
Fractures of the zygomatic bone and zygomatic arch: causes, symptoms, diagnosis, treatment
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
 [
[What causes a fracture of the malar bone and zygomatic arch?
According to the literature, patients with fractures of the zygomatic bone and arch make up 6.5 to 19.4% of the total number of patients with injuries of the bones of the face. They make up only 8.5%, because not only patients enter the clinics for emergency care, but also a significant number of planned patients who need complex reconstructive-reconstructive surgeries after trauma to other bones of the face. The reason for them is often household (fall, punch or solid object), industrial, transport or sports injuries.
According to the most common classification developed in the clinic of the CNIIS, the fractures of the zygomatic bone and zygomatic arch are divided into the following groups:
- fresh closed or open isolated fractures without displacement or with a slight displacement of fragments;
- fresh closed or open fractures with a significant displacement of fragments;
- fresh closed or open combined fractures without bias or displacement of fragments;
- fresh closed or open combined fractures with simultaneous damage to other bones of the face;
- chronic fractures and traumatic defects of the zygomatic bone and arch with deformation of the face and violation of the movements of the lower jaw.
Approximately the same classifies such fractures Yu. E. Bragin.
In some cases, instead of the term "zygomatic bone", the term "anterior branch of the zygomatic arch" is used, and instead of the "zygomatic arch", the "posterior part of the zygomatic arch".
Non-fire damage to the malar bone and arch can be divided into three groups:
- bilge-jaw fractures (closed or open, with displacement of fragments or without displacement);
- fractures of the zygomatic arch (closed or open, with displacement of fragments or without displacement);
- improperly fused cheek-jaw fractures or fractures of the zygomatic arch (with deformity of the face, persistent contracture of the lower jaw, or phenomena of chronic inflammation of the maxillary sinus).
Given the literature data and the experience of our clinic, all lesions of the zygomatic bone and arch, depending on the time elapsed since the injury, can be divided into three groups:
- fresh fractures - up to 10 days after injury;
- chronic fractures - 11-30 days;
- incorrectly fused and not merged - more than 30 days.
Direct contact of the bones of the person with each other as a whole and with the malar bone - in particular, as well as the complexity and variety of the vascular and nervous plexuses that are located here determine! Occurrence in the trauma of this area of various injuries, united under the name "Purcher syndrome", or a syndrome of traumatic retinopathy and angiopathy. This syndrome includes a decrease in visual acuity 1-2 days after trauma, cicatricial changes in the retina of the eye, pigmentation and atrophy of the optic nerve of various degrees, up to retinal detachment after several months from the time of injury.
Symptoms of a fracture of the malar bone and zygomatic arch
Fractures of the zygomatic bones are usually combined with a closed craniocerebral trauma: most often with concussion of the brain, less often with a moderate or severe bruise.
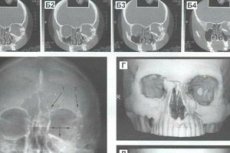
In most cases, with a fracture, the malar bone is displaced downward, inward and backward; less often the mixing is directed upward, inward and backward, and even more rarely - outward and backward or forward. With any displacement of the malar bone, the infraorbital nerve or its posterior upper alveolar branches are damaged, which manifests itself as a violation of the sensitivity of the skin of the infraorbital region, upper lip, nose wing, and electrical excitability of the teeth of the upper jaw. Isolated fractures of the zygomatic bone, as a rule, do not occur. The often observed introduction of the zygomatic bone into the maxillary sinus leads to its filling with blood as a result of damage to the bone walls and sinus mucosa, which in turn promotes the development of traumatic sinusitis. The dimensions of the maxillary sinus are reduced, but on the roentgenogram this remains unnoticed due to a sharp decrease in sinus pneumatization. The obscurity of the contours of the maxillary sinus can also be caused by the penetration of fatty tissue from the orbit into it.
The old fractures of the malar bone. Cosmetic and functional disorders in chronic fractures depend on the localization of the fracture, the degree of displacement of bone fragments, bone loss, the duration of the trauma, the nature of the treatment used, the vastness of the scar formation, the presence of chronic sinusitis or osteomyelitis of the zygomatic bone, maxilla, saliva fistula.
