
Shihan Syndrome
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Ischemic necrosis of the pituitary gland and persistent decline in its functions due to postpartum hemorrhage was termed Shihan syndrome. This rare complication of childbirth, accompanied by life-threatening blood loss, is also called postnatal pituitary insufficiency, postpartum hypopituitarism, pituitary (diencephalic-pituitary) cachexia or Symmonds disease.
This endocrine pathology has code E23.0 for ICD-10.
Epidemiology
In developed countries, due to the high level of obstetric care, Shihan syndrome is rare: its frequency has declined from 10-20 cases per 100,000 women to 0.5% of all cases of hypopituitarism in women over 50 years.
According to the European Society of Endocrinology, some symptoms of slight damage to the anterior lobe of the pituitary gland are found in 4% of women who have lost a lot of blood at birth. Moderate signs of Shihan syndrome are diagnosed in 8%, and severe forms of postpartum hypopituitarism are 50% of women after hypovolemic shock.
In the international database of the pharmacoepidemiological register KIMS (Pfizer International Metabolic Database) for 2012, there are 1034 patients with growth hormone (STH) deficiency, and in 3.1% of cases in women, the cause of this pathology is Shihan syndrome.
Postpartum hypopituitarism poses a serious threat to women in underdeveloped and developing countries. For example, in India the prevalence of Shihan syndrome is estimated at 2.7-3.9% among women giving birth over 20 years.
Causes of the shihan syndrome
All causes of Shihan syndrome are the result of hypovolemic shock, which develops with a sharp decrease in the volume of circulating blood and a drop in blood pressure caused by bleeding during childbirth.
With massive blood loss (more than 800 ml), blood supply to organs and oxygen supply to them is impaired. And, first of all, it concerns the brain. Syndrome Shihana arises from the damage to the pituitary gland (pituitary gland) - the gland of the brain responsible for the synthesis of the most important hormones.
The most affected hormone-producing cells of its anterior lobe - adenohypophysis. During the period of gestation - under the influence of placenta hormones - the size of this gland increases, according to some estimates, by 120-136%. In particular, there is hypertrophy and hyperplasia of lacto-cytopocytes - cells that synthesize prolactin, necessary for the development and preparation of the mammary glands to produce milk.

Risk factors
Obstetricians-gynecologists note the risk factors for the development of Shihan's syndrome:
- disorders of blood coagulation in pregnant women (in particular, thrombocytopenia);
- edema of peripheral tissues (in which the hormone of the hypothalamus activates vasopressin, which increases vascular tone and blood pressure);
- gestational hypertension (high blood pressure);
- pre-eclampsia (high blood pressure and proteinuria);
- increased hemolysis (destruction of red blood cells, most often associated with kidney failure).
The risk of bleeding during childbirth and the emergence of Shihan syndrome in cases of placenta previa, premature detachment, as well as in multiple pregnancies (twins or triplets) and with rapid (turbulent) births during which embolism of the vessels of the lungs with amniotic fluid may be increased.
Pathogenesis
The pathogenesis of Shihan syndrome is associated with hypoxia of the pituitary tissues and their death. In the increased vulnerability of the adenohypophysis, the main role is played by the peculiarity of its blood supply: through the portal venous system and the network of capillary anastomoses of the portal vessels. With severe bleeding and a fall in blood pressure, there is no local blood flow in the enlarged anterior lobe of the gland; associated with a shock of spasm of blood vessels that feed the pituitary, leads to a lack of oxygen and ischemic necrosis of the gland.
As a consequence, the pituitary does not produce a sufficient number of such tropic hormones:
- somatotropin (STH), activating the cellular synthesis of proteins regulating the metabolism of carbohydrates and hydrolysis of lipids;
- prolactin (luteotropic hormone), stimulating the development and function of the mammary glands and yellow body;
- follicle-stimulating hormone (FSH), which provides growth of ovarian follicles and proliferative processes of uterus tissues;
- luteinizing hormone (LH), responsible for ovulation;
- adrenocorticotropic hormone (ACTH), which activates the production of corticosteroids by the adrenal cortex;
- thyroid-stimulating hormone (TSH), regulating the secretory function of the thyroid gland.
Symptoms of the shihan syndrome
Violation of the balance of hormones produced by the pituitary gland generates very diverse symptoms of Shihan syndrome, which depend on the degree of insufficiency of the secretion of specific pituitary hormones.
