
Fracture of upper jaw
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
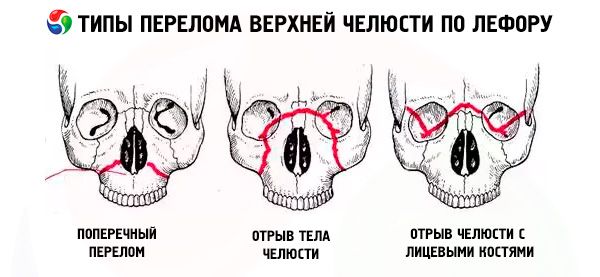
The fracture of the upper jaw usually passes through one of the three typical lines of least resistance described by Le Forus: the upper, middle and lower. They are called the lines of Le Fora (Le Fort, 1901).
- Le Fort I - the bottom line, has a direction from the base of the pear-shaped aperture horizontally and back to the pterygoid process of the sphenoid bone. This type of fracture is first described by Geren, he is mentioned in his work by Le Fort, and therefore a fracture along the lower line should be called the Geren-Le Fora fracture.
- Le Fort II - the middle line, runs transversely through the nasal bones, the bottom of the orbit, the infraorbital margin, and further down the cheek-jaw joint and pterygoid process of the sphenoid bone.
- Le Fort III - the upper line of the least strength, passing in the transverse direction through the base of the nasal bones, the bottom of the orbit, the outer edge of it, the zygomatic arch and the pterygoid process of the sphenoid bone.
In the case of a fracture along the Le Fort I line, only the dental arch of the upper jaw is mobile, along with the palatal process; with a fracture of the type Le Fort II - the entire upper jaw and nose, and in the case of a fracture of the type Le Fort III - the entire upper jaw along with the nose and cheekbones. This mobility can be one- and two-sided. With unilateral fractures of the upper jaw, the fragility mobility is less pronounced than with bilateral ones.
Fractures of the upper jaw, especially along the line of Le Fort III, are often accompanied by injuries to the base of the skull, concussions, bruises or compression of the brain. Simultaneous damage to the jaw and brain is more often the result of a severe and severe injury: a severe blow on the face, compression, falling of the victim from a high altitude. The condition of patients with a fracture of the upper jaw is greatly aggravated with damage to the walls of the paranasal sinuses, the nasal part of the pharynx, the middle ear, the meninges, the anterior cranial fossa with the injection of nasal bones into it, the walls of the frontal sinus. As a result of a fracture of the walls of this sinus or a latticed labyrinth, emphysema of the subcutaneous tissue in the area of the orbit, forehead, and cheek may appear, which is a characteristic symptom of crepitus. Often there is a crushing or rupture of the soft tissues of the face.
 [1],
[1],
Symptoms of a fracture of the upper jaw
Fractures of the base of the skull are accompanied by a symptom of "bloody glasses", subconjunctival suffusion (blood-pressure), retroauric hematoma (with a fracture of the middle cranial fossa), bleeding and especially cerebrospinal fluid from the ear and nose, disorders of the cranial nerves and obschevenrologicheskimi disorders. Most often, the branches of the trigeminal, facial and oculomotor nerves are damaged (loss of sensitivity, mimicry, pain when moving the eyeballs up or to the sides, etc.).
A high diagnostic value is the rate of development of hematomas: rapid - indicates its local origin, and slow - within 1-2 days - typical for indirect, deep bleeding, i.e. Fracture of the base of the skull.
Diagnosis of fractures of the upper jaw in comparison with injuries of the lower jaw represents a more difficult task, as they are often accompanied by a rapidly increasing edema of the soft tissues (eyelids, cheeks) and interstitial hemorrhages.
The most typical symptoms of a fracture of the upper jaw are:
- elongation or flattening of the middle part of the face due to displacement of the severed jaw downward or inward (backward);
- soreness when trying to close a tooth;
- malocclusion;
- bleeding from the nose and mouth.
The latter is especially pronounced in the case of fractures along the line of Le Fort III. In addition, often fractures of the upper jaw are nailed, so it is difficult to detect the main symptom of any bone fracture - the displacement of fragments and their pathological mobility. In such cases, the flattening of the middle third of the face, the bite and the step symptom, detected by palpation of the edges of the eye sockets, the zygomatic arches and the cheek-alveolar ridges (the junction of the zygomatic process of the maxilla and the maxillary process of the malar bone) can help diagnose it, and is caused by a violation of the integrity of these bone formations .
