Medical expert of the article

New publications
Coronary artery stenting: indications, technique of performance
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The number of cases of cardiovascular diseases is growing every year, and with it the statistics of fatal outcomes associated with heart failure, myocardial infarction and other heart pathologies are also adjusted. After all, we are talking about an organ that provides blood supply to the entire human body, and failures in its work necessarily affect the condition of other organs and systems. But it happens that the heart itself suffers from a lack of nutrients. And the reason for this can be a narrowing of the vessels that feed the organ. There are not so many effective methods to restore blood supply to the heart, improving the patency of the affected vessel, and one of them is coronary stenting.
Pathogenesis of arterial stenosis
It is not for nothing that the heart is compared to a pump, because thanks to it, blood is able to move through the vessels. Rhythmic contractions of the heart muscle ensure the movement of physiological fluid, which contains substances and oxygen necessary for the nutrition and respiration of organs, and then everything depends on the condition of the vessels.
Blood vessels are hollow organs, limited by a strong and elastic wall. Normally, nothing should prevent blood from moving at the speed set by the heart inside the arteries, veins and small capillaries. But narrowing of the lumen of the vessels, the formation of blood clots and cholesterol plaques on their walls is an obstacle to the movement of physiological fluid.
Such obstacles slow down the blood flow, and this affects the organs that were supplied with blood by the stenotic vessel, because they no longer receive enough nutrients and oxygen necessary for normal functioning.
Comparing the human heart to a pump, one can understand that this organ also needs energy to perform its important function. And the heart receives it from blood, providing nutrition and respiration to the myocardium. Blood is supplied to the heart by a network of coronary arteries, any changes in the condition of which, including vascular stenosis, negatively affect the blood supply and performance of the heart, causing myocardial ischemia, heart failure, and infarction.
What are the reasons for the narrowing of the lumen of the coronary arteries? Doctors believe that the most common cause of this condition is atherosclerosis of the vessels, i.e. the formation of cholesterol deposits on the inner layer of their walls, which gradually increase, leaving less and less free space for blood.
Other common causes include blockage of the coronary arteries by blood clots (thrombosis) or spasm of the heart vessels due to gastrointestinal diseases, infectious and allergic pathologies, rheumatoid and syphilitic lesions.
Risk factors for such problems include physical inactivity (sedentary lifestyle), excess weight (obesity), bad habits (for example, smoking), age over 50, frequent stress, taking certain medications, hereditary predisposition and national characteristics.
The occurrence of foci of pathological narrowing of blood vessels, in the treatment of which coronary stenting is practiced, can be caused by some diseases, in addition to those described above. These include metabolic diseases, endocrine diseases, blood and vascular diseases (for example, vasculitis), intoxication of the body, arterial hypertension, anemia, congenital malformations of the heart and blood vessels (for example, slowly progressing heart disease with a predominance of stenosis).
Since our heart is divided into two parts, to the ventricles of which blood vessels are supplied, doctors distinguish between stenosis of the left and right coronary artery trunk. In the first case, almost all human organs are affected, because the left ventricle of the heart supplies blood to the systemic circulation. The most common cause of stenosis of the left artery of the heart is considered to be atherosclerosis, in which a gradual decrease in the lumen of the vessel occurs.
If we are talking about the fact that the arterial cavity occupies less than 30% of the original lumen, we speak of critical stenosis, which is fraught with cardiac arrest or the development of myocardial infarction.
With stenosis of the right cardiac artery, the organ itself suffers first and foremost, since the blood supply to the sinus node is disrupted, which leads to disturbances in the heart rhythm.
In some cases, doctors diagnose a simultaneous narrowing of the right and left coronary artery (the so-called tandem stenosis). If, with unilateral stenosis, the compensatory mechanism was triggered and the undamaged ventricle took on most of the work, then with tandem narrowing this is impossible. In this case, only surgical treatment can save a person's life, a more gentle option of which is stenting.
The concept of treating vascular stenosis by widening the stenotic section of arteries using a special frame was proposed more than half a century ago by American radiologist Charles Dotter, but the first successful operation was performed only a year after his death. But the evidence base for the effectiveness of stenting was obtained only 7 years after the first experience. Now this method helps save the lives of many patients without resorting to traumatic abdominal surgery.
Indications for the procedure
Usually, with heart disease, patients come to the doctor complaining of pain behind the breastbone. If this symptom intensifies with physical exertion, the specialist may suspect a narrowing of the coronary arteries, which results in a disruption of the blood supply to the heart. At the same time, the smaller the lumen of the vessel, the more often a person will experience discomfort in the chest and the more pronounced the pain will be.
