Medical expert of the article

New publications
Hemophagocytic syndrome in children: primary, secondary
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
A rare and difficult to define disease is hemophagocytic syndrome, otherwise known as hemophagocytic lymphohistiocytosis. This severe disease is associated with the occurrence of failure of many organs as a result of uncontrolled activation of the effector component of cellular immune defense.
In hemophagocytic syndrome, there is a strong increase in the functionality of toxic T-lymphocytes and macrophages, which leads to the production of numerous anti-inflammatory cytokines. In turn, this process entails an intense systemic inflammatory reaction and large-scale dysfunction of many organs.
Causes hemophagocytic syndrome
Hemophagocytic syndrome is most often primary, that is, hereditary in nature as a result of a genetic disorder in the functioning of macrophages.
Secondary hemophagocytic syndrome is also called acquired: it is associated with various infectious pathologies, tumor processes, autoimmune diseases, and congenital metabolic disorders.
In the classic variant of the hereditary type of hemophagocytic syndrome, children are often placed for treatment in the intensive care unit or ICU at infectious hospitals, diagnosing septic complications or intrauterine generalized infection. The diagnosis of hemophagocytic syndrome is often established after a fatal outcome.
However, even seemingly ordinary infectious diseases of viral or microbial origin can cause such a complication as life-threatening hemophagocytic syndrome.
Hemophagocytic syndrome in adults is almost always secondary: most often, the pathology develops against the background of lymphoproliferative diseases and chronic EBV infections.
Hemophagocytic syndrome in children can be either primary or secondary – as a result of previous infectious diseases (chickenpox, meningoencephalitis, etc.).
Symptoms hemophagocytic syndrome
The symptoms of the syndrome were first described in the middle of the last century. The following characteristic symptoms were identified:
- stable febrile condition;
- decrease in the level of hematopoietic substances;
- enlargement of the liver and spleen;
- expressive hemorrhagic syndrome.
Patients may exhibit liver failure, high ferritin and transaminase levels, clear neurological findings with CNS dysfunction, high serum triglyceride levels, accelerated blood clotting and coagulopathy.
Often, patients have enlarged lymph nodes, skin rash, yellowing of the sclera, skin and mucous membranes, as well as swelling.
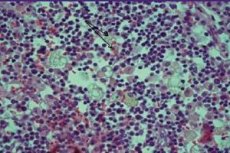
The parenchyma of the spleen, sinusoidal liver capillaries, lymph node sinuses, bone marrow and central nervous system are characterized by diffuse infiltration by active macrophages against the background of hemophagocytic symptoms. Depletion of lymphoid tissue occurs. Liver examination reveals lesions typical of the chronic form of persistent inflammation.
Forms
There are two clinical forms, which are quite difficult to differentiate at first.
- Primary hemophagocytic lymphohistiocytosis, which is an autosomal recessive pathology, in the development of which the mutation of the perforin gene is of primary importance.
- A secondary form of hemophagocytic lymphohistiocytosis that develops as a result of excessive immune activity of the mononuclear phagocyte chain.
Complications and consequences
- Addition of infection with subsequent intoxication. This complication is characterized by gradual loss of function of the main organs and systems, fever, and exhaustion of the patient.
- Malignant transformation of cells. Malignancy usually represents the development of lymphoma, leukemia and other malignant diseases.
- Autoimmune pathologies are a kind of aggressive reaction of the patient’s own immune defense.
- Persistent decrease in immunity with the development of an immunodeficiency state.
- Insufficiency of kidney and liver function.
- Internal bleeding, hemorrhages.
- Death of a patient from total organ dysfunction or from septic complications.
Diagnostics hemophagocytic syndrome
If the family history is not burdened, it is very difficult to determine the primary or secondary nature of hemophagocytic syndrome. In order to make an accurate diagnosis, it is necessary to conduct histological differentiation of hemophagocytosis.
Many diseases are difficult to diagnose using only information obtained from tissue biopsies: lymph nodes, liver and bone marrow.
Conducting immunological studies that allow us to see the suppressed function of NK-cell structures and an increase in the content of the interleukin-2 receptor cannot serve as a basis for making a diagnosis. In addition, the features of the clinical picture, damage and dysfunction of the central nervous system and changes in the composition of the patient's blood are taken into account.
The final point in making a diagnosis is the data from molecular genetic analysis.
Differential diagnosis
Differentiating the disease is extremely difficult, and the approach should be determined depending on the patient's age. In pediatrics, it is important to detect genetic forms of hemophagocytic syndrome as early as possible, analyzing all possible factors that may indicate a hereditary type of pathology.
Thus, rapid development of the syndrome during the first 12 months of life with an uncomplicated family history is typical for the primary form of hemophagocytic syndrome. The expression of perforin on NK-cell structures detected using flow cytofluorometry and molecular genetic testing of perforin helps establish the correct diagnosis in approximately 30% of cases of hereditary hemophagocytic syndrome. The simultaneous occurrence of the disease against the background of albinism is detected in the following syndromes:
If the inheritance is X-linked, that is, when the disease develops in related men on the mother's side, then the most likely is the presence of autoimmune lymphoproliferative syndrome.
In secondary hemophagocytic syndrome, the main thing is to promptly detect malignant tumors, which are most often the cause of the syndrome in adulthood.
Who to contact?
Treatment hemophagocytic syndrome
Treatment for hemophagocytic syndrome is quite complex: the success of such treatment largely depends on the age of the patient and how timely the disease was detected.
Therapeutic regimens for hemophagocytic syndrome include the use of glucocorticosteroids (Dexamethasone), cytostatics (Etoposide, Cyclosporine A). Cytostatics are prescribed to suppress the proinflammatory action of phagocytes with subsequent allogeneic stem cell transplantation.
A single treatment regimen used for hemophagocytic syndrome has not yet been determined. Etiotropic treatment is considered insufficient to combat the syndrome, and the use of immunosuppressants can negatively affect the course of the viral-bacterial process.
Injections of high doses of immunoglobulin are recommended, based on the amount of 1-2 mg per kilogram of the patient's weight per day.
Plasmapheresis can be prescribed as part of pathogenetic treatment to monitor hypercytokinemia.
The mainstay of treatment is splenectomy and donor bone marrow transplant.
Prevention
Experts currently do not have clear information about methods of preventing primary hemophagocytic syndrome, since the causes of the development of this pathology have not been fully studied.
As for secondary hemophagocytic syndrome, preventive measures may include the following:
- competent and timely treatment of viral and microbial infections;
- qualified treatment of autoimmune pathologies under the supervision of a medical specialist in rheumatology.
Forecast
The prognosis for hemophagocytic syndrome is considered extremely unfavorable, as can be seen from the statistical information: six deaths among seven patients. The maximum survival time at the moment is two years.
Hemophagocytic syndrome is considered a very complex and insidious disease, which today “competes” only with the human immunodeficiency virus infection, and in terms of the frequency of consequences even exceeds HIV.
 [ 27 ]
[ 27 ]