The volume of damaged pituitary cells determines the acute and chronic forms of the disease. The acute form reflects significant damage to the anterior lobe of the gland, and the symptoms become evident soon after delivery. In chronic cases, the lesions detected are less, and the symptoms may not appear for several months or years after delivery.
The most common first signs of Shihan syndrome are agalactia, that is, lack of lactation. Due to the long-term lack of estrogen at the right time after delivery, the menstrual cycle does not resume, the mammary glands decrease, the mucous membrane of the vagina becomes thinner. A deficiency of gonadotropin is expressed in amenorrhea, oligomenorrhea, decreased libido. In some women, menstruation resumes, and a second pregnancy is possible.
Characteristic symptoms of thyroid-stimulating hormone deficiency in Shihan syndrome are manifested by fatigue and a violation of thermoregulation with intolerance to cold; dry skin, hair loss and brittle nails; constipation and weight gain. These symptoms usually develop gradually.
The effects of a deficit of growth hormone are limited to some loss of muscle strength, an increase in fat tissue in the body and an increased sensitivity to insulin. Both in acute and chronic forms, there may be signs of diabetes insipidus: strong thirst and increased diuresis (volume of urine).
Symptoms of Shihan syndrome include signs of secondary adrenocortical insufficiency, that is, lack of ACTH. This decrease in overall body tone and body weight loss, hypoglycemia (low blood sugar), anemia and hyponatremia (low sodium levels). Deficiency of this hormone leads to chronic hypotension with syncope and orthostatic hypotension, inability to respond to stress. Also, hypopigmentation and folds on the skin (several weeks or months after delivery) are observed.
Exacerbation of adrenal insufficiency, which requires urgent medical care, occurs in severe infections or surgical interventions.
Complications and consequences
Severe pituitary insufficiency in Shihan syndrome can lead to coma and death.
Potentially life-threatening postpartum pangypopituitarism is also less common - when 90% of adenohypophysis tissues are affected. The consequences and complications of this severe form of Shihan syndrome: constant low blood pressure, cardiac arrhythmia, low blood sugar (hypoglycemia), hypochromic type anemia.
Diagnostics of the shihan syndrome
Usually the diagnosis of Shihan syndrome is based on clinical signs and medical history of patients, in particular, whether there was bleeding during labor or any other complications associated with childbirth. Important information about problems with lactation or the absence of menstruation after childbirth, which are two important signs of this syndrome.
To test the level of pituitary hormones (TTG, ACTH, FSH, LH, T4), cortisol and estradiol requires blood tests.
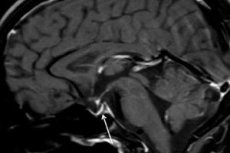
Instrumental diagnosis - using computed tomography (CT) or magnetic resonance imaging (MRI) of the brain - allows you to study the size and structure of the pituitary gland. In the early stages of the pituitary gland, the pituitary gland is enlarged, and at the time of iron it becomes atrophic, and the diagnostic sign of pathology revealed during the scan is developed as an "empty Turkish saddle", that is, the absence of the pituitary gland in the pituitary bone fossa at the base of the brain.
Differential diagnosis
The task that differential diagnosis should perform is to identify other diseases that are manifested by hypopituitarism: pituitary adenomas, craniopharyngiomas, meningiomas, chordomas, ependymomas or gliomas.
The pituitary gland can be damaged by brain abscess, meningitis, encephalitis, neurosarcoidosis, histiocytosis, hemochromatosis, autoimmune or lymphoblastic hypophysitis, and autoimmune antiphospholipid syndrome.
Who to contact?
Treatment of the shihan syndrome
Treatment of Shihan syndrome is a lifelong hormone replacement therapy with the use of synthetic analogs of tropic hormones of the ovaries, thyroid gland, adrenal cortex.
Thus, the deficiency of ACTH and cortisol is compensated by the intake of glucocorticoids (hydrocortisone or prednisolone). Preparations of thyroxine (levothyroxine, tetraiodothyronine, etc.) replaces the thyroid hormone, and the blood test data on serum free thyroxine levels help to adjust their dosage.
Estrogen deficiency is usually supplemented by the use of oral contraceptives, and these hormones should be taken by women with Shihan syndrome before the age of menopause.
Endocrinologists note that if the level of hormones in the blood is controlled, there are usually no side effects. Side effects can be when the dose of hormonal drugs is too high or too low. Therefore, patients with this syndrome are on dispensary registration, undergo regular examinations and take blood tests for hormones.