Diagnosis of fracture of the malar bone and zygomatic arch
Diagnosis of fractures of the zygomatic bone and arch is based on data of anamnesis, external examination, palpation of the area of the lesion, examination of the bite, anterior rhinoscopy, radiography in the axial and sagittal (naso-chin) projections. In Table. 4 presents the subjective and objective symptoms of fracture of the malar bone and zygomatic arch.
In the first hours after injury before the onset of edema, infiltration or palpation of the hematoma, it is possible to obtain so many valuable objective data that in some cases the need for radiographic examination is no longer necessary.
Displacement of fragments can be of different degrees, and the asymmetry of the face and the westernization of the eyeball, being a cosmetic defect. May be accompanied by functional disorders in the form of diplopia, restriction of opening the mouth. Therefore, for each of the 8 listed classes of fresh fractures of the malar bone, there is a combination of a number of symptoms of cosmetic and functional disorders in varying degrees.
Treatment of fractures of the zygomatic bone and arch
Treatment of fractures of the zygomatic bone and arch depends on the prescription and localization of the fracture, the direction and degree of displacement of fragments, the presence of concomitant common disorders (concussion, brain contusion) and damage to surrounding soft tissues.
When comotio-concussion syndrome, take the necessary measures in this case. Local interventions are determined primarily by the prescription of the fracture, the degree and direction of the displacement of fragments, the presence or absence of damage to adjacent soft tissues and bones.
Treatment of fractures of the zygomatic bones and arches can be conservative and surgical. The latter, in turn, is divided into bloodless (non-operative) and bloody (operative).
All surgical methods of treatment are also divided into intraoral and extraoral.
Non-operative surgical treatment of the fracture of the zygomatic bone and zygomatic arch is shown with easily repaired, fresh closed fractures with varying degrees of displacement of the zygomatic bone, arch or fragments. There are two options for this treatment:
- the surgeon inserts the index or thumb of the hand into the posterior section of the upper arch of the vestibule of the mouth and reps the cheekbone, controlling the fingers of the other arm with the correctness and adequacy of the reposition;
- wrapped gauze spatula or spatula Buyalsky introduced into the same area and raise their cheekbone, arch or their fragments. In this case, it is advisable not to use a spatula on the cheek-alveolar ridge. A bloodless method can be effective for fresh fractures (in the first three days). If it is unsuccessful, one of the operational methods is used.
Conservative treatment of fracture of the malar bone and zygomatic arch
Conservative treatment is indicated with fresh fractures of the zygomatic arch or bone without significant displacement of the fragments.
Intraoral method Keen
This method is indicated for fractures of the third class and consists in the fact that in the upper-posterior part of the vestibule of the mouth a cut is made behind the cheek-alveolar crest through which a short and strong elevator is inserted, it is advanced to a displaced bone and vigorously moving up and outwards to re-insert it in the correct position.
Wielage Method
The method is a modification of the Keen method with the only difference being that it is applied to both the zygomatic bone and the zygomatic arch.
For this purpose, it is also possible to use the retractor AG Mamonov, AA Nesmeyanov, EA Glukina, who stupidly pass through the wound to the region of the transitional fold at the level of the projection of the tips of the roots of the teeth, reaching the surface of the tuberosus of the maxilla (with the zygomatic bone) or scaly part of the temporal bone (with zygomatic arch pointing). Pressing the hand on the retractor makes it easier to move the fragments of the bone and set them in the correct position; With a free hand, the doctor controls the movement of the fragments. The therapeutic effect is determined by the results of clinical and radiological examination of the patient in the postoperative period.
Method MD Dubova
This method consists in lengthening the Keen-Wielage incision to the first incisor for simultaneous revision of the anterior-lateral wall of the maxilla and maxillary sinus. It is indicated in the treatment of fractures of the zygomatic bone, combined with a fine-lop-sided injury of the maxillary sinus. In these cases, exfoliate the mucus-periosteal flap, release soft tissues that are restrained between the fragments, correct (with the help of a spatula or a spoonful of Buyalski) fragments of bone, remove fragments of the mucous membrane and blood clots. Then pick up the fragments of the lower wall of the orbit and the iodoform-gauze swab impregnated with petroleum jelly, fill the cavity (to keep the fragments in the correct position). The end of the tampon is outwardly formed through the surgeon's formation with the lower nasal passage. On the eve of the mouth, the wound is sewn tightly. The tampon is removed after 14 days.
