A heart
The heart (cor) is a hollow muscular organ that pumps blood into the arteries and receives venous blood. The heart is located in the thoracic cavity in the organs of the middle mediastinum. In shape, the heart is like a cone. The longitudinal axis of the heart is directed obliquely - from right to left, from top to bottom and from behind in front; it is located two-thirds in the left half of the thoracic cavity. The apex cordis is turned downward, to the left and forward, and the wider base of the heart (upward and posteriorly).
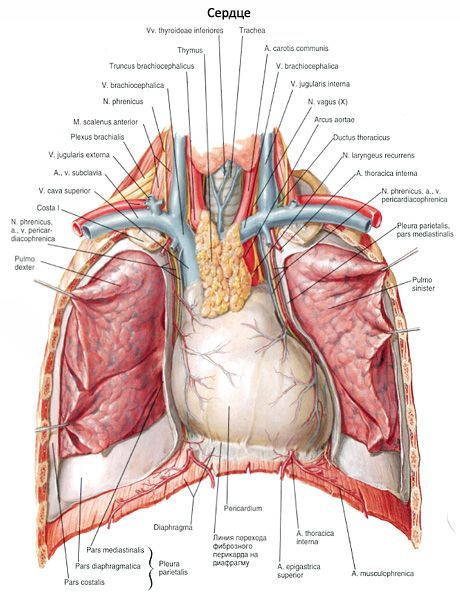
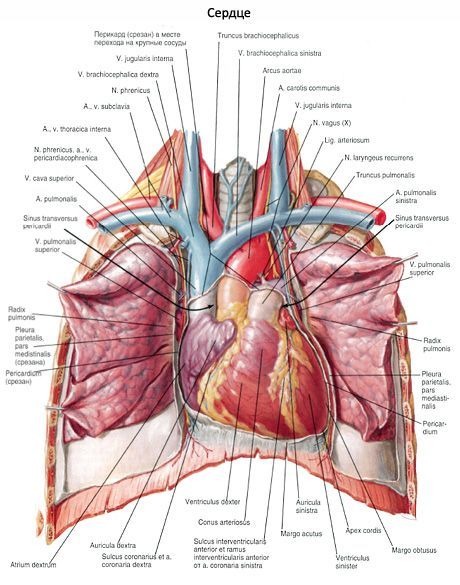
The thoracic-costal (anterior) surface of the heart (facies sternocostalis, s.anterior) is more convex, facing the posterior surface of the sternum and the cartilaginous ribs. The lower surface faces the diaphragm and is called the diaphragmatic surface (facies diaphragmatica, s.inferior). In clinical practice, this surface of the heart is called back. The lateral surfaces of the heart are facing the lungs, each of them is called the facies pulmonalis. Wholely these surfaces (or edges) are visible only at deducing lungs from heart. On X-rays, these surfaces have the form of contours, the so-called edges of the heart: the right pointed and the left more dull. The average heart mass in men is about 300 grams, in females is 250 grams. The largest transverse heart size is 9-11 cm, anteroposterior size is 6-8 cm. The heart is 10-15 cm, the thickness of the atrium wall is 2-3 mm, the right ventricle - 4-6 mm and the left - 9-11 mm.
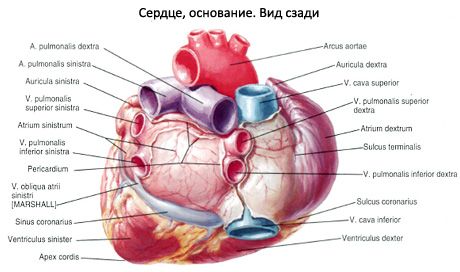
On the surface of the heart distinguish a transversely located, rather deep coronary furrow (sulcus coronarius), which is the boundary between the atria and ventricles. In this sulcus, the coronary arteries of the heart are located. In front, the furrow is covered by the pulmonary trunk and the ascending part of the aorta, behind which the atria are located. Above the coronal sulcus on the anterior surface of the heart there is a part of the right atrium with its right eye and the eye of the left atrium lying entirely behind the pulmonary trunk. Anterior interventricular sulcus (sulcus interventricularis anterior) is visible on the anterior chest-costal surface of the heart, to which the same artery and the large vein of the heart adjoin. On the back of the heart, the posterior interventricular furrow (sulcus interventricularis posterior) is visible with the artery and the middle vein of the heart lying in it.
