation from keratinizing leukoplakia: it has different causes and clinical significance (risks of precancerous lesions). This is why, when the picture is alarming, a biopsy is prescribed. [14]
Risk factors
Key factors include recurrent bladder infections, use of spermicides and diaphragms, frequent catheterization/instrumentation, pelvic floor dysfunction and incomplete voiding, postmenopause with estrogen deficiency, and in men, obstruction due to prostatic hyperplasia and chronic prostatitis.[15]
Disturbances in urochemistry (pH shift, reduction of the protective glycosaminoglycan layer of the urothelium) make the triangle more vulnerable to irritation. This explains why some patients respond well to restoration of the GAG layer with hyaluronic acid instillations. [16]
Long-term self-medication with antibiotics without confirmed infections worsens dysbiosis and does not treat trigonitis as a metaplastic condition. Therefore, the strategy always begins with confirming or ruling out a bacterial process. [17]
Table 2. Risk factors and possible interventions
| Factor | Mechanism | What helps? |
|---|---|---|
| Recurrent UTIs | Chronic inflammation of the triangle | Treatment of EAU/AUA episodes, prophylaxis without antibiotics |
| Spermicides/diaphragm | Chemical irritation | Changing contraception |
| Residual urine, obstruction | Stagnation, contact with urine | Correction of urodynamics, pelvic floor physiotherapy |
| Catheter/instruments | Mucosal injury | Minimize interventions, asepsis |
| Estrogen deficiency | Weakening of the vaginobiome, pH↑ | Vaginal estrogens in postmenopause |
Pathogenesis
The urothelium of the trigone responds to chronic irritation with squamous cell metaplasia (without keratinization), increasing local inflammation and thinning and fraying of the protective GAG layer. This leads to hypersensitivity of stretch and pain receptors, resulting in imperative urges and a stabbing pain at the end of urination. [18]
In “adjacent” reactive conditions (cystitis cystica/glandularis), cysts and glandular structures are formed in the lamina propria of the urothelium, which reflects a long-term irritable background; more often, these are clinically silent foci in the cervix/triangle. [19]
The neuroinflammatory component and cross-sensitization with pelvic floor muscles are discussed, which brings some patients closer to the "vesicocentric" pain phenotype (at the intersection with bladder pain syndrome). Therefore, a combined approach is often needed in rehabilitation. [20]
Keratinization is not characteristic of trigonitis; its appearance moves the conversation into the realm of leukoplakia (a precancerous condition) and requires a different approach. [21]
Symptoms
The most typical symptoms are: frequent and urgent urge to urinate, discomfort/burning at the end of urination, a feeling of incomplete emptying, and suprapubic pain. In women, there is often a connection with sexual intercourse and cycle phases (due to hormonal fluctuations and the urovaginal ecosystem). [22]
Concomitant infections can cause cloudy urine, leukocyturia, and the need for frequent antibacterial treatment. However, symptomatic trigonitis is also possible with sterile cultures, in which case non-antibacterial methods become more important. [23]
In men, symptoms are more often "lower": terminal pain, nocturnal urges, intermittent urinary flow. Here, it is especially important to rule out prostatitis and obstruction. [24]
Table 3. Symptoms and possible explanations
| Symptom | A common cause in the context of trigonitis |
|---|---|
| Cutting pain at the end of urination | Inflammation/hypersensitivity of the cervix |
| Frequent small portions | Irritation of the triangle receptors |
| Enhancement after sex | Chemical-mechanical irritation, dysbiosis |
| Symptoms of "clean" crops | Metaplasia, GAG layer deficiency, neuroinflammation |
Forms and stages
Conventionally, the following are distinguished:
- Asymptomatic trigonitis (incidental finding during cystoscopy).
- Symptomatic non-infectious trigonitis (sterile cultures, pronounced “irritating” symptoms).
- Trigonitis with recurrent UTIs (intermittently positive cultures).