Duchange Method
Special Dipschang forceps, equipped with cheeks with sharp teeth, grasp the cheekbone and direct it. In the same way, the zygomatic bone is repositioned by the forceps of S. K. Chollaria.
The method of A. A. Limberg
The method is used for a relatively small time of fracture (up to 10 days). The displaced zygomatic arch or bone is caught from the outside (through the puncture of the skin) by a special single-tooth crochet with a transversely located handle and pulled into the correct position. However, in some patients with the V-shaped fracture of the zygomatic arch, A. A. Limberg's one-tooth hook does not provide the same level of detachment of fragments, since it can be brought only under one fragment, and the other either stays in place or is shifted (set) first. To eliminate this defect, Yu. E. Bragin proposed a two-toothed hook having a more comfortable handle, taking into account the anatomical features of the surgeon's brush, and an opening on each tooth. Through these holes, ligatures are carried out under the fragments of the zygomatic arch to fix them to the outer tire.
The method of PV Khodorovich and VI Barinova
This method involves the use of advanced forceps, which, if necessary, move bone fragments not only outside but also in all other directions.
The method of Yu. E. Bragin
The method can be used even for very old fractures (prescription over 3 weeks) due to the fact that the device is built on the principle of a screw, allowing with a minimal effort of the surgeon to gradually increase the displacing (reponning) force of influence on the cheekbone, distributing and transferring it to the skull bones two support platforms. It is also important that the hooks of the apparatus are placed on the edges of the fragment of the malar bone without preliminary dissection of the soft tissues.
The method of VA Malanchuk and PV Khodorovich
This method can be used for both fresh and old fractures. The advantage of the method is that only one support (in the region of the parietal bone) is required to establish the apparatus. The use of the apparatus of VA Malanchuk and PV Khodorovich makes it possible to exclude, almost completely, the more complex surgical methods of introducing the zygomatic bone and the arch with the application of bone seams. Thanks to the application of this method in our clinic, in the treatment of fresh fractures of the cheekbone complex, good results were obtained in 95.2% of cases, satisfactory at 4.8%, in the treatment of chronic (11-30 days) fractures - 90.9% and 9.1%, respectively, in the treatment of improperly intergrown fractures (over 30 days) - 57.2% and 35.7%, and unsatisfactory results - in 7.1% of cases. At a greater prescription of a trauma the open osteotomy and osteosynthesis of fragments is shown.
Contouring facial plastic surgery for fractures of the cheekbone complex is indicated with normal function of the mandible and cosmetic defects that are older than 1-2 years. Palliative surgery - resection of the coronoid process of the lower jaw, or osteotomy and reposition of the zygomatic arch - are indicated if the lower jaw function is impaired.
If the surgeon does not have one of the devices described above for correcting long-lasting fractures with a displacement of fragments that occurred 10 or more days ago, it is often inexpedient to direct fragments with bloodless and operative methods. In such cases, one-stage refracture, reposition and fixation of the jaw bone fragments or slow reposition of the fragments by means of their elastic (rubber or spring) extension is carried out.
If these methods proved to be ineffective, different approaches can be used to perform one-step operative repositioning and fixation of the zygomatic bone, arc or their fragments: intraoral (subcutaneous and transonic), temporal, transverse, orbital, and bilo-arched.
The temporal method of Gillis, Kilner, Stone (1927)
The hair in the temple area is shaved off and a cut of the skin and subcutaneous tissue is about 2 cm long, somewhat backward from the border of the hairline. A long wide elevator is introduced into the incision, it is advanced to the zygomatic arch. Controlling the outside with the fingers of the other hand, the displaced bone is repaired using the elevator.
Reduction of the zygomatic bone and the lower wall of the orbit via the canine fossa and maxillary sinus by the Kazanjian-Converse
Having made an intraoral cut along the transitional fold within the canine fossa, it is exposed by lifting up the mucosal-periosteal flap, which is held by a curved crochet. In the anterolateral wall of the intermaxillary sinus, a window is made through which blood clots are removed from it. The finger examines the wall of the maxillary sinus, reveals the place of fracture of the lower wall of the orbit and specifies the degree of compression of the zygomatic bone into the maxillary sinus. The bony walls of the maxillary sinus and the malar bone are repaired by means of a tamponade of the sinus cavity with a soft rubber tube filled with gauze strips (pre-soaked with oil and a solution of antibiotics). The end of the rubber tube is inserted into the nasal cavity (as in the case of maxillary sinus after Caldwell-Luc). The wound is sewn tightly over the transitional fold; The tampon is removed after 2 weeks.
