Medical expert of the article

New publications
Cornelia de Lange syndrome
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

This is a rare congenital pathology, characterized by the fact that the child is born with immediately noticeable multiple deviations from the norm. Subsequently, the infant also shows signs of mental retardation.
The first to describe the syndrome as an independent disease was the German doctor W. Brachman at the beginning of the 20th century. Somewhat later, a pediatrician from the Netherlands, Cornelia de Lange (de Lange), treated two small patients suffering from this disease and described it in detail based on observations. This pathology can also be called Brachman-de Lange syndrome or degenerative nanism (dwarfism) of the "Amsterdam" type, since three children with this diagnosis lived in the capital of the Netherlands.
Epidemiology
Epidemiology of Cornelia de Lange syndrome: it is rare, newborns with such pathology appear in approximately one case out of 10-30 thousand births, other sources cite even lower rates - one case out of 100 thousand. In total, at the moment, more than 400 cases of this disease are known in different countries, boys and girls among them are approximately equal.
Causes Cornelia de Lange syndrome
The etiology and pathogenesis of this syndrome have not yet been established and are under study. There are suggestions that the disease is hereditary and may be caused by various genetic abnormalities, although the gene responsible for intrauterine developmental disorders and the type of its transmission have not yet been determined (a hypothesis has been put forward about mutations in the BIPBL gene (HSA 5p13.1), encoding delangin).
Mutations in genes encoding two other proteins involved in sister chromatid cohesion, SMC1A and SMC3, have been reported in 5% and 1% of patients with Cornelia de Lange syndrome, respectively.
Analysis of samples of this disease suggests that the inheritance of the mutant gene in this case is not characterized by its primitive transmission. It is likely that over time, improved cytogenetic research will be able to identify pathology at the chromosomal level.
Most of the studied cases of Cornelia de Lange syndrome are solitary, and usually there were no changes in the chromosomal set of patients, although anomalies were occasionally detected - fragmentary trisomy of the long arm of chromosome 3 and chromosome 1 was most common, and chromosome 9 had a ring shape.
There are also known cases of the disease occurring in members of the same family, the analysis of which suggests an autosomal recessive mode of transmission of the gene that provokes this pathology.
However, in the manifestations of the syndrome in members of the same family, there is no complete or partial underdevelopment of the limbs, as in isolated cases. Based on this, a hypothesis has been put forward about differences in the causes of familial and isolated cases of Cornelia de Lange syndrome.
The influence of paternal age on the frequency of having a child with this disease is more than controversial, so it is still unclear whether this syndrome can be caused by single autosomal dominant genotype transformations.
Risk factors
Risk factors include a family history of this syndrome, since in this case (if the assumption about the recessive mode of gene transmission is correct) the probability of the next child having a pathology is 25%. The probability of the situation repeating itself in single episodes, in the absence of chromosomal mutations in the parents, is theoretically 2%.
It is assumed that chromosome transformations occur as a result of severe infections and intoxications suffered by the expectant mother in the first three months of pregnancy, side effects of chemotherapeutic drugs and some physiotherapeutic procedures. Gene mutations can be promoted by endocrine diseases of the mother, radiation, the advanced age of the child's father or the mother's age over 35 years, as well as when the mother and father are blood relatives.
 [ 8 ]
[ 8 ]
Symptoms Cornelia de Lange syndrome
It is characterized by numerous developmental defects that are usually noticeable, although sometimes only detected through diagnostic procedures.
The main symptoms of Cornelia de Lange syndrome are:
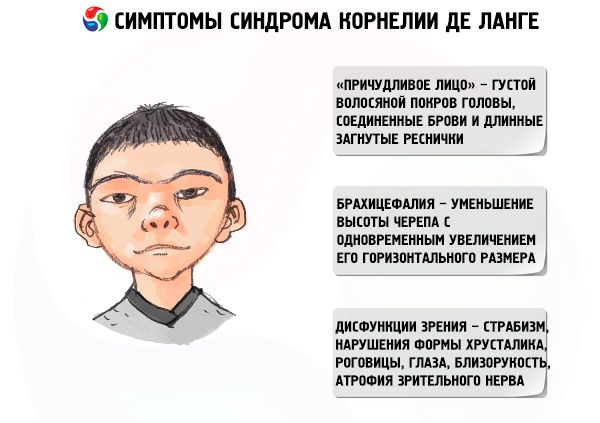
- "bizarre face" - thick hair on the head for a newborn, connected eyebrows and long curved eyelashes, deformed ears and a small nose with nostrils open in front, the space from the upper lip to the tip of the nose is abnormally large, a thin red border of the upper lip, the corners of the lips are lowered;
- microcephaly of the brain;
- brachycephaly – a decrease in the height of the skull with a simultaneous increase in its horizontal size;
- pathologies of the oral cavity and nasopharynx - atresia of the choanae, arched palate with a cleft, failures in the process of eruption of milk teeth.
- visual dysfunctions – strabismus, abnormalities of the shape of the lens, cornea, eye, myopia, optic nerve atrophy;
- shortened limbs, ectrodactyly, oligodactyly and other limb anomalies;
- marbled leather;
- anomalies of the nipples and genitals;
- hyperhairy body;
- episodic convulsive readiness, hypotonia, hypertonia of muscles;
- dwarfism;
- mental retardation of varying degrees – from minor deviations from the norm (rare) to oligophrenia and imbecility in most cases.