- Trigonitis-like picture in comorbid conditions - pelvic floor dysfunction, obstruction, catheter. [25]
According to morphology: nonkeratinizing metaplasia (trigonitis) versus keratinization (leukoplakia). The latter requires a different route (biopsy, active intervention). [26]
Symptom severity is assessed using a voiding diary, pain scales, and quality of life impact scales; this helps monitor the effect of therapy and decide on escalation. [27]
Complications and consequences
The main risk is chronic pelvic discomfort, sleep disturbance, and sexual dysfunction. Frequent "empirical" antibiotic use in sterile cultures creates unnecessary drug pressure and promotes resistance. Therefore, a strategy of "antibiotic-free prophylaxis → targeted antibacterial therapy only for confirmed infection" is considered optimal. [28]
In a mixed scenario (trigonitis + UTI), without correcting the underlying factors (residual urine, spermicides, estrogen deficiency), relapses will recur. This is why interventions "at the sources of irritation" are a mandatory part of the plan. [29]
Keratinization/leukoplakia is a different story with a risk of malignancy; here, delay in biopsy and observation is undesirable. [30]
When to see a doctor
Urgently - in case of fever, flank pain, nausea/chills (suspected pyelonephritis), macrohematuria, severe urinary retention. This goes beyond the scope of "local trigonitis." [31]
In the near future – if persistent "irritating" symptoms occur, especially if urine cultures are repeatedly negative: it is important to rule out leukoplakia, interstitial cystitis, neurogenic and obstructive causes. The decision regarding cystoscopy is made by a urologist. [32]
For recurrent UTIs, culture before antibiotics for each episode; for 2+ episodes within six months, a prevention plan starting with non-antibacterial measures. [33]
Diagnostics
A basic step is a general urine analysis and culture for each symptomatic episode before treatment. This distinguishes infectious exacerbations from the "sterile" phases of trigonitis and helps guide therapy. The EAU 2024 guidelines emphasize the importance of rational antibacterial tactics. [34]
Cystoscopy is indicated for persistent symptoms, atypia, hematuria, and the ineffectiveness of empirical measures. The physician evaluates the trigonium, cervix, and satellite changes; if leukoplakia is suspected, a biopsy is taken. Visually, trigonitis appears as pale, matte, or erythematous areas with a "velvety" surface, but histology is decisive. [35]
Urodynamics/ultrasound with residual urine assessment – as indicated (feeling of incomplete emptying, nocturnal urges, male gender, neurological complaints). This helps identify triggers such as congestion, obstruction, and detrusor overactivity. [36]
Comorbidity diagnosis: vaginal dysbiosis, postmenopausal atrophy, prostatitis in men, and the effects of contraceptives. Without their correction, a lasting effect is difficult to achieve. [37]
Table 4. What, why and when to prescribe
| Study | Target | When it's especially important |
|---|---|---|
| Urine culture | Distinguish an infectious episode | Every episode before antibiotic |
| Cystoscopy ± biopsy | Confirm trigonitis, exclude leukoplakia | Persistent symptoms, hematuria |
| Ultrasound/residual urine | Identify congestion/obstruction | Men, neurogenic complaints |
| Hormonal status/microbiota assessment | Find adjustable triggers | Postmenopause, relapses |
Differential diagnosis
- Recurrent bacterial cystitis - positive cultures, rapid response to antibiotics, no persistent "sterile" pain.
- Interstitial cystitis/bladder pain syndrome - sterile cultures, pain on filling, phenotype-directed therapy; often overlaps symptoms with trigonitis. [38]
- Keratinizing leukoplakia - cystoscopically similar, but histologically and clinically different (precancerous potential); requires biopsy and active intervention. [39]
- Pelvic floor dysfunction/obstruction—a feeling of incomplete evacuation, intermittent urine stream, and significant residual urine. Treatment is aimed at eliminating the underlying cause. [40]
Table 5. "Similar - not similar"
| Sign | Trigonite | Recurrent bacterial cystitis | IC/bladder pain | Leukoplakia |
|---|---|---|---|---|
| Urine culture | Often negative | Positive in episode | Negative | May be negative |
| Cystoscopy | Metaplasia without keratinization | Non-specific. inflammation | Often without foci | Whitish plaques, keratinization |
| Risk of oncotransformation | No data | No | No | There is (precancerous) |
Treatment (very detailed; both classic and new methods)
1) Base: eliminate irritants and build a “ladder”
- Confirm/exclude bacterial infection and treat episodes according to EAU/AUA (nitrofurantoin, fosfomycin, etc. - according to the local antibiogram). Without culture, do not prescribe "prophylactic" courses. [41]
- Contraception without spermicides, careful intimate hygiene, avoiding aggressive gels/deodorants.
- Vaginal estrogens in postmenopausal women with atrophy (restore the vaginobiome and reduce the “irritating” effect of urine on the triangle). [42]
- Pelvic floor physiotherapy for concomitant hypertonic pelvic pain, urination training.