To simplify this method, it is possible to make an incision of the mucous membrane along the entire length of the transitional fold on the side of the lesion, which allows lifting up the widely peeled soft tissues and examining the anterior and posterior surfaces of the maxilla, the zone of the mandibular suture and the lower sections of the zygoma. After opening the maxillary sinus, examine and palpate the posterior and lower walls of the orbit. At the same time, the presence of the zygomatic bone in the maxillary sinus, the fracture of the lower wall of the orbit, the proliferation of the fatty tissue of the orbit or cheek in the maxillary sinus, the entry of small bone fragments and blood clots into it are clarified. Then, with the help of a narrow raspora, the zygomatic bone and the walls of the maxillary sinus are fixed, and then tightly plastered with iodoform gauze, as recommended by Bonnet, AI Kosachev, AV Klementov, B. Ya. Kelman, and others. A tampon whose end are removed into the lower nasal passage, they are removed after 12-20 days (depending on the age of the fracture and the degree of difficulty in correcting bone fragments due to the formation of fibrous adhesions). A long tamponade of the maxillary sinus gives a good effect and does not cause complications, among which the development of diplopia is especially painful for patients. Some authors recommend using inflatable rubber cylinders instead of iodoform gauze.
Suture on bone
Gill suggested that after a reposition of the zygomatic bone through the temporal or intraoral cut through the temporal or intraoral cut, two additional incisions should be made in the region of the forehead-frontal and cheek-maxillary sutures, and then one hole should be made on each side of the fracture site. They introduce a steel wire (in our clinic we use a polyamide thread) with a diameter of 0.4-0.6 mm. By pulling and tying the ends of the threaded wire or polyamide thread, they reach the rendezvous of fragments and their tight contact.
Suspension and extension of the zygomatic bone
Suspension and traction of the zygomatic bone occurs when it can not be corrected by the Wielage method through intraoral access. When suspended by the method of Kazanjian using a cut at the lower edge of the lower eyelid, the cheek part of the infraorbital margin is exposed. In the bone, a hole is drilled, through which a thin wire is made of stainless steel. The end of it is pulled outward and bent in the form of a hook or loop, by means of which the elastic stretching is carried out to a tripod-rod, mounted in a gypsum cap. You can also approach the bone through the intraoral cut of Caldwell-Luc.
Extension of the zygomatic bone
Extension of the zygomatic bone (usually outward and forward) is carried out with a polyamide thread, threaded through the hole in it. The cheek bone is exposed with the help of an external incision in the place of its greatest occlusion. Experience shows that a polyamide thread is less than a wire that irritates soft tissues and is easily removed after the end of the stretch, which is carried out through a rod mounted laterally into the gypsum cap.
Suspension of the zygomatic bone together with the maxilla can be accomplished either by the Ya. M. Zbarge's jawbone and extraoral device, or by an individually manufactured plastic maxillary bar with extraoral rods, or by the operational methods of Adams, Federspil or Adams-T. V. Chernyatina.
NA Shinbirev suggested fixing the cheek bone with the AA Limberg single-edged hook (which he corrected) to the head plaster bandage.
Methods of treatment of patients with isolated fractures of the zygomatic arch
In these cases, there are usually two fragments, lying freely and concave with their approximal ends inward. They are guided by different methods.
The Limberg-Bragin method
Single-tooth hook A. A. Limberg or a two-tooth hook Yu. E. Bragin is introduced through a puncture-cut in length 0.3-0.5 cm in the projection of the lower edge of the zygomatic arch. They move the fragments to the outside by pulling the hook under their inwardly displaced ends. If the fragments in the correct position are not displaced, the wound is sutured.