To increase the accuracy of diagnosis of fractures of the upper jaw, one should take into account the painfulness at palpation of the following points corresponding to areas of increased extensibility and compression of bones:
- upper nasal - at the base of the root of the nose;
- lower nasal - at the base of the septum of the nose;
- supraorbital - on the upper edge of the orbit;
- extraorbital - at the outer edge of the orbit;
- infraorbital - on the lower edge of the orbit;
- zygomatic;
- arc - on the zygomatic arch;
- tuberal - on the hill of the upper jaw;
- cheek-alveolar - above the area of the 7th upper tooth;
- canine;
- palatine (the points are palpable from the side of the mouth).
Symptoms of mobility of the fragments of the upper jaw and the "floating sky" can be revealed as follows: with the fingers of the right hand the doctor grasps the anterior group of teeth and the sky, and places the left hand on the cheeks from the outside; then produces easy rocking movements forward-down and back. When the fractures are punctured, the mobility of the fragment can not be determined in this way. In these cases it is necessary to palpate the pterygoid processes of the wedge-shaped bones; the patient usually feels pain, especially with fractures along the lines of Le Fort II and III, sometimes accompanied by a number of the aforementioned symptoms of a fracture of the base of the skull, trellis labyrinth, nasal bones, lower walls of the orbit and zygomatic bones.
In patients with injuries of the upper jaw and frontal bone, a fracture of the walls of the maxillary sinuses, the lower jaw and zygomatic bones, the latticed labyrinth and the septum of the nose is possible. Therefore, with combined fractures of the base of the skull, upper jaw, zygomatic bones, septum of nose and lacrimal bones intense tearing and liquorrhea from the nose and ears may appear.
The combination of fractures of the upper jaws with traumatic damage of other parts of the body in most cases is clinically manifested by a particularly severe syndrome of mutual burdening and overlapping. Patients with this combination should be referred to the category of victims with an increased risk of developing common septic complications, not only in the maxillofacial area, but also in other foci of damage to distant localization (as a result of metastatic infection), including those not closed, not having a direct anatomical connection with jaws, oral cavity, face.
In many patients with fractures of the upper jaws, there is a more or less pronounced traumatic neuritis of the infraorbital branches of the trigeminal nerve; In some cases, long-term electrical excitability of the teeth on the side of the trauma persists.
The detection of palpation of the uneven edges of the eye socket (step-like protrusions), the alveolar ridges, the naso-maxillary sutures, as well as the changes in the edges of the upper jaw with X-ray in the axial and frontal projections are of definite diagnostic significance.
Outcomes of jaw fractures
Outcomes of jaw fractures depend on many factors: the age and previous trauma of the general condition of the victim, the presence of the syndrome of mutual burdening, the ecological situation in the area where the victim permanently resides; in particular - on the presence of an imbalance of mineral elements in water and food (GP Ruzin, 1995). Thus, according to GP Ruzin, in the inhabitants of different regions of the Ivano-Frankivsk region the course of fractures and the nature of the metabolic processes studied are almost identical and can be considered optimal, and in the Amur region the process of bone tissue regeneration and metabolic reactions proceed more slowly. The frequency and nature of the complications depend on the period of adaptation of the individual in the area. The indicators used by him: the index of inflammatory reaction (IWR), the index of metabolism (MI), the index of regeneration (RI) allow analyzing a set of changes in the studied indicators even in cases when the changes of each of them do not go beyond physiological norms. Therefore, the use of indices of IWR, MI and RI makes it possible to predict the course of a fracture, the development of an inflammatory-infectious complication, to formulate a scheme for treating a patient with the aim of optimizing metabolic processes, preventing complications, and controlling the quality of treatment, taking into account the characteristics of the patient and external conditions. For example, for the Ivano-Frankivsk region, the critical values of the indices are: IWR - 0.650, MI - 0.400, RI - 0.400. When receiving lower figures, corrective therapy is necessary. Optimization of metabolism is not required if IVR> 0.6755, MI> 0.528, RI> 0.550. The author has established that in different regions the values of the indices can vary depending on the medical-geographical and biogeochemical conditions that must be taken into account when analyzing them. So, in the Amur region these values are lower than in Ivano-Frankivsk. That is why it is advisable to assess the IWR, MI and RI in combination with the clinical and radiological examination of the patient in the first 2-4 days after the trauma - to reveal the initial level of regenerative potencies and the necessary corrective therapy, on the 10th to the 12th day - for clarification conducted treatment, on the 20-22th day - to analyze the results of treatment and predict the characteristics of rehabilitation.
