
Sensitivity study
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

The most common complaint related to a violation in the sensory sphere is pain. If the patient has pain syndrome, it is necessary to clarify the following aspects:
- character of pain (acute, blunt, burning, stitching, shooting, etc.);
- localization and pain irradiation;
- time characteristics (constant, paroxysmal, periods of pain intensification / reduction) and their duration;
- the severity of the pain (the patient is offered to evaluate the pain on an 11-point scale, according to which 0 points corresponds to the absence of pain, 10 - to the maximum possible);
- factors contributing to the easing / intensification of pain (movement, a certain posture, rest, stress, taking analgesics, etc.);
- associated symptoms (visual impairment, muscle spasms, nausea or vomiting, etc.);
- the onset of pain (date, circumstances, accompanying the appearance of pain, possible cause, etc.).
The sensitivity evaluation is entirely based on the patient's self-report on his subjective sensations, therefore, when performing a neurological examination, sensitivity is investigated in the last place. Complaints and changes in the neurological status revealed in the pre-existing stages of the survey largely determine the characteristics of sensitivity studies in each individual patient. So, if the patient does not make complaints and no neurological disorders have been detected before, we can confine ourselves to screening sensitivity testing, which includes the study of pain sensitivity on the face, limbs and trunk, vibration and deep sensitivity on the limbs. On the contrary, if neurological disorders are identified and there are already assumptions about their cause, sensitivity is examined taking into account the formed hypothesis. Interpreting the results of a sensitivity study can be quite difficult. In many cases (fatigue, anxiety, depression, reduction of cognitive functions), self-evaluation of sensitive disorders does not reflect the real state of sensitive innervation of tissues and organs. So, an anxious patient with an analytical mindset is able to fix attention on the most insignificant sensations that have no clinical significance, while patients with a reduced level of wakefulness sometimes deny the most serious disorders.
Isolate simple and complex types of general somatosensory sensitivity. Simple types of general sensitivity according to their "receptor affiliation" are divided into superficial (perception of signals from the skin analyzer's exteroreceptors) and deep (perception of signals from the proprioceptors of the motor analyzer). In its turn, simple surface (skin or exteroceptive) sensitivity includes pain, temperature (cold and thermal), and tactile (touch, feeling of light touch), and simple deep sensitivity - the muscular-joint feeling (sense of passive movement, sense of position), dermal kinesthesia folds, a sense of pressure (strong touch), mass and vibration.
The results of the investigation of simple sensitivities reflect primarily the state of the receptor apparatus, the conductor part, and the primary sensory ("projection") cortical fields of the corresponding analyzers.
To complex types of sensitivity include a sense of localization, discrimination, two-dimensional and three-dimensional-spatial feeling. Sometimes the complex senses include the feeling of mass. Complex types of sensitivity are based on the analysis and synthesis of pulses of different modalities. Their research reflects the state of not only the conductor sections of analyzers and the primary sensory fields of the cortex, but also secondary and tertiary cortical receptor fields (that is, areas of the cortex that integrate information from various sensory organs).
Investigation of surface sensitivity
- Pain sensitivity is examined using a special safe needle soldered into a plastic casing, and a new needle should be used for each new patient. Pressing the needle should be strong enough to cause a painful feeling, but not traumatic. It is unacceptable to stab the patient "to the blood" or leave a scratch after testing. In response to a prick, the patient should report his feelings ("keenly" or "stupidly"), and not simply state the fact of touch. It is necessary to adhere to a certain sequence of testing: pain sensitivity is checked at symmetrical points on the right and left sides of the body, moving from the distal extremities to the proximal or from the area of one dermatome to the other. If an increase in the threshold of pain sensitivity is detected, they move from the area of reduced perception of pain to a safe area, starting from the center to the edges to determine the boundaries of the disturbance area. The defeat of the trunk of the peripheral nerve causes a violation of sensitivity in the zone of its autonomic innervation, and the spinal cord injury in the zone of the corresponding dermatome. With polyneuropathy disorders of pain sensitivity occupy the territory of "gloves" and "socks". We also note the presence of hyperalgesia.
- Tactile sensitivity is examined with a light touch of a piece of cotton wool or a brush with soft hair. Initially, they show the patient touches, applying them in the forehead area, and explain that he should report each touch he feels with the word "yes" or "feel." Then, the patient is asked to close his eyes and concentrate on analyzing the sensations obtained. The presence of hyperkeratosis in the region of the soles or palms increases the threshold of tactile sensitivity in these areas, which can not be considered as a neurological deficit.