The first signs of the disease are visually noticeable in newborns. In addition to external features, the child's low birth weight is noteworthy - it is 2/3 of the weight of a healthy child born at a similar stage of pregnancy. Newborns have problems with feeding and breathing. From an early age, they suffer from frequent infectious and inflammatory diseases of the respiratory tract due to the specific structure of the nasopharynx.
Autopsies of deceased patients reveal various defects of the brain (underdevelopment of the inferior frontal gyrus, enlargement of the ventricles, dysplasia and hypoplasia of the gyri), histology often shows pronounced transverse striation of neurons in the external granular layer of the cerebral cortex and a disorder in the topography of cerebellar neurons.
In more than half of all cases, Amsterdam dwarfism is accompanied by defects in the structure of the heart (aortopulmonary window, unclosed septum separating both the atria and ventricles, often in combination with vascular disorders, tetralogy of Fallot), defects in the structure of the gastrointestinal tract (mainly intestinal rotation disorders), genitourinary system (cystic kidney formations, single and multiple, sometimes horseshoe kidney and hydronephrotic changes, cryptorchidism, bicornuate uterus).
This disease, characterized by multiple developmental defects, is essentially an as-yet undisclosed genetic anomaly that begins during the formation of the embryo. The process, triggered by the pathogenic factor, continues and worsens later, after the birth of the child. The stages of the disease go hand in hand with biochemical pathologies in the brain neurons throughout all stages of the body's maturation. Such lesions are accompanied by mental retardation, and the multiple behavioral and external deviations present in the patient do not yet indicate the end of the process in the intrauterine period.
[ 9 ]
Forms
Modern psychiatry classifies the following types of this syndrome:
- Classical (first), when all symptoms are clearly manifested: specific appearance, multiple developmental defects, noticeable mental retardation.
- The erased type (second), in which the same defects of the face and body are present, but there are no anomalies of the internal organs that are incompatible with life, and motor, mental and intellectual impairments are weakly expressed.
According to parents' observations, children with this disease do not ask to go to the toilet at any age, are prone to irritability, and constantly commit senseless acts that are not typical for healthy children: they tear or eat paper, break everything that catches their eye, and move in circles. This brings them peace.
Complications and consequences
The consequences and complications of having de Lange syndrome are unfavorable, people are very dependent on others, they are unable to live independently without constant help, in classic cases death from some pathology of the development of internal organs is possible even in infancy.
[ 13 ]
Diagnostics Cornelia de Lange syndrome
At the current stage of diagnostics development, it is impossible to detect the presence of this pathology in the embryo. A risk factor for the development of the syndrome is the absence of plasma protein-A (PAPP-A) in the serum of a pregnant woman, which is normally produced in large quantities during pregnancy. However, it is impossible to accurately diagnose the presence of the disease in the embryo based on the results of this test alone, since in 5% of normal pregnancies a false positive result is observed, and chromosomal abnormalities in the fetus are detected only in 2-3% of cases of decreased levels of this protein.
Amsterdam dwarfism is determined in newborns by characteristic external signs.
Multiple defects and anomalies incompatible with life must be diagnosed in a timely manner so that the surgical intervention necessary to save life can be carried out.
Instrumental diagnostics are carried out using magnetic resonance imaging, ultrasound and X-ray examination, rhinoscopy and other modern diagnostic methods as necessary.
The patient undergoes both standard clinical and cytogenetic tests.
Diagnostics is carried out in two stages: clinical examination of the newborn's condition, corresponding to modern methods, and differential diagnostics of a specific genetic pathology. It is based on the differentiation of such lesions with the most typical symptomatic manifestations in this syndrome.
The diagnosis of de Lange syndrome is sometimes controversial, since there are children with mental retardation and a small number of defects - signs of this disease. Since there is no indisputable biological way to confirm the diagnosis, it is impossible to determine with certainty whether these episodes relate to this syndrome.
[ 14 ]
Who to contact?
Treatment Cornelia de Lange syndrome
There are no specific treatment methods for this condition. Infants undergo surgery when necessary to correct developmental defects that are incompatible with life.
During the rest of life, treatment procedures are prescribed - physiotherapy, psychotherapy, massage, wearing glasses, etc. according to symptoms. Drug treatment - nootropics, anabolics, vitamins, anticonvulsants and sedatives.
Prevention
It is difficult to prevent a syndrome whose causes have not been precisely determined.
However, taking into account the known sources of gene mutations, the following can be recommended as preventive measures:
- preventing conception of children from a mother and father who are blood relatives;
- be carefully examined in case of the possibility of late motherhood and fatherhood;
- Pregnant women should avoid contracting viral infections, especially in the first trimester, and if infected, use drug therapy only as prescribed by a doctor.
Women and men with a family history of Cornelia de Lange syndrome should definitely visit a medical genetic consultation. During pregnancy, women should definitely be tested for the presence of plasma protein-A.
Forecast
The life expectancy of people with this disease depends on many factors, the main ones being the severity of defects in vital organs, their early diagnosis and the quality of surgical interventions to eliminate them.
In case of developmental anomalies incompatible with life, the child dies in the first week of life. If they are insignificant or are surgically eliminated in a timely manner, a patient with Cornelia de Lange syndrome can live quite a long time. Prognosis is complicated by the lack of resistance of the body of patients with this syndrome to ordinary infections that are not dangerous for ordinary people, such as viral infections, which also cause the early death of such patients.
The average life expectancy is approximately 12-13 years; according to some sources, patients with a latent form of the disease or successful operations to correct developmental defects sometimes lived to their fifth or sixth decade.
[ 18 ]