2) Restoration of the GAG layer (instillation)
Hyaluronic acid instillations (sometimes in combination with chondroitin sulfate) are aimed at restoring the damaged glycosaminoglycan barrier. In a European study in women with trigonitis, weekly instillations for 10 weeks, then monthly for up to 10 months, resulted in a reduction in symptoms; histological changes were delayed, confirming the clinical relevance of the method. This approach is particularly logical in cases of sterile cultures and "vesicle-centric" symptoms. [43]
3) Targeted antibacterial therapy - only if indicated
In cases of positive cultures, treatment is directed specifically at the pathogen and is brief. In cases of frequent relapses, non-antibacterial strategies (methenamine, cranberry, etc.) and factor correction are prioritized; continuous antibiotic prophylaxis is considered as a last resort and only after conservative measures have failed. The EAU 2024 Guidelines emphasize this. [44]
4) Endoscopic methods (in selected cases)
In refractory symptomatic trigonitis, electrocoagulation/electrofulguration of trigonal lesions is considered. Prospective series in women with recurrent infections and confirmed trigonitis have shown long-term symptom reduction in some patients; however, these are not randomized studies, and this method is reserved for cases unresponsive to conservative therapy. Laser coagulation options have also been described. [45]
5) What doesn't work with "sterile" trigonitis
Long-term "just in case" antibiotics, antiseptic douches, and aggressive diuretic regimens do not eliminate metaplasia and the barrier defect, but worsen the microbiome and quality of life. [46]
Table 6. Therapy “ladder” for symptomatic trigonitis
| Step | Measure | When |
|---|---|---|
| 1 | Correction of triggers: hygiene, refusal of spermicides, fluid regimen | To everyone |
| 1 | Treatment of culture-confirmed UTIs | If the culture is positive |
| 2 | Vaginal estrogens (postmenopause) | Atrophy, relapses |
| 2 | Instillations of HA ± CS | Sterile cultures, "bubbly" phenotype |
| 3 | Endoscopic coagulation of foci | Refractory cases after conservative measures |
Prevention
- Behavioral: drink enough fluids, do not hold back the urge to urinate, practice gentle intimate hygiene, wear cotton underwear, avoid spermicides and scented products.
- Monitoring of urogynecological background: treatment of vaginitis, restoration of vaginobiome, local estrogens in postmenopause.
- Urodynamics: treat obstruction/residual urine, teach proper voiding, pelvic floor physiotherapy if necessary.
- Infections: in cases of episodes - culture before treatment; to prevent relapses - priority to non-antibacterial measures. [47]
Table 7. Prevention - a quick reminder
| Direction | Tool |
|---|---|
| Reduced irritation | Care without aggressive means, refusal from spermicides |
| Restoring the barrier | Instillations of GC/HS as indicated |
| Vaginal health | Estrogens in postmenopause, treatment of vaginitis |
| Urodynamics | Correction of obstruction/residual urine |
| Antibiotics | Only by sowing, prevention - in extreme cases |
Forecast
In a significant proportion of patients, symptoms can be controlled with a combination of first- and second-line measures (care, factor correction, instillations). The prognosis is better with early differentiation of trigonitis and exclusion of leukoplakia/interstitial cystitis. [48]
If trigonitis coexists with recurrent infections, a lasting effect is achieved after eliminating the triggers (obstruction, spermicides, atrophy) and rational use of antibiotics. Endoscopic methods are reserved for refractory cases. [49]
If leukoplakia is suspected, the prognosis and tactics change: a biopsy and active management are required. [50]
FAQ
1) Is this the same as bacterial cystitis?
Not always. Trigonitis is often a non-infectious metaplastic condition of the triangle. Cultures may be negative, and antibiotic treatments are ineffective. [51]
2) How to confirm the diagnosis? The
diagnosis can be suspected based on the patient's complaints, but confirmation is possible with a cystoscopy; if in doubt, a biopsy is performed to rule out keratinization (leukoplakia). A urine culture is necessary to rule out any concomitant infection. [52]
3) What really helps with "sterile" cultures?
Correction of triggers, restoration of the GAG barrier with instillations of hyaluronate (± chondroitin), pelvic floor physiotherapy; in postmenopausal women - vaginal estrogens. [53]
4) Is trigonitis dangerous in terms of cancer?
Trigonitis itself (nonkeratinizing metaplasia) is not considered precancerous. However, it must be differentiated from keratinizing leukoplakia, which carries a risk of malignancy. [54]
5) Can I just "cauterize" it and forget about it?
Endoscopic coagulation does not help everyone and is considered an escalation after conservative therapy; long-term randomized data are limited. The decision is made on an individual basis. [55]
Who to contact?