Medical expert of the article

New publications
Diaphragm
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The diaphragm (diaphragma, sm phrenicus) is a movable muscular-tendinous partition between the thoracic and abdominal cavities. The diaphragm has a dome-shaped form due to the position of the internal organs and the difference in pressure in the thoracic and abdominal cavities. The convex side of the diaphragm is directed into the thoracic cavity, the concave side is directed downwards, into the abdominal cavity. The diaphragm is the main respiratory muscle and the most important organ of the abdominal press. The muscle bundles of the diaphragm are located along the periphery, have a tendon or muscle origin on the bony part of the lower ribs or costal cartilages surrounding the lower aperture of the thorax, on the posterior surface of the sternum and lumbar vertebrae. Converging upward, to the middle of the diaphragm, the muscle bundles pass into the tendon center (centrum tendineum). According to the origin, the lumbar, costal and sternal parts of the diaphragm are distinguished. The muscle bundles of the lumbar part (pars lumbalis) of the diaphragm originate on the anterior surface of the lumbar vertebrae, forming the right and left crura (crus dextrum et crus snistrum), as well as on the medial and lateral arcuate ligaments. The medial arcuate ligament (lig. arcuatum mediale) is stretched over the psoas major muscle between the lateral surface of the 1 lumbar vertebra and the apex of the transverse process of the 2 lumbar vertebra. The lateral arcuate ligament (lig. arcuatum laterale) passes transversely in front along the quadrate muscle of the lumbar spine and connects the apex of the transverse process of the 11 lumbar vertebra with the 12 rib.
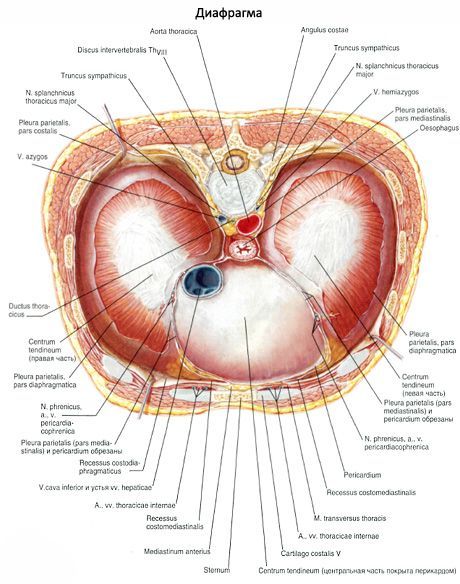
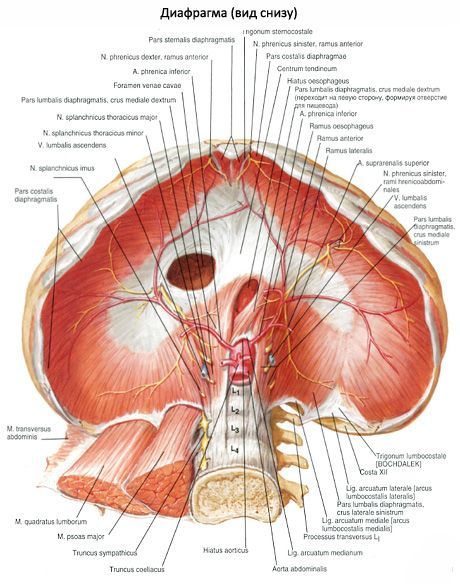
The right crus of the lumbar part of the diaphragm is more developed and begins on the anterior surface of the bodies of the 1st-4th lumbar vertebrae. The left crus originates on the first three lumbar vertebrae. The right and left crura of the diaphragm are intertwined below with the anterior longitudinal ligament of the spine. Above, the muscle bundles of these crura cross in front of the body of the 1st lumbar vertebra, limiting the aortic opening (hiatus aorticus). The aorta and the thoracic (lymphatic) duct pass through this opening. The edges of the aortic opening of the diaphragm are limited by bundles of fibrous fibers - this is the median arcuate ligament (lig. arcuatum medianum). When the muscle bundles of the crura of the diaphragm contract, this ligament protects the aorta from compression. Above and to the left of the aortic opening, the muscle bundles of the right and left crura of the diaphragm cross again and then diverge again, forming the esophageal opening (hidtus esophageus). Through this opening, the esophagus passes from the thoracic cavity to the abdominal cavity along with the vagus nerves. Between the muscle bundles of the right and left crura of the diaphragm pass the corresponding sympathetic trunk, the large and small splanchnic nerves, as well as the azygos vein (on the right) and the hemiazygos vein (on the left).
On each side between the lumbar and costal parts of the diaphragm there is a triangular area devoid of muscle fibers - the so-called lumbocostal triangle. Here the abdominal cavity is separated from the thoracic cavity only by thin plates of the intra-abdominal and intrathoracic fascia and serous membranes (peritoneum and pleura). Diaphragmatic hernias can form within this triangle.
The costal part (pars costalis) of the diaphragm begins on the inner surface of the six or seven lower ribs with separate muscle bundles that are wedged between the teeth of the transverse abdominal muscle.
The sternal part (pars sternalis) of the diaphragm is the narrowest and weakest, beginning on the back surface of the sternum.