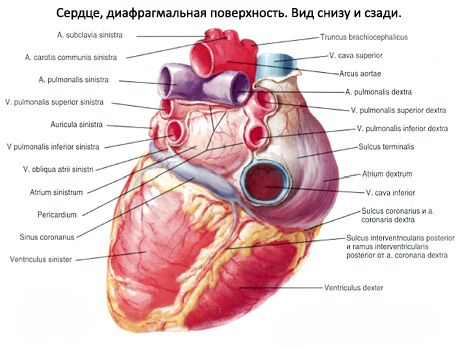
The longitudinal anterior interventricular furrow divides the sternocostal surface of the heart into a larger right side corresponding to the right ventricle, and a smaller left one belonging to the left ventricle. Most of the left ventricle forms the posterior surface of the heart. The posterior (inferior) interventricular furrow starts on the posterior surface of the heart at the site of the coronary sinus inflow into the right atrium, reaches the apex of the heart, where, with the help of the incisura apicis cordis, connects with the lower part of the anterior furrow.
The heart consists of 4 chambers: two atria and two ventricles - right and left. The atria take blood from the veins and push it into the ventricles. The ventricles eject blood into the arteries: the right - through the pulmonary trunk into the pulmonary arteries, and the left - into the aorta, from which numerous arteries move to the organs and walls of the body. The right half of the heart contains venous blood, the left half - the arterial blood. Between themselves, the right and left halves of the heart are not reported. Each atrium is connected to the corresponding ventricle through the atrioventricular opening (right and left), each aperture is closed with valvular valves. The pulmonary trunk and aorta at the beginning have semilunar valves.
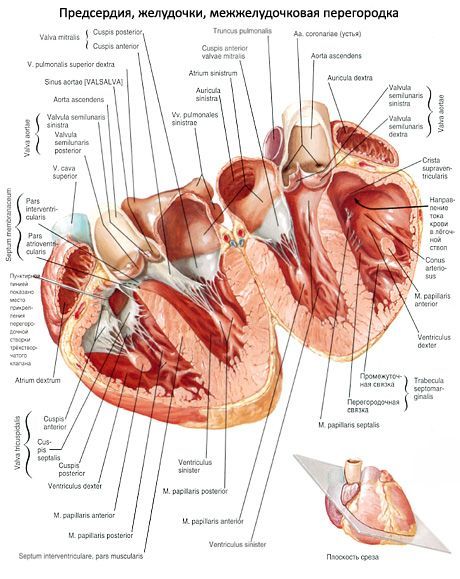
The right atrium (atrium dextrum), shaped like a cube, has a rather large additional cavity - the right ear (auricula dextra). From the left atrium it is separated by the interatrial septum (septum interatriale). On the septum, an oval recess is clearly seen-an oval fossa ovalis, closed by a thin membrane. This fossa, which is the remainder of an overgrown oval hole, which communicates the right and left atriums in the fetus, is limited by the edge of the oval fossa (hmbus fossae ovalis). The right atrium has an opening of the superior vena cava (ostium venae cavae superioris) and an opening of the inferior vena cava (ostium venae cavae inferioris).
Along the lower edge of the opening of the inferior vena cava there is a small inconsistent semilunar fold - the damper of the inferior vena cava (eustachian valve, valvula venae cavae inferioris). This damper in the embryo (fetus) directs the flow of blood from the right atrium to the left through the oval aperture. Sometimes the flapper of the inferior vena cava has a network structure: it consists of several connecting tendon threads. Between the holes of the hollow veins is seen a small intervenous tubercle (tuberculum tuberculum intervenosum), which is considered the remnant of a valve directing the blood flow from the superior vena cava to the right atrioventricular aperture in the embryo. The extended posterior portion of the right atrial cavity that receives both hollow veins is called the sinus venarum cavarum.
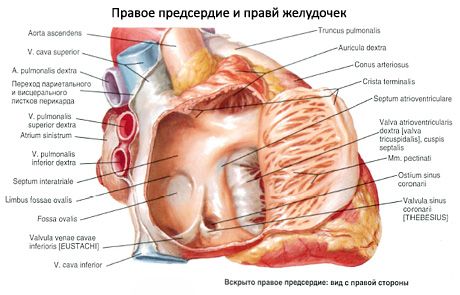
On the inner surface of the right abdomen and the adjacent section of the anterior wall of the right atrium, longitudinal muscular ridges projecting into the atrial cavity are visible - the comb muscles (mm.pectinati). At the top these cushions (muscles) end with a border crista (crista terminalis), which separates the venous sinus from the cavity of the right auricle (in the embryo there was a boundary between the common atrium and the venous sinus of the heart). The right atrium communicates with the ventricle through the right atrioventricular orifice (ostium atrioventriculare dextrum). Between this hole and the opening of the inferior vena cava there is an opening of the coronary sinus (ostium sinus coronarii). In its mouth, a thin sickle-shaped fold is visible - the damper of the coronary sinus (Valium sinus coronarii). Near the orifice of the coronary sinus, there are pinpoints of the smallest veins (foramina venarum minimalum) flowing into the right atrium independently; their number may be different. On the circumference of the aperture of the coronary sinus, the crural muscles are absent.
