
Tricher Collins Syndrome
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Serious craniofacial deformations occur in intrauterine disorders of bone development, and one of the varieties of this pathology is the Tricker Collins syndrome (TCS) or mandibularfascial, ie maxillofacial dysostosis.
Code of the disease according to the ICD 10: class XVII (congenital anomalies, deformations and chromosomal abnormalities), Q75.4 - mandibulofacial dysostosis.
Causes of the Tricher Collins Syndrome
This syndrome was named after the outstanding British ophthalmologist Edward Tricher Collins, who described the main features of the pathology more than a hundred years ago. However, European doctors more often refer to this type of anomaly of the bones of the face and jaws as a disease or Franceschetti syndrome - based on extensive studies by the Swiss ophthalmologist Adolf Franceschetti, who introduced the term "mandibular fascial dysostosis" in the middle of the last century. In medical circles, the name is also used - Franceschetti-Collins syndrome.
The causes of the Tricer Collins syndrome are mutations of the TCOF1 gene (at the locus of chromosome 5q31.3-33.3), which encodes the nucleolar phosphoprotein responsible for the formation of the craniofacial part of the human embryo. As a result of a premature decrease in the amount of this protein, biogenesis and rRNA functions are disrupted. According to the geneticists of the Human Genome research program, these processes lead to a reduction in the proliferation of embryonic cells of the neural crest-the cushion along the nerve trough, which, during the development of the embryo, closes into the neural tube.
Formation of the tissues of the facial part of the skull occurs due to the transformation and differentiation of the cells of the upper (head) part of the neural crest, which migrate along the neural tube into the region of the first and second branchial arches of the embryo. And the deficit of these cells causes craniofacial deformities. The critical period of occurrence of anomalies is from 18 to 28 days after fertilization. After the migration of neural crest cells (at the fourth week of gestation) almost all loose mesenchymal tissues in the face area are formed, which later (from 5 to 8 weeks) are differentiated into skeletal and connective tissues of all parts of the face, neck, larynx, ear (including internal) and future teeth.
Pathogenesis
The pathogenesis of the Tricer Collins syndrome often has a family character, and the anomaly is inherited by an autosomal dominant principle, although there are cases of autosomal recessive defect transmission (with mutations of other genes, in particular, POLR1C and POLR1D). The most unpredictable in the maxillofacial dysostosis is that the mutation is inherited by children only in 40-48% of cases. That is, in 52-60% of patients the causes of the Tricer Collins syndrome are not related to the presence of an anomaly in the genus, and it is believed that the pathology arises from sporadic gene de novo mutations. Most likely, the new mutations represent the effects of teratogenic effects on the fetus during pregnancy.
Among the teratogenic causes of this syndrome, specialists refer to large doses of ethanol (ethyl alcohol), radiation, cigarette smoke, cytomegavirus and toxoplasm, and glyphosate-based herbicides (Roundal, Glorfor, Tornado, etc.). And the list of iatrogenic factors included preparations for acne and seborrhea with 13-cis-retinoic acid (Isotretinoin, Accutane); anticonvulsant drug Phenytoin (Dilantin, Epanutine); psychotropic drugs Diazepam, Valium, Relanium, Seduxen.
Symptoms of the Tricher Collins Syndrome
For the most part, the clinical signs of mandibulofascial dysostosis and the degree of their severity depend on the features of the manifestation of gene mutations. And the first signs of this anomaly in most cases are visible in the child immediately after his birth: the face with the syndrome of Tricher Collins has a characteristic appearance. Moreover, morphological anomalies are usually bilateral and symmetrical.
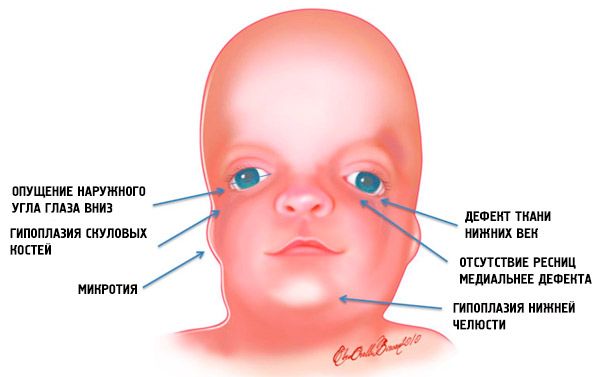
The most obvious symptoms of Tricer Collins syndrome are:
- underdevelopment (hypoplasia) of the facial bones of the skull: zygomatic, zygomatic processes of the frontal bone, lateral pterygoid plates, accessory sinuses of the nose, mandible and protrusions of bony epiphyses (condyles);
- underdevelopment of the bones of the lower jaw (micrognathia) and more obtuse than usually the mandibular angle;
- nose has a normal size, however, it seems great because of hypoplasia of the superciliary arches and underdevelopment or lack of zygomatic arches in the region of the temples;
- the eye slits are descending, that is, the incision of the eyes is abnormal, with the outer corners lowered downwards;
- defects of lower eyelids (coloboma) and partial absence of eyelashes on them;
- ears of irregular shape with a wide range of deviations, up to their location in the corner of the lower jaw, the absence of lobes, blind fistulas between the goat ear and the corner of the mouth, etc .;
- narrowing or infection (atresia) of the external auditory canal and anomalies of the ossicles of the middle ear;
- absence or hypoplasia of the parotid salivary glands;
- pharyngeal hypoplasia (narrowing of the pharynx and respiratory tract);
- non-healing of the hard palate (wolf mouth), as well as the absence, shortening or immobility of the soft palate.