The most unpleasant thing is that the appearance of the first signs of stenosis is not evidence of the onset of the disease, which could have been latent for a long time. Discomfort during physical exertion occurs when the lumen of the vessel becomes significantly smaller than normal and the myocardium begins to experience oxygen starvation at the moment when it is required to work actively.
Symptoms that are also worth paying attention to are shortness of breath and attacks of angina (a symptom complex that includes: rapid heartbeat, chest pain, hyperhidrosis, nausea, a feeling of lack of oxygen, dizziness). All of these signs may indicate coronary stenosis.
It should be said that this pathology, regardless of its causes, has a not very good prognosis. If we are talking about atherosclerosis of the coronary vessels, then conservative treatment with statins, which correct the level of cholesterol in the blood, and drugs that reduce the myocardium's need for oxygen, is prescribed only at the initial stages of the disease, when a person actually does not complain of anything. When symptoms of stenosis appear, traditional treatment may not give results, and then doctors resort to surgical intervention.
Severe narrowing of the vessels causes angina attacks, and the more vessels are affected, the more obvious the disease becomes. Angina attacks can usually be stopped with medications, but if there is no improvement, then there is no other way out than to resort to coronary bypass surgery or less traumatic stenting.
Coronary artery bypass grafting is the creation of a bypass for blood flow if a blood vessel narrows so much that it can no longer cover the needs of the myocardium. This operation requires opening the sternum and all manipulations are performed on an open heart, which is considered very dangerous.
At the same time, if a safer minimally invasive operation called stenting, which does not require large incisions and a long recovery period, is used, it is not surprising that doctors have been resorting to the latter much more often lately.
Moreover, stenting can be successfully performed both in the case of a single stenosis and in the case of narrowing of several arteries.
If the vessels are narrowed by more than 70% or the blood flow is completely blocked (occluded), there is a high risk of developing acute myocardial infarction. If the symptoms indicate a pre-infarction condition, and the patient's examination indicates acute tissue hypoxia associated with impaired blood flow in the coronary vessels, the doctor may refer the patient to an operation to restore arterial patency, one of which is arterial stenting.
Coronary stenting surgery can also be performed during treatment of a heart attack or in the post-infarction period, when the person has received emergency care and the heart's activity has been restored, i.e. the patient's condition can be called stable.
Stenting after a heart attack is prescribed in the first hours after the attack (maximum 6 hours), otherwise such an operation will not bring any particular benefit. It is best if no more than 2 hours pass from the appearance of the first symptoms of a heart attack to the beginning of the surgical intervention. Such treatment helps to prevent the attack itself and reduce the area of ischemic necrosis of myocardial tissue, which will allow for a quicker recovery and reduce the risk of relapse of the disease.
Restoring vascular patency within 2-6 hours after a heart attack will only prevent a recurrence. But this is also important, because each subsequent attack is more severe and can end the patient's life at any moment. In addition, aortocoronary stenting helps restore normal breathing and nutrition of the heart muscle, which gives it the strength to recover faster after damage, because normal blood supply to tissues accelerates their regeneration.
Stenting of vessels in atherosclerosis can be performed both as a preventive measure against heart failure and myocardial ischemia, and for therapeutic purposes. Thus, in chronic forms of coronary heart disease, when the vessels are half blocked by cholesterol deposits, stenting can help preserve healthy heart tissue and prolong the patient's life.
Coronary stenting is also prescribed in cases of frequently recurring angina attacks with the slightest physical exertion, not to mention the obstruction of the coronary vessels. But it is important to understand that severe cases of ischemic heart disease (unstable or decompensated angina) cannot be cured in this way. The operation only alleviates the patient's condition and improves the prognosis of the disease.
 [
[ Preparation
Any operation, even the least traumatic, is considered a serious intervention in the body, and what can we say about heart operations, which are considered potentially dangerous to human life. It is clear that the cardiac surgeon must have good reasons for performing such manipulations. The patient's desire alone is not enough.
First, the patient should be examined by a cardiologist. After a physical examination, study of the patient's medical history and complaints, auscultation (listening) to the heart, measurement of heart rate and blood pressure, if coronary artery stenosis is suspected, the doctor may prescribe the following tests:
- general and biochemical blood analysis,
- ECG and EchoCG are studies of the activity of the heart by recording the electrical impulses passing through it (at rest and under load),
- X-ray or ultrasound of the chest, which allows recording the location of the heart and blood vessels, their size and changes in shape,
But the most informative in this case is the study called coronary angiography (coronary angiography), which involves examining the lumen of the vessels that feed the myocardium of the heart, with the determination of the severity of coronary heart disease. It is this diagnostic study that allows us to assess the feasibility of performing heart surgery and choose the appropriate technique, as well as determine the areas where stents will be installed.