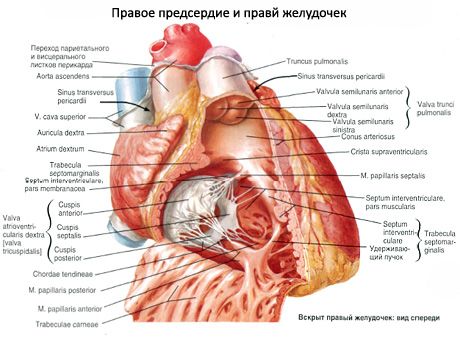
The right ventricle (ventnculus dexter) is located on the right and in front of the left ventricle, in shape resembles a triangular pyramid with a tip facing downward. The slightly convex medial (left) wall of the right ventricle forms the interventricular septum (septum interventriculare) separating the right ventricle from the left ventricle. Most of the septum is muscular (pars muscularis), and the smaller part located in the uppermost part is closer to the atria - membranaceous (pars membranacea).
The lower wall of the right ventricle, adjacent to the tendon center of the diaphragm, is flattened, the anterior wall convex anteriorly. In the upper, the widest part of the ventricle, there are two openings:
Right atrioventricular orifice
(ostium atrioventriculare dextrum), through which venous blood enters the ventricle from the right atrium, and in front -
Pulmonary trunk opening
(ostium trunci pulmonalis), through which the blood is directed to the pulmonary trunk. The site of the ventricle, from which the pulmonary trunk leaves, is called
Arterial cone
(conus arteriosus). Small
Supraventricular crest
(crista supraventricularis) delimits the arterial cone from the inside of the rest of the right ventricle.
The right atrioventricular aperture is closed by the right atrioventricular (tricuspid) valve (valva atrioventricularis dextra, s.valva tricuspidalis). The valve consists of three valves: front, rear and partitions. The base of the valves is firmly fused with a dense connective tissue ring located on the border of the atrium and ventricle. The valves of the atrioventricular valve are a triangular fold of the inner shell of the heart (endocardium), into which fibrous fibers from the connective tissue ring enter. Free edges of the valves, in appearance similar to thin tendon plates, face the cavity of the ventricle. In the anterior semicircle of the opening, the anterior valve cuspis (cuspis anterior) is reinforced, the posterolateral (cuspis posterior) on the posterolateral one and, finally, on the medial semicircle - the smallest of them is the medial septalis (cuspis septalis). When the atrium is contracted, the valves are pressed against the walls by a current of blood and do not interfere with its passage into the cavity of the ventricle. With contraction of the ventricles, the free edges of the valves close, but do not turn out into the atrium, since they are held on the side of the ventricle by tightly tight connective tissue strands - the chordae tendineae.
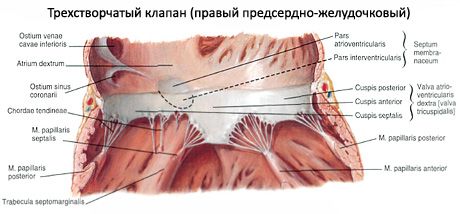
The inner surface of the right ventricle (with the exception of the arterial cone) is uneven, here we can see protruding ribs (trabeculae cdrneae) and cone-shaped papillary muscles (mm.papillares) protruding into the lumen of the ventricle. From the top of each of these muscles - the anterior (largest) and posterior (mm.papillares anterior and posterior) - most (10-12) tendon chords begin. Sometimes part of the chords originates from the fleshy trabeculae of the interventricular septum (the so-called septal papillary muscles). These chords are attached simultaneously to the free edges of two adjacent flaps, as well as to their surfaces facing the cavity of the ventricle. Therefore, when the atrioventricular valve is closed, the valves are set at the same level. Sometimes the chords are attached to the surfaces of the valves, facing the cavity of the ventricle.