- Temperature sensitivity (sensation of heat, cold) is usually investigated only in patients with gipalgesia. Use tubes with a hot (32-40 ° C) and cold (not above 25 ° C) water or other cold and warm objects (for example, a metal hammer and a doctor's finger). First, they determine the patient's ability to distinguish between cold and hot, applying warm and cold objects alternately to a region with a presumably preserved sensitivity. Normally the difference of 2 ° C is already noticeable to the subject. Then apply a cold (or warm) object alternately to the symmetrical parts of the body, starting from the rear of the foot, moving upward and comparing the intensity of perception of the temperature stimulus to the right and left. Studies of cold and heat sensitivity are carried out separately, since they can be broken to varying degrees. If necessary, also investigate the temperature sensitivity in various dermatomes or in zones of autonomic innervation of the affected nerves, finding the boundaries of the changed sensitivity. A clear definition of the territory of the disturbed sensitivity, coinciding with a certain innervation, allows the subjective feeling of the patient to be transformed into an objective neurological sign.
Investigation of deep sensitivity
- The sense of vibration arises when the deep receptors are stimulated by vibrations of a certain frequency and amplitude. For research use low-frequency (64-128 Hz) tuning fork. It is advisable to independently test the tuning fork on healthy people. Normally, the feeling of vibration on the ankles continues from 9 (tuning fork 48 Hz) to 21 seconds (tuning fork 64 Hz). Vibration sensitivity is examined on the fingers and toes, on the ankles, patella, pelvic bones, radial and ulnar bones, clavicle, skull. To the area under investigation, attach the leg of the vibrating tuning fork and ask the patient to inform him when he ceases to perceive the oscillations. Compare the threshold of vibration sensitivity on the right and left limbs. If the vibration sensitivity on the foot is broken, check it in the ankle, knee, hip joint area to determine the boundaries of the disorder. Similarly, the vibration sensitivity on the fingers is investigated. Vibration sensitivity decreases with peripheral polyneuropathies and spinal cord diseases involving its posterior funicles. At the same time, the vibration sensitivity can only decrease in the distal parts of the legs and remain intact in the hands. Moderate increase in the threshold of vibration sensitivity in elderly people is observed even in the absence of any neurological pathology.
- Muscular-articular feeling. The patient is first shown what passive movements will be made with his fingers and how to call them. Then the patient is asked to close his eyes, take the nail phalanx of the finger behind the side surfaces and smoothly move the finger up, then down; The patient must report in which direction (up or down) his finger is moved. Normally, a person is very sensitive to even very thin passive movements in the joints and is able to distinguish the movement by an angle of 1-2 °. If the muscular-articular feeling in the patient is disturbed in the distal parts of the limbs, check the sensation of passive movements in the joints located more proximally.
- The feeling of the position is examined by giving the limb a certain position. The patient should, with his eyes closed, determine this position. If the feeling of movement in the joint is perceived primarily by receptors localized in the tendons and joints, then the receptors located in the muscles, that is, the afferents of the muscle spindle, are responsible for determining the static position of the part of the body in space.
Evaluation of research results
Based on complaints, anamnestic data and the results of the investigation of surface sensitivities, one can form an idea of the disorders present in the patient.
- The decrease / absence of sensitivity is denoted by the terms "hypoesthesia" and "anesthesia" (for pain sensitivity - "hypalgesia" and "analgesia", for temperature sensitivity - "thermohyesthesia" and "thermoanesthesia", for deep - "batianesthesia").
- The increase in sensitivity to ordinary non-spontaneous stimuli is called hyperesthesia, increased sensitivity to pain - hyperalgesia.

The above violations are designated as quantitative disorders; to qualitative disorders of sensitivity include the following.
- Polyesthesia (one shot is perceived as multiple).
- Alloheiria (the patient determines the irritation not in the place where it was applied, but on the opposite half of the body).
- Synaesthesia (sensation of perception and in the place of application of the stimulus, and in another place where it was not applied).
- Paresthesia (spontaneous or caused by unusual sensations).
- Neuralgia (extremely severe acute pain, spreading over one or more nerves).
- Causalgia (sensation of intense burning pain).
- Dysaesthesia (perverted perception of receptor affiliation). Variants of dysesthesia: temperature - the appearance of a sensation of heat in response to a shot; allodynia - the appearance of pain in response to irritation, which is normally not accompanied by them (sometimes allodynia refers only to the pain response to a touch of a brush, while the pain sensations for temperature effects and pressure are designated respectively by the terms "hyperalgesia for cold and heat" and "hyperalgesia at pressure").