If the patient's condition allows, the doctor prescribes a planned operation and explains how to properly prepare for it. Preparation for the operation involves:
- Refusal to take certain medications:
- non-steroidal anti-inflammatory drugs and anticoagulants (warfarin, etc.) that affect blood clotting are not recommended to be taken within a week before surgery (or at least a couple of days),
- a couple of days before the operation, you will need to stop taking sugar-lowering medications or change the time of their intake (these issues should be discussed with an endocrinologist),
- In case of cardiac ischemia and cardiac failure, patients should regularly take aspirin-based medications, there is no need to change their regimen. Moreover, 3 days before the operation, the patient may be prescribed antithrombotic drugs (for example, clopidogrel). Less often, it is administered in high doses directly in the preoperative room, which is fraught with stomach problems.
- Eating is not prohibited the night before the operation, but it should be a light dinner. After 12 midnight, complete abstinence from food and liquids is required. The operation is performed on an empty stomach.
- Before the coronary stenting procedure, it is advisable to take a shower using antibacterial agents and shave the hair in the groin area (usually the stent is inserted into the femoral artery in the pelvic area, since access through the groin area is considered more reliable and safer than puncturing a large artery in the arm).
In severe cases of acute coronary insufficiency and myocardial infarction, when there is no time for a full examination and preparation for surgery, the patient simply undergoes the necessary tests and an emergency operation is initiated, during which the cardiac surgeon makes a decision on stenting or bypass surgery of the vessels.
Technique coronary artery stenting
The most important diagnostic method, which allows not only to detect the fact of stenosis, but also to determine the exact size and location of the affected area, is coronography. This is a type of X-ray examination of blood vessels using contrast, which allows to visualize any changes in the structure of the heart arteries. Pictures are taken from different angles and archived on a computer screen, so that it is easier for the doctor to navigate during the operation, because the human eye is not able to see what is happening inside the body.
Coronary stenting, unlike bypass surgery, is performed without large incisions in body tissues and involves the percutaneous insertion of a thin tube through which all the necessary instruments are delivered to the site of the operation (as in endoscopy). It turns out that the cardiac surgeon works blindly and cannot see the result of his work. That is why such operations are performed under the control of X-ray or ultrasound.
Ideally, in routine surgeries, diagnostic testing should be performed the day before the procedure, but in severe cases requiring emergency care, coronary angiography and coronary stenting can be performed simultaneously. This way, doctors do not have to waste precious time on diagnostics and at the same time they have the opportunity to actively monitor the progress of the operation.
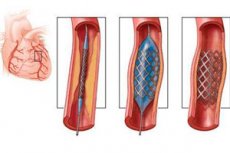
The essence of the coronary stenting operation is to expand the stenotic vessel using a special flexible metal frame resembling a mesh. The stent is inserted in a folded form, but at the site of the narrowing of the artery it expands and then remains straightened inside the vessel, preventing further narrowing of the lumen.
To insert a stent, a puncture must be made in a large artery running in the groin or arm. Pain relief is provided by local anesthesia, but sedatives (the patient remains conscious and can see the surgeon's manipulations, so such preparation is not a problem) and painkillers may also be administered. First, the puncture site is treated with an antiseptic, then an anesthetic is administered. Novocaine or lidocaine are usually used.
During the operation, the heart's work is constantly monitored using an ECG, for which electrodes are placed on the patient's upper and lower limbs.
Most often, the puncture is made in the femoral artery, which is more convenient and allows you to avoid various complications. At the puncture site, a plastic tube called an introducer is inserted into the artery, which will be a kind of tunnel for feeding instruments to the site of the vessel lesion. Another flexible tube (catheter) is inserted inside the introducer, which is advanced to the site of stenosis, and a folded stent is fed through this tube.
When performing coronary angiography and stenting simultaneously, iodine preparations are injected into the catheter before the stent is inserted, which are used as a contrast agent that is captured by X-rays. The information is displayed on a computer monitor. This allows the catheter to be controlled and brought precisely to the site of the vessel stenosis.
After the catheter is installed, a stent is inserted into it. A deflated special balloon used for angioplasty is first placed inside the stent. Even before the development of stenting, the expansion of stenotic vessels was carried out using balloon angioplasty, when a deflated balloon was inserted into the vessel, and then the patency of the artery was restored by inflating it. True, such an operation was usually effective for six months, after which restenosis was diagnosed, i.e. repeated narrowing of the lumen of the vessel.