Directly at the beginning of the pulmonary trunk, on its walls, is located the valve of the pulmonary trunk (valva trunci pulmonalis), consisting of three circular lobes: anterior, left and right (valvulae semilunaris anterior, dextra et sinistra). The convex (lower) surface of the flaps faces the cavity of the right ventricle, and the concave (upper) and free edge - into the lumen of the pulmonary trunk. The middle of the free edge of each of these dampers is thickened by the so-called nodulus valvulae semilunaris. Nodules contribute to more tightly closing the semilunar dampers when they close. Between the wall of the pulmonary trunk and each of the semilunar flaps there is a small pocket - a lunar (sine) semilunar flap (lunula valvulae semilunaris). During contraction of the ventricular musculature, the semilunar flaps (valves) are pressed against the wall of the pulmonary trunk by a current of blood and do not interfere with the passage of blood from the ventricle. When the muscles relax, when the pressure in the cavity of the ventricle falls, the return flow of blood fills the lunettes (sinuses) and opens the flaps: the edges of the flaps close and do not allow blood to pass into the cavity of the right ventricle.
The left atrium (atrium sinistrum), which has an irregular cuboidal shape, is delimited from the right atrium by a smooth atrial septum. The oval fossa located on the septum is more clearly expressed from the right atrium. The left atrium has 5 holes, four of them are located at the top and rear - these are the openings of the pulmonary veins (ostia venarum pulmonalium), two on each side. Pulmonary veins do not have valves. The fifth hole is the largest; this left atrioventricular orifice communicates the left atrium with the ventricle of the same name. The anterior wall of the left atrium has an anterior cone-shaped extension - the left eye (auricula sinistra). The inner wall of the left atrium is smooth, since the crest muscles are located only in the auricle.
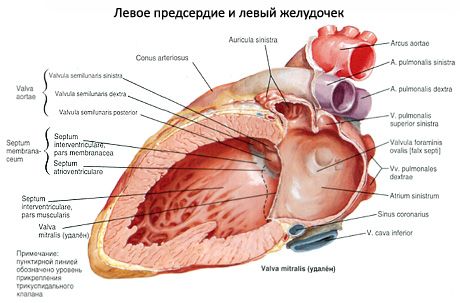
The left ventricle (ventriculus sinister) is conical, with a base turned upward. In the upper, widest part of the ventricle there are two openings. Behind and to the left is the left atrioventricular orifice (ostium atrioventriculare sinistrum), and to the right of it is the aortic opening (ostium aortae). In the left atrioventricular opening there is a left atrioventricular valve (mitral valve; valva atrioventricularis sinistra, s.valva mitralis).
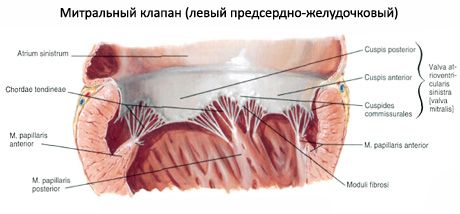
This valve consists of two folds of a triangular shape: the anterior cuspis anterior, which starts on the medial semicircle of the opening (near the interventricular septum), and the posterior cuspis posterior, smaller than the anterior one, starting from the lateral-posterior semicircle of the orifice.
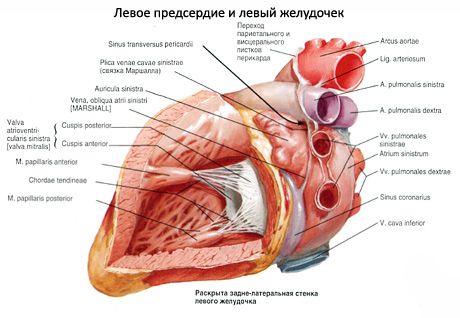
On the inner surface of the left ventricle (especially in the apex of the heart) are many large fleshy trabeculae and two papillary muscles - anterior and posterior (mm.papillares anterior and posterior). These muscles are located on the corresponding walls of the ventricle. From the tops of the muscles are the thick tendon chords that attach to the valves of the atrioventricular valve. Before entering the aortic opening, the surface of the ventricle is smooth. The valve of the aorta (valva aortae), located at its very beginning, consists of three semilunar flaps: the posterior (valvula semilunaris posterior), right (valvula semilunaris dextra) and left (valvula semilunaris sinistra). Between each flap and the wall of the aorta is a lunar (sine) semilunar flap (lunula valvulae semilunaris). The aortic flaps also have nodules-nodules of semilunar dampers, located in the middle of the free edges, the aortic flaps are larger than those of the pulmonary trunk.

Where does it hurt?
What's bothering you?
What do need to examine?
Last reviewed: 31.05.2018