- Hyperpathy (the appearance of excruciating pain in response to repeated pain and sky stimuli combined with an increase in the threshold of perception of a single stimulus and the difficulty of a clear localization of stimulation).
The study of simple types of general sensitivity also makes it possible to determine the type of distribution of sensitivity disorders.
- The defeat of the nerve trunks leads to a peripheral neural type of distribution of sensitivity disorders. It is characterized by a violation of all sensitivities in the innervation zone of the peripheral nerves (when the plexus is affected, in the innervation zone of the plexus, when the individual nerve is affected, in the innervation zone of this nerve, and with polyneuropathy in the distal sections of the extremities). Sensitive disorders are usually combined with paresis or paralysis of muscles innervated by the corresponding nerves.
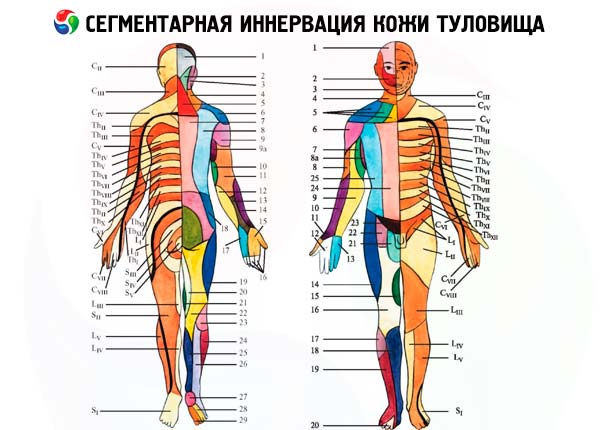
- The defeat of the posterior roots of the spinal nerves is accompanied by the appearance of a peripheral radicular type of sensitive disorders. Violated all kinds of sensitivity in dermatomes, corresponding to the affected roots. However, since the cutaneous zones of innervation of adjacent roots partially overlap, when one spine is turned off, no loss of sensitivity is detected (the region of the corresponding dermatome continues to be provided with adjacent roots). Clearly in the zone of one dermatome, sensitivity is disturbed only when three adjacent roots are affected. The decrease in sensitivity in this type of disorder is accompanied by severe pain and paresthesia in the corresponding dermatomes.
- The defeat of the posterior horns of the spinal cord can cause a spinal segmental type of sensitivity disorder: ipsilateral impairment of pain and temperature sensitivity in one or more dermatomes with the preservation of tactile sensitivity in these segments. Such dissociated anesthesia can occur with intramedullary tumors, myelo-ischemia, and hematomyelia, but is most characteristic of syringomyelia, which is manifested by the formation of cavities in the gray matter of the spinal cord. Since the localization of the syringomyelic cavities in the cervical and upper thoracic parts of the spinal cord is typical, the zone of sensitive disorders has the appearance of a "half-jacket", and when the cavity is spread to the other half of the spinal cord or at the initial central location of the cavity, the form of the "jacket". When the spinal cord of the trigeminal nerve is involved in the process of the nucleus, the pain and temperature sensitivity on the face in the outer zones of the Selder falls out; middle and inner zones are involved later.
- The spinal conductor type of the distribution of sensitive disorders occurs when the pathways in the cord of the spinal cord are damaged. When the lateral cord is affected with involvement of the lateral spinotalamic tract, there is a violation of the temperature and pain sensitivity on the opposite side to one or three dermatomes below the level of the focus. When the posterior cord is injured, there is a violation of deep sensitivity (vibration sensitivity and muscular-articular feeling) on the side of the focus; while pain and temperature sensitivity remains intact. This disorder is combined with ipsilateral and sensitive ataxia.
- Braun-Secar syndrome occurs when one half of the transverse section of the spinal cord is affected. On the side of the lesion below the level of the focus, there is spastic paralysis (break of the pyramidal tract) and a violation of deep sensitivity (disconnection of the back cord), and on the opposite side from a level located several segments below the level of the lesion, a disorder of pain and temperature sensitivity according to the conductor type spinotalamicheskogo tract in the side cord).
- The central type of distribution of sensitive disorders occurs when the brain structures are damaged. Its manifestations differ depending on which level and which structures suffer, but in any case, with unilateral localization of the focus above the level of the medulla oblongata, the sensitivity on the trunk is disturbed on the opposite side to the side.