Coronary angioplasty with stenting reduces the risk of such complications, because the person may not survive the repeated operations required in this case. The deflated balloon is placed inside the stent. Having advanced it to the site of the narrowing of the vessel, the balloon is inflated, and the stent is straightened accordingly, which, after the balloon and tubes are removed, remains inside the artery, preventing it from narrowing.
During the procedure, the patient can communicate with the doctor, follow his instructions and report any discomfort. Usually, chest discomfort appears when approaching the stenotic area, which is a normal variant. When the balloon begins to inflate and the stent is pressed into the vessel walls, the patient may experience pain associated with impaired blood flow (the same attack of angina). You can slightly reduce the discomfort by holding your breath, which the doctor may also ask you to do.
Currently, doctors successfully perform stenting of the left and right coronary arteries, as well as treatment of tandems and multiple stenoses. Moreover, the effectiveness of such operations is much higher than that of balloon angioplasty or aortocoronary bypass. The least complications occur when using drug-eluting stents.
Contraindications to the procedure
Coronary stenting is an operation that helps save a person's life in case of life-threatening pathologies. And since there can be no consequences worse than death, there are no absolute contraindications to the procedure. Especially if stenting is indicated for myocardial infarction. Serious problems can only arise if there is no possibility to carry out antiplatelet treatment, because the risk of blood clots after the operation increases.
The procedure has some relative contraindications, which are risk factors for complications after or during surgery. However, some disorders may be temporary, and after their successful treatment, surgery becomes possible. Such disorders include:
- feverish state, high body temperature,
- infectious diseases in the active stage,
- gastrointestinal bleeding,
- acute form of stroke,
- a severe neuropsychiatric condition in which contact between the patient and the doctor is impossible,
- cardiac glycoside poisoning,
- severe anemia, etc.
In this case, it is recommended to postpone the date of the operation if possible until the patient's condition stabilizes. But there is another part of the diseases that can affect the outcome of the operation:
- severe acute and chronic renal failure,
- respiratory failure,
- blood pathologies in which its coagulability is impaired,
- intolerance to the contrast used for coronography,
- arterial hypertension that cannot be corrected,
- severe electrolyte imbalances,
- heart failure in the decompensation stage,
- diabetes mellitus,
- pulmonary edema,
- concomitant disease that may have complications after coronary angiography,
- inflammation of the inner lining of the heart and its valves (endocarditis).
In these cases, the decision to perform the operation is made by the attending physician, who makes certain adjustments to the procedure taking into account possible complications (for example, the study of the vessels is carried out without contrast or other substances with similar properties are used instead of iodine).
Another obstacle to the operation is the patient's unwillingness to undergo further treatment, if necessary. After all, stenting of the heart vessels is a serious intervention that requires the surgeon to expend energy, nerves, and strength, so if the patient is not currently in mortal danger and does not want to worry about his future, should the doctor worry about this? After all, at the same time, the surgeon can provide assistance to a patient who seriously needs it.
Care after the procedure
After the operation, which usually takes about 1-2 hours, the patient is transferred to intensive care. The introducer remains in the artery for some time. For several hours after the procedure, the patient's blood counts, blood pressure, heart function are constantly monitored, and the site of catheter insertion is monitored. If everything is normal, the tube is removed, and a pressure bandage is applied to the puncture site. No stitches are needed, the small wound usually heals within a few days.
The patient can eat and drink immediately after the operation. This will not affect his condition in any way. Coronography during coronary stenting involves the introduction of a contrast agent. To quickly remove it from the body, it is recommended to drink mineral water in a volume of at least 1 liter.
To insert a stent, which will subsequently maintain sufficient lumen of the vessel, there is no need to open the sternum or make large incisions on the body that heal over a long period of time, limiting the patient's physical activity. A small puncture does not impose such restrictions, and yet on the day of the operation the patient must not bend his leg.
The next day, after the patient is transferred to a regular ward, he will be allowed to walk and take care of himself. But for some time he will have to refrain from active physical activity that involves a lot of strain on the legs and blood vessels.
Usually, after a couple of days, if the patient feels normal, they are discharged home. Recovery of the body is different for everyone. For some, a few days are enough, while for others, life gets better after 3-4 months. During this period, you should avoid overwork, hypothermia or overheating of the body, stick to a balanced diet (preferably fractional), try to worry less and avoid stressful situations.
If the patient was prescribed any medications before the operation, the doctor may cancel this prescription, leaving only the drugs that reduce blood viscosity and prevent the formation of blood clots. Then the patient will have to regularly visit a cardiologist with the necessary examinations: cardiogram, stress test, tests, etc. How the body will recover after the operation largely depends on the patient's compliance with the doctor's recommendations.