Suture on bone
In this case, the incision along the lower edge of the malar bone increases somewhat (up to 1.5-2 cm). This is necessary in cases when, after correcting the fragments of the arch, they again occupy an incorrect position with the formation of a diastase between the ends of the fragments. If the arc is wide enough, holes are made with a small fissure boron, a thin chrome-plated catgut or polyamide thread is drawn in them, they tighten the ends and thereby give the bone fragments the correct position.
Correction by wire loop according to the method Matas-Berini
Using a large bent needle Bassini conduct a thin wire in the thickness of the tendon of the temporal muscle, forming a loop-grip. Pulling the wire loop, fix the fragments in the correct position.
The choice of the method of repositioning and fixing fragments for fractures of the zygomatic bone and arch
Since the formation of bone tissue in fractures of the malar bone occurs metaplastic and ends on average in two weeks, it is advisable to divide them into fresh ones (up to 10 days from the moment of injury) and old ones (more than 10 days) to choose therapeutic tactics. By the same principle, it is possible to divide all the methods of correcting the fragments of the malar bone.
In the period up to 10 days after the injury, the treatment can be either conservative (non-operative) or surgical (radically operative), and after 10 days - only operative. The nature of surgical intervention is determined by the peculiarities of functional and cosmetic disorders caused by cicatricial fixation of bone fragments in the wrong position, as well as the experience of the surgeon, the availability of the necessary tools, equipment, etc. The ratio of the patient himself to the cosmetic defect that he develops proposal to undergo surgical intervention.
The choice of the method of surgical treatment of fresh fractures of the zygomatic bone or arch depends primarily on the type (localization) of the fracture, the number of fragments, the degree of their displacement and the presence of a tissue defect.
For chronic fractures (more than 10 days), bone fragments can be inserted by the most simple methods (finger method, Keen-Wielage incision, using the A. Limberg single-tooth hook or Yu. E. Bragin's two-tooth hook) usually fails. In such cases it is necessary to resort to more severe surgical interventions: either to use the apparatus of VA Malanchuk and PV Khodorovich, Yu. E. Bragin, or by exposing the site of the fracture with the help of intra- or extraoral access, to break formed scarring adhesions , to fasten the repaired fragments with a seam or mini-plate. One of the methods of fixation of the zygomatic bone and the lower wall of the orbit after correction is the method of tight tamponade of the maxillary sinus with the iodoform-gauze swab according to VM Gnevsheva, and OD Nemsadze and LI Hirseli (1989) as a support for the repaired zygomatic bones use a rod of canned allogeneity of the appropriate size, inserted into the sinus: one end of it rests against the zygomatic bone on its inner side, the other - in the lateral wall of the nose.
Outcomes of a fracture of the malar bone and zygomatic arch
In cases of timely and correct reposition and fixation of fragments with fresh fractures of the zygomatic bones and arches, complications are not observed.
If there is no correction, complications such as deformity of the face, persistent contracture of the lower jaw, visual impairment, chronic sinusitis, chronic osteomyelitis of the malar bone and upper jaw, impaired sensitivity, mental disorders, etc., may occur.
Deformation of the face is caused by a significant mixing or defect of the zygomatic bone (arc), not eliminated in the treatment of the victim.
OD Nemsadze, MN Kiviladze, AA Bregadze (1993) suggest, after establishing the degree of displacement of the zygomatic bone in the lateral zone (with an old or incorrectly intergrown fracture of the malar bone) with the aim of repositioning the bone fragments (after refractory fragments) In the region of the orbital wall of the orbit (in the area of the forehead-frontal suture), a newly formed bone of the appropriate size should be resected.
The contracture of the lower jaw can be caused by two reasons:
- the displacement of the zygomatic bone inside and back, followed by the fusion of its fragments in the wrong position;
- a rough cicatricial degeneration of the soft tissues surrounding the coronoid process of the lower jaw.
Especially often contracture develops with lesions 1, 3, 5-8 classes.
Chronic traumatic sinusitis occurs quite often: for example, in the so-called "cheek-jaw fractures" it is observed in 15.6% of the affected (VM Gnevsheva, 1968).
All these complications, and especially chronic traumatic osteomyelitis, arise as a result of open infected fractures of the malar bone, in the absence of timely and correct surgical treatment, repositioning and fixation. In this connection, the infection can spread to the maxillary bone, the mucous membrane of the maxillary sinus, conjunctiva, the cellular tissue of the eye, and soft facial tissues.