- The defeat of the lateral parts of the medulla oblongata (dorsolateral medullary syndrome Wallenberg-Zakharchenko) causes loss of pain and temperature sensitivity on the same side of the face (involvement of the nucleus of the spinal cord of the trigeminal nerve), a decrease in pain and temperature sensitivity at the opposite foci of half of the body and extremities (damage to the spinotalamic tract) and decrease of deep sensitivity on the side of the focus in the extremities (involvement of the cores of the thin and wedge-shaped bundles). Sensitive disorders are combined with cerebellar ataxia on the side of the focus (lower leg of the cerebellum); dizziness, nystagmus when looking toward the lesion, nausea and vomiting (vestibular nuclei and their connections); Bernard-Horner's symptom on the side of the focus (defeat of descending pathways from hypothalamus to ciliospinal center in lateral horns C 8 -T 2 ); dysarthria, dysphagia, dysphonia, ipsilateral paralysis of the muscles of the soft palate, pharynx and vocal cords (defeat of the double core of IX-X pairs of cranial nerves).
- The defeat of the thalamus (usually of the vascular nature) leads to the loss of all kinds of sensitivity on the opposite side to the side of the body. As a rule, the sensitivity gradually improves, however, on the same side of the body, burning ("thalamic") pains develop over time, which are provoked by any stimuli, especially cold and emotional stress. These pains are painful diffuse and can be noted against the background of an increase in the threshold of pain sensitivity. Simultaneously, sensitive hemiataxia is detected in contralateral foci of limbs and hemianopsia. Often, a "thalamic arm" is formed (the shoulder is pressed to the trunk, the forearm and the wrist are bent, the brush is penetrated, the proximal phalanges of the fingers are bent, the others are bent).
- When the posterior end of the inner capsule is injured, hemiansesthesia occurs in its posterior third on the opposite side of the body with violation of all sensitivities (defeat of thalamocortical fibers) and sensitized hemiataxy, often combined with the contralateral foci with hemianopsia (visual eye involvement). When the pathological process involves the entire posterior stalk of the inner capsule, hemianesthesia and hemianopsia are combined with the contralateral foci by central hemiplegia.
- The defeat of the primary sensory cortex (postcentral gyrus) causes some decrease in pain, temperature and tactile sensitivity on the opposite side of the body. The whole half of the body does not suffer, but only the area corresponding to the projection of the pathological focus. In addition, there may be paresthesia (sensation of tingling, chills and numbness) in the affected limb.
Complex types of sensitivity reflect the analytical and synthetic work of the parietal lobe of the brain, which integrates the elementary sensory modalities. Therefore, it is advisable to investigate complex types of sensitivity only with the preservation of simple species of general sensitivity. Thus, in a patient with peripheral neuropathy or spinal cord injury, there is little point in testing cortical sensory functions.
- Discriminative feeling is the ability to distinguish between two stimuli that are simultaneously applied to closely spaced areas of the body surface. For the study use a pair of compasses or two paper clips. One or two irritations are applied to the area under investigation, asking the patient to report how many irritations (one or two) he feels. The threshold of discrimination sensitivity (that is, the minimum distance between the sites of application of stimulation, in which it is perceived as double) varies greatly in different parts of the body: the tips of the fingers are most sensitive (4 mm), the least is the back region (7 mm).
- The sense of localization is checked by applying tactile stimulation to different parts of the body. The patient should determine the place of touch.
- Stereognosis is the ability to recognize a familiar object when feeling with closed eyes. The patient is asked to close his eyes, give him a familiar object (coin, key, matchbox) in his hand and suggest to determine what it is. Normally, a person recognizes objects and even is able to determine the value of various coins. The destruction of the inferior parietal lobe of any hemisphere causes asteroognosis. In left-sided lesions, asteroognosis occurs in the right hand, with a right-sided lesion marking the bilateral decrease in tactile gnosis. The patient retains the ability to sense an object in his hand, but is not able to recognize it by touch with closed eyes. In addition, there may be a defect in discriminatory sensitivity and feelings of localization.
- Two-dimensional sense of space (graveesthesia). The patient is offered to close his eyes and determine the letter or figure that the doctor is drawing on his palm with a blunt object. Compare the perception on the right and left side.
- The feeling of mass (baresthesia). The patient compares the mass of two similar objects that are placed on the palm of his outstretched hands. In typical cases, the object that the patient holds in the injured hand seems to be easier, regardless of its mass.
- Test of synchronous bilateral stimulation used in patients with lesions of the parietal lobe, to identify unilateral spatial ny neglekt (ignoring the phenomenon of one-half the space) on the side opposite the lesion focus. Touch up to one side of the body of the subject (face or hand), then simultaneously to symmetrical areas on both sides. Ask him to tell which side of the body (to the right, to the left, to both) is touched. If he correctly recognizes each side separately, but when stimulating both halves of the body at once, guesses touch only on one side, diagnose hemispheric ignoring.
 [
[