Medical expert of the article

New publications
Melioidosis
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Melioidosis (or Whitmore's disease) is an acute infectious disease of bacterial etiology; it often manifests as community-acquired pneumonia or sepsis; it has a high mortality rate. The bacteria are widespread in soil and water in the tropics. They enter the human body through direct contact with a contaminated source, especially during the rainy season.
Epidemiology
The distribution features or epidemiology of melioidosis are well studied: the infection is endemic in Southeast Asia. For example, in Thailand, there are 36 cases of melioidosis per 100,000. In Australia, this bacterium is contracted in tropical climate zones – in the north of the continent. In many Asian countries, the B. pseudomallei bacterium is so widespread that it is even detected in laboratory cultures. About 75% of registered cases of melioidosis are detected during tropical rainy seasons.
Nowadays, melioidosis is increasingly diagnosed in Latin American countries, and individual cases (among tourists and immigrants) are noted in the USA, Africa, and the Middle East.
Routes of infection for B. pseudomallei include direct contact with water and soil, and infection through skin lesions (abrasions, cuts, etc.), drinking contaminated water, and inhalation of dust. Seasonal monsoon rains significantly increase aerosolization of the bacteria, which also results in their entry through the upper respiratory tract. Several cases of human-to-human transmission have been reported.

Causes melioidosis
The causes of melioidosis are human infection with the bacterium Burkholderia pseudomallei, which belongs to the phylum Proteobacteria, class Betaproteobacteria.
The causative agent of melioidosis is a pathogenic gram-negative aerobic rod-shaped bacterium. This bacterium is intracellular and is quite mobile due to the presence of a filament (thread-like flagellum).
Burkholderia pseudomallei is a saprotroph, meaning it lives in waterlogged soil and water, where it gets its nutrients from rotting organic matter. The bacteria can infect many animals (including farm and domestic ones) and birds, and their excrement additionally contaminates the soil and water. Not long ago, this proteobacteria was discovered in dolphins and sea lions at the Hong Kong Ocean Park aquarium.
Risk factors
The disease usually develops in the fourth and fifth decades of life, especially among those with chronic comorbidities such as diabetes mellitus, alcoholism, immunosuppression, and renal failure.
Pathogenesis
The pathogenesis of this infectious disease is associated with the defeat of tissue macrophages by the B. pseudomallei bacteria and the suppression of immune C-proteins produced by phagocytes, in particular, betaglobulin C3b. And thus the bacteria manage to neutralize the membrane-attacking (lysing) complex and, moreover, destroy the membranes of endocytic phagolysosomes, which are formed to neutralize antigens.
In addition, B. pseudomallei is capable of polymerizing the structural protein actin and spreading from cell to cell to form giant multinucleated cells. The melioidosis pathogen enters various organs by hematogenous and lymphogenous routes and leads to the development of inflammation and necrosis.
Microbiologists note that the bacterium Burkholderia pseudomallei is an “accidental pathogen” because it does not need other organisms to reproduce and replicate RNA, and for the bacterium, infecting humans is an “evolutionary dead end.”
Doctors have identified the main risk factors for developing melioidosis: diabetes, chronic renal failure, high alcohol consumption, liver pathologies (cirrhosis), thalassemia, chronic lung diseases, HIV and other immunosuppressive conditions.
Symptoms melioidosis
The incubation period of melioidosis varies depending on the number of bacteria that have entered the body and the route of infection and can range from several hours to 14-28 days. The first signs of the disease appear much faster in the presence of risk factors (listed above).
The disease has an incredibly diverse list of clinical manifestations, including such symptoms of melioidosis as: fever, chills, cough, difficulty breathing, headache, drowsiness, chest and abdominal pain, weight loss, convulsions, enlarged spleen and liver, inflammation of the bladder, prostate gland, joints, soft tissues, regional lymph nodes, etc.
Forms
Infectiologists distinguish the following types of meliodoses (or rather clinical forms of its manifestation): localized, pulmonary, septic. There are also acute, subacute, chronic, recurrent and latent (hidden) forms of this disease.
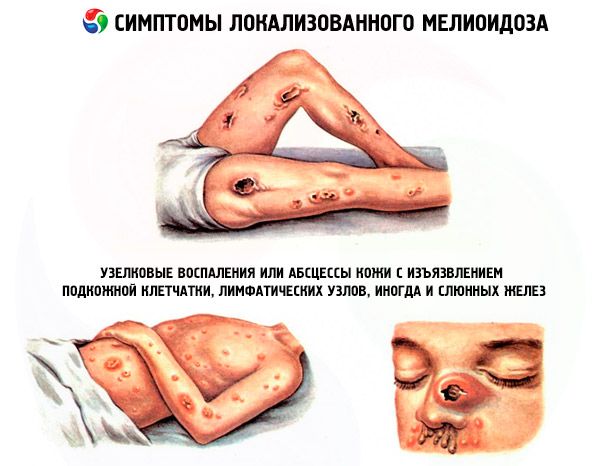
Manifestations of localized meliodiza: ulcers, nodular inflammations or skin abscesses with ulceration of the subcutaneous tissue, lymph nodes, and sometimes salivary glands. The first signs are fever and muscle pain in the affected area. In this case, subacute infection (usually focal) can affect almost any organ system and be a source for subsequent bacteremia.
The symptoms of melioidosis, the most common pulmonary form, are all the signs of purulent bronchopneumonia, including pulmonary abscesses and purulent pleural effusion. Characteristic manifestations include high temperature with fever, headache and chest pain, cough (non-productive or with sputum), loss of appetite, muscle soreness.
