Medical expert of the article

New publications
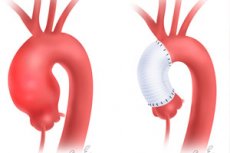
Aneurysm of the ascending aortic arch
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Aneurysm of the ascending aortic arch is diagnosed by pathologic local expansion and bulging of the wall of the arch-shaped part of the aorta (the main artery of the great circle of blood circulation), going upward from the left ventricle of the heart and enclosed in the cavity of the outer shell of the heart (pericardium). [1]
Epidemiology
According to statistics, thoracic aortic aneurysms account for almost one third of all cases of localized bulging of the wall of this vessel; about 60% of all thoracic aneurysms occur in the ascending aorta, and its prevalence is 8-10 people out of 100 thousand. They are most often diagnosed between 50 and 60 years of age.
Up to 80% of patients with Marfan syndrome have an aneurysm or dilatation in the region of the ascending aorta and its arch. However, even in the absence of the syndrome, at least 20% of thoracic aortic aneurysms are considered to be genetically determined. [2]
Causes of the ascending aortic arch aneurysms
Aneurysms of the ascending aorta (extending from the sinotubular junction to the origin of the brachiocephalic artery) and its ascending arch (which runs anterior to the trachea and to the left of the trachea and esophagus, contains the origin of the brachiocephalic artery, and branches into the arteries of the head and neck) are a subtype of thoracic aortic aneurysm.
Regardless of localization, the main causes of aneurysm formation are weakening of the vascular wall with its stretching and widening of the vessel lumen (dilatation), which can increase the diameter of the artery by 50% or even one and a half to two times (up to 5 cm or more).
Aneurysm formation can lead to:
- Atherosclerosis;
- Inflammation of the aorta - aortitis, including untreated syphilis;
- Granulomatous inflammation of the aorta - arteritis or takayasu syndrome, and Horton's disease or giant cell arteritis;
- Systemic connective tissue diseases of autoimmune origin (systemic lupus erythematosus, behçet's disease ) and congenital diseases that can affect the connective tissue of blood vessel walls - genetic arteriopathies in Marfan, Loeys-Dietz, Ehlers-Danlos, Ulrich-Nunan syndromes.
Infectious etiology of aneurysm of this localization is also possible, due to bacteremia: the presence in the blood of such anaerobic Gram-negative bacteria as Salmonella spp., Staphylococcus spp. And Clostridium spp.
Aortic arch aneurysms can be fusiform (spindle-shaped) or saccular (pouch-shaped). Fusioform ones are more often caused by connective tissue abnormalities, in particular, in genetic diseases. Sometimes such aneurysms are calcified. Aortic arch sac aneurysm, which affects a limited part of the aortic circumference, is associated with atherosclerosis in most patients. [3]
For more information see. - aneurysms: causes, symptoms, diagnosis, treatment
Risk factors
According to experts, the aorta itself is predisposed to the development of aneurysms, which is explained by the shape of this vessel and the presence of aortic sinuses - sinuses of Valsalva, the walls of which do not have a middle layer (tunica media) and therefore thinner than the wall of the artery. [4]
And risk factors for aneurysm formation of the ascending aortic arch include:
- Age over 55-60 years old;
- Smoking;
- Abdominal obesity and lipid metabolism-related hypercholesterolemia (elevated blood cholesterol);
- Arterial hypertension and cardiovascular disease;
- Family history of aortic aneurysms, i.e. Genetic predisposition to aortic aneurysm disease. It is believed that the closest relatives of a person with an aortic aneurysm have at least a 10-fold increased risk of developing it;
- Connective tissue dysplasia;
- Heart defect or aortic valve defect (absence of its third leaflet);
- Presence of aortic arch anomaly, in particular, malposition of the right common carotid artery; subclavian artery aberration; bullous aortic arch - common branch of the brachiocephalic arteries (subclavian, left vertebral and common carotid arteries).
Pathogenesis
Studying the mechanism of pathological processes occurring in the vascular wall and leading to its weakening and bulging, the researchers came to the conclusion: structural changes under the influence of causative factors first affect the inner (tunica intima) and middle (tunica media) shells or layers of the wall, and then the outer shell - adventitia.