Such anatomical abnormalities in all cases have complications. These are functional hearing impairments in the form of conductive (conductive) hearing loss or total deafness; impaired vision due to improper formation of eyeballs; Defects of the palate cause difficulties with feeding and swallowing. There are jaw-related violations of the occlusion of the teeth (an incorrect bite), which, in turn, causes problems with chewing and articulation. Pathologies of the soft palate explain the nasal voice.
Complications and consequences
The consequences of maxillofacial anomalies in the Tricher Collins syndrome are manifested in the fact that at the time of the birth of the child his intellectual abilities are normal, but because of hearing defects and other disorders, a secondary delay in mental development is noted.
In addition, children with such defects are acutely aware of their inferiority and suffer, which negatively affects their nervous system and psyche.
Diagnostics of the Tricher Collins Syndrome
Postnatal diagnosis of Tricher Collins syndrome is essentially based on clinical signs. Maxillofacial dysostosis is easily determined with complete expressiveness of the syndrome, but when there are minimal symptoms of pathology, problems can arise with the formulation of the correct diagnosis.
In this case, special attention is required to assess all the functions associated with anomalies, especially those that affect breathing (due to the threat of sleep apnea). Assessment and monitoring of the efficiency of feeding and saturation of hemoglobin with oxygen are also conducted.
In the future - on the 5th-6th day after birth - it is necessary to find out the degree of damage to the hearing with the help of audiological testing, which should be carried out in the maternity hospital.
An examination is made, during which the instrumental diagnosis is performed by fluoroscopy of cranial-facial dysmorphology; pantomography (panoramic x-ray of the bony structures of the facial skull); full cranial computed tomography in various projections; CT or MRI of the brain to determine the condition of the internal auditory meatus.
The earliest - prenatal diagnosis of maxillofacial anomalies in the presence of Tricher Collins syndrome in a family history is possible by biopsy chorionic villus at 10-11 weeks of gestation (the procedure threatens miscarriage and infection in the uterus).
Also blood tests of family members are taken; on 16-17 weeks of pregnancy, the analysis of amniotic fluid (transabdominal amniocentesis) is taken; on 18-20 weeks of pregnancy, fetoscopy is performed and blood is taken from the fruit vessels of the placenta.
But most often in the prenatal diagnosis of this syndrome the fetus uses ultrasound (at 20-24 weeks of pregnancy).
What tests are needed?
Differential diagnosis
The same methods are used by specialists when differential diagnostics is needed to recognize the faintly expressed Tricer Collins syndrome and distinguish it from other congenital anomalies of craniofacial bones, in particular: the syndromes of Aper, Cruson, Nager, Peters-Hevels, Hellerman-Stef, and with hemifacial microsomy (Goldenhar syndrome), hypertelorism, premature penetration of the cranial suture (craniostenosis), or fracture of the facial bones (craniosynostosis).
Who to contact?
Treatment of the Tricher Collins Syndrome
As in all cases of genetically conditioned birth defects, treatment of the Tricer Collins syndrome in severe forms is exclusively palliative, as there are no therapeutic methods for such pathologies. The spectrum and degree of deformation in this syndrome are extensive and, consequently, the nature and intensity of medical intervention also has a variety of options.
Hearing aids are used to correct and improve hearing, to improve speech - classes with a speech therapist.
Surgical interventions are required at an early age in severe cases of narrowing of the respiratory tract (tracheostomy) and larynx (gastrostomy for feeding). Oral correction of the palate may also be required.
Operations for lengthening the lower jaw are performed at the age of 2-3 years or later. Reconstruction of soft tissues includes correction of the lower eyelid colonies and plasty of the auricles.
Prevention
Forecast
What can the prognosis be for this pathology? It depends on the degree of deformity and the intensity of the symptoms. The Tricker Collins syndrome is a life-long diagnosis.
 [25]
[25]