Between the sternum and the costal parts of the diaphragm there are also triangular areas - sternocostal triangles, where, as noted, the thoracic fascia and abdominal cavity are separated from each other only by the intrathoracic and intra-abdominal fascia and serous membranes (pleura and peritoneum). Diaphragmatic hernias can also form here.
In the tendinous center of the diaphragm on the right there is an opening of the inferior vena cava (foramen venae cavae), through which this vein passes from the abdominal cavity into the thoracic cavity.
Function of the diaphragm: when the diaphragm contracts, its dome flattens, which leads to an increase in the chest cavity and a decrease in the abdominal cavity. When contracting simultaneously with the abdominal muscles, the diaphragm helps increase intra-abdominal pressure.
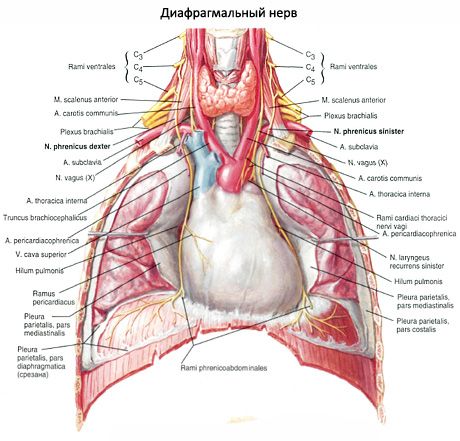
Innervation of the diaphragm: phrenic nerve (CIII-CV).
Blood supply of the diaphragm: superior and inferior phrenic arteries, posterior intercostal arteries (inferior).
 [
[ Diseases of the diaphragm
Damage to the diaphragm may occur with penetrating wounds to the chest and abdomen and with closed trauma, mainly with transport or catatrauma (falling from a height). Against the background of this injury, damage to the diaphragm is not always determined clinically, but in all cases of damage to the chest and abdomen, the diaphragm must be examined without fail, and it must be remembered that in 90-95% of cases of closed trauma, the left dome is damaged.
The most common pathology of the diaphragm is hernia. By localization, there are hernias of the dome of the diaphragm and the esophageal opening. Hernias of the cleft of the sympathetic trunk, inferior vena cava, intercostal nerve opening are extremely rare, but they do not give clinical signs and are more often an operational finding. By origin, hernias are divided into congenital and acquired, with a missed rupture. Clinical manifestations depend on the size of the hernial orifice and the tissues exiting through them into the chest cavity. With small sizes and prolapse of only the omentum, there may be no clinical manifestations of the hernia. The most acute are strangulated hernias of the dome of the diaphragm (hernias of the esophageal opening are never strangulated): a sudden attack of sharp pain in the epigastrium and chest, there may even be pain shock, palpitations, shortness of breath, vomiting, with strangulation of the intestine - signs of intestinal obstruction.
Sliding hernias of the dome of the diaphragm, most often of traumatic genesis, but can also form with underdevelopment of the diaphragm with localization in the area of the costal-lumbar triangle, usually on the left (Bogdalek's hernia), are accompanied by two syndromes: gastrointestinal and cardiorespiratory or their combination. Gastrointestinal syndrome is manifested by pain in the epigastrium and hypochondrium (usually on the left), chest, radiating upward - to the neck, arm, under the shoulder blade, emaciation, vomiting, sometimes with an admixture of blood, paradoxical dysphagia (solid food passes freely, and liquid is retained with subsequent vomiting). With prolapse into the chest cavity of the stomach, gastric bleeding may occur. Cardiorespiratory syndrome is manifested by cyanosis, shortness of breath, palpitations, which intensify after eating, physical exertion, when in a bent position. During a physical examination of the chest, there may be a change in percussion sound (tympanitis or dullness), weakening or absence of breathing in the lower lobes, intestinal noises, etc.
Hernias of the diaphragmatic opening are accompanied by pain and burning in the epigastrium and behind the breastbone, heartburn, belching, regurgitation, and sometimes dysphagia. The symptoms intensify after eating, in a horizontal position, and when bending the body. Sen's syndrome may develop: a combination of hernia of the esophageal opening, cholelithiasis, and diverticulitis of the colon. Rarely, relaxation of the diaphragm may occur: congenital, caused by underdevelopment of the muscles, and acquired, formed during inflammatory processes in the diaphragm, damage to the phrenic nerve. Accompanied by pain in the epigastrium and hypochondrium, shortness of breath, attacks of palpitations, a feeling of heaviness after eating, belching, nausea, constipation, weakness. Patients often have recurrent pneumonia of the lower lobes.
The examination complex should include: radiography of the lungs and abdomen, according to indications, a study is carried out with contrasting of the stomach and intestines with barium suspension and pneumoperitoneum (carefully, with a ready-made set for puncture of the pleural cavity or thoracentesis), laparoscopy or thoracoscopy with artificial pneumothorax, FGDS. The purpose of the study is not only to establish the pathology of the diaphragm, but also to conduct differential diagnostics with tumors of the esophagus, tumors and cysts in the liver, spleen.
Tactics: treatment is surgical, examination is complex, therefore the patient must be hospitalized in the thoracic department, less often in the abdominal surgery department.