In the septic form – a systemic infection in the blood – a life-threatening clinical picture of sepsis and septicocemia develops, often causing concomitant pneumonia and abscesses of the liver and spleen. The infection can spread to the bones, joints, skin, and soft tissues. In this form of the disease, the infection especially quickly leads to the terminal stage, which within 7-10 days after the onset of symptoms ends in septic shock and death.
Although acute forms are most typical for this disease, there are many cases of latent infection, which is asymptomatic and reactivates within a year. And with latent melioidosis, symptoms may appear several years after infection, usually in combination with a change in immune status. Researchers believe that B. pseudomallei bacteria can remain inactive in macrophages for a long time.
 [ 19 ], [ 20 ], [ 21 ], [ 22 ], [ 23 ], [ 24 ], [ 25 ], [ 26 ]
[ 19 ], [ 20 ], [ 21 ], [ 22 ], [ 23 ], [ 24 ], [ 25 ], [ 26 ]
Complications and consequences
The consequences and complications of melioidosis vary depending on the severity of the lesion, as well as timely treatment. In the case of acute severe melioidosis, the mortality rate is from 30 to 47%; in cases of delayed treatment of septicemia, the mortality rate exceeds 90% (in septic shock - about 95%). According to Nature Reviews Microbiology, with adequate medical care, the mortality rate is much lower, for example, the mortality rate of patients with B. pseudomallei in Australia is 19%.
Diagnostics melioidosis
In domestic practice, the diagnosis of septic forms of melioidosis is considered “problem-free” if it turns out that the patient was in endemic regions.
According to foreign epidemiologists, the diagnosis of meliodiza is difficult due to non-specific symptoms and requires laboratory tests for the presence of Burkholderia pseudomallei in the body. For this, blood, sputum, urine or pus samples are taken from patients.
In this case, the blood test for acute forms of melioidosis may be negative, but this does not exclude the disease. A common reason for difficulties in making a correct diagnosis is the virtual absence of approved diagnostic reagents for immunological or molecular diagnostic tests for the presence of B. pseudomallei.
Even in areas where melioidosis is endemic, laboratory diagnostic difficulties arise, and the pathogen may be mistakenly identified as Chromobacterium violaceum, Burkholderia cepacia, or Pseudomonas aeruginosa, the Journal of Medical Microbiology reports.
Instrumental diagnostics cannot identify the bacteria, but it is used to assess the condition of the affected organs: chest X-ray, ultrasound or CT of the visceral organs are performed.
Differential diagnosis
Differential diagnosis of the pulmonary form of melioidosis is very important, since it can look like mild bronchitis or severe pneumonia.
Who to contact?
Treatment melioidosis
Currently, the only effective treatment for melioidosis is a long course of antibiotics. Initial treatment consists of intravenous antibiotics for 14 days.
The causative agent of melioidosis exhibits resistance to many antibiotics, in particular, macrolides and drugs of the aminoglycoside, tetracycline and fluoroquinolone group.
At the initial stage of the disease, the drugs of choice are the cephalosporin antibiotic Ceftazidime (Zacef, Orzid, Kefadim, Sudocef and other trade names) and the beta-lactam antibiotic Meropenem (Meronem, Imipenem).
Without antibiotics, the septic form of melioidosis is fatal in 9 cases out of 10. The use of antibacterial drugs reduces the number of deaths in uncomplicated cases by 9 times, and in cases of bacteremia or severe sepsis - by only 10%.
As a rule, the body responds to appropriate antibacterial therapy quite slowly: on average, fever can last up to 6-8 days.
As epidemiologists note, 10-20% of patients in endemic regions experience relapses (due to repeated infection or the initially multifocal form of the disease), so treatment of melioidosis must necessarily include eradication therapy, the goal of which is to completely destroy B. pseudomallei in the body.
For this purpose, Trimethoprim and Sulfamethoxazole (or their combination – Co-trimoxazole) are taken orally for the next 8 weeks. Less effective are Doxycycline (Vibramycin, Doxacin) and the combined beta-lactam antibiotic Amoxiclav (amoxicillin + clavulanic acid).
Prevention
Currently, specific prevention of melioidosis is not possible, since there is no vaccine against B. pseudomallei yet.
Since the transmission of infection from person to person is considered an emergency (and is questioned by experts), the main way is to avoid contact with soil and standing water in endemic regions. For example, in Southeast Asian countries, people working in rice fields are warned about the dangerous infection and are advised to work in rubber boots and gloves (so that the bacteria does not enter the body through minor skin lesions).
If there are any lesions on the skin, cover them with a waterproof bandage and avoid contact with dirt or water in areas where the disease is present.
It is essential to wash your hands only in clean water and boil any water used for drinking and cooking. It is also recommended to wash vegetables and fruits with boiled water. It has been established that the pathogenic bacteria that causes melioidosis die when water is heated above +74°C for 10 minutes.
To prevent B. pseudomallei, it would be possible to use disinfectants, but, as it turns out, the bacterium does not react to phenolic preparations and tolerates normal bactericidal concentrations of chlorine very well…
Forecast
Melioidosis is an infectious disease that often leads to fatal consequences, so doctors define its prognosis as unfavorable. But antibiotics can save from death.
The latest issue of the journal Nature Microbiology reports that 165,000 cases of the disease are registered worldwide each year.
[ 39 ]