Thus, the intima, consisting of a layer of endothelium (endothelial cells), which is supported by the connective subintima (with a basal membrane between the two tissue types), begins to be damaged due to a reaction to subendothelially acting inflammatory mediators: a range of cytokines, endothelial adhesion molecules, and growth factors. For example, it activates the degradation of extracellular matrix by increasing the production of plasminogen activators and the release of matrix metalloproteinases (MMPs) - transforming growth factor beta-1 (TGF-B1).
Over time, the media, consisting of fibers (elastin and collagen), smooth muscle cells and connective tissue matrix, becomes involved in the process. This sheath makes up about 80% of the thickness of the vessel wall (including the aorta), and it is the proteolytic degradation of its structural components - destruction of elastic fibrils, deposition of glycosaminoglycans in the matrix and thinning of the wall - that is associated with the pathogenesis of aneurysm development.
In addition, in atherosclerosis and arterial hypertension in old age, stretching, local expansion of the intravascular lumen and bulging of part of the wall under the action of increased blood pressure in the aorta during systole occurs due to penetrating ulceration of the vessel wall. It, in turn, is caused by the formation of atherosclerotic plaques - with loss of nuclei of medial matrix cells and degeneration of elastic laminae of basal membranes of vascular sheaths. [5]
Symptoms of the ascending aortic arch aneurysms
Minor aneurysms of the ascending aortic arch are mostly asymptomatic, and the first signs appear when the bulging part of the vessel wall enlarges.
Symptoms usually occur with a larger aneurysm and may manifest as a result of compression of surrounding structures (trachea, bronchi, esophagus) in the form of: hoarseness of voice; wheezing and/or coughing; shortness of breath; dysphagia (difficulty swallowing); chest or upper back pain. [6]
Complications and consequences
Pathology of the aorta in the form of aneurysms of its ascending part and arch can cause complications and lead to such consequences as:
- Aortic dissecting aneurysm;
- Accumulation of lymphatic fluid in the pleural cavity (chylothorax);
- Calcification of the vessel wall;
- Formation of thrombus inside the saccular aneurysm, which, when displaced, causes peripheral thrombosis (thromboembolic complications). [7]
The larger the aneurysm, the higher the risk of rupture. A ruptured aortic arch aneurysm can lead to severe internal bleeding with life-threatening consequences. Read more - ruptured thoracic and abdominal aortic aneurysms: chances of survival, treatment
Diagnostics of the ascending aortic arch aneurysms
Instrumental diagnosis is necessary to detect an aneurysm of the ascending aortic arch:
- Chest x-ray;
- Chest CT scan;
- Transthoracic echocardiography;
- Aortic ultrasound;
- CT angiography coronary arteries and aorta;
- Magnetic resonance angiography thoracic vessels.
Patients take blood tests (general, biochemical, immunoenzymatic), general urinalysis. [8]
A differential diagnosis is performed to exclude pathologic mediastinal masses, intramural aortic hematoma and aortic dissection, and aortic arch anomaly in the form of Commerell's diverticulum.
Who to contact?
Treatment of the ascending aortic arch aneurysms
For aortic arch aneurysms, treatment depends on the size, growth rate and underlying cause. Aneurysms less than 5 cm in size usually do not require immediate surgery unless the patient has additional risk factors (family history of aneurysms, presence of connective tissue disease and aortic valve disease).
Usually hypotensive drugs of the group of alpha2-adrenoreceptor agonists, i.e. Alpha-adrenolytic drugs, are prescribed to control BP. The aneurysm size is monitored by periodic imaging examinations (X-ray, ultrasound, CT scan).
In case of a large (more than 5-5.5 cm) or rapidly growing aneurysm, surgical treatment is required, either by open surgery (removal of the vessel bulge and sewing of a graft) or by endovascular plasty of the vessel (placement of a stent in the aneurysm). For more information, see surgery for arterial aneurysms
When an aneurysm ruptures, surgery is performed as an emergency. [9]
Prevention
To reduce the risk of developing an aneurysm of the ascending aortic arch, doctors recommend controlling your weight, blood pressure and blood cholesterol levels, as well as a healthy diet, do not abuse alcohol and do not smoke.
Forecast
Given the multifactorial nature of this pathology and its possible consequences and complications, it is difficult to predict the outcome of the disease. Aneurysms of the ascending aortic arch can be fatal due to the tendency to delamination or rupture. [10]
According to the data of foreign specialists, after planned surgical intervention in almost 80% of cases the survival rate is about 10 years, but in acute untreated aortic dissection the lethal outcome within two days reaches 50% of cases. In emergency surgery for ruptured aneurysms, the mortality rate is 15-26%.