According to GP Ruzin, in regions with hypo- and discomforting conditions, the presence of an imbalance of mineral components and the amino acid composition of proteins in the period of adaptation, it is necessary to include anabolics and adaptogens in the treatment complex. Among all the same physical factors used, the most pronounced positive effect was exerted by laser radiation.
Based on his research practical recommendations, the author summarizes as follows:
- It is advisable to use tests that characterize the conditions of metabolism and reparative process: the index of inflammatory reaction (IWR), metabolic index (MI), regeneration index (RI).
- With an HDI below 0.675, the use of osteotropic antibiotics is required, with an HDI above 0.675, with timely and adequate immobilization, antibiotic-co-therapy is not indicated.
- At MI and RI values less than 0.400, therapy is necessary with the inclusion of a complex of drugs and drugs that stimulate protein and mineral metabolism.
- At low IWR indices, the use of local thermal procedures (UHF) is contraindicated prior to the resolution or drainage of the inflammatory focus.
- In the treatment of patients with fractures of the mandible in adverse medical and geographical conditions, especially during the period of adaptation, adaptogens, anabolics and antioxidants should be prescribed.
- In order to quickly resolve the infiltrate and reduce the duration of the pain syndrome, it is advisable to use laser irradiation in the first 5-7 days after injury.
- To optimize the treatment of patients with a fracture of the lower jaw, shortening the periods of hospitalization, it is necessary to organize rehabilitation cabinets and continuity at all stages of treatment.
With the provision of timely pre-medical, medical and specialized care, the outcomes of jaw fractures in adults are favorable. For example, VF Chistyakova (1980), using a complex of antioxidants to treat uncomplicated fractures of the mandible, was able to reduce the stay of patients in the hospital by 7.3 bed days, and V. V. Lysenko (1993) in the treatment of open fractures, i.e., known to be infected with the microflora of the oral cavity, using nitazol foam aerosol intraorally, reduced the percentage of traumatic osteomyelitis by 3.87 times, reducing the duration of antibiotic use. According to KS Malikov (1983), when comparing the x-ray picture of the process of reparative regeneration of the lower jaw with autoradiographic indices, a peculiar pattern is established in bone mineral metabolism: an increase in the intensity of incorporation of the radioactive isotope 32 P and 45 Ca into the bone regenerate of the injured lower jaw is accompanied by the appearance of X-ray calcification sites in the terminal fragments; the dynamics of absorption of radiopharmaceuticals proceeds in the form of two phases of the maximum concentration of labeled compounds of 32 P and 45 Ca in the trauma zone. As the fracture of the bone fragments occurs in fractures of the lower jaw, the intensity of inclusion of the isotopes 32 P, 45 Ca in the damage zone increases. The maximum concentrations of osteotropic radioactive compounds in the terminal regions of the fragments are observed on the 25th day after injury to the jaw. The accumulation of macro- and microelements in the terminal sections of the fragments of the lower jaw is of a phase nature. At the same time, the first increase in the concentration of mineral substances is observed on 10-25 days, the second on 40-60 days. In later terms of reparative regeneration (120 days), mineral metabolism in the fracture zone begins to gradually approach normal parameters, and by the 360th day it completely normalizes, which corresponds to the process of final reconstruction of the bone callus that connected the fragments of the lower jaw. The author has established that timely and correct anatomical comparison of fragments and their reliable operative fixation (for example, with a bone suture) leads to early (25 days) bone fusion of fragments of the lower jaw and restoration (after 4 months) of the normal structure of the newly formed bone tissue, and its study by biochemical and spectral research methods in comparison with morphological and autoradiographic data showed that the degree of saturation of microstructures of corn with mineral substances gradually increased With increasing maturity of bone tissue.
In case of untimely application of complex treatment, the mentioned above and other inflammatory complications (maxillary sinusitis, arthritis, migrating granuloma, etc.), the formation of false joints, the appearance of cosmetic facial disfigurement, the malfunction of chewing and speech, the development of other non-inflammatory diseases that require complex and long-term treatment.
With multiple jaw fractures in elderly and senile patients, delayed fusion, false joints, osteomyelitis, etc. Are often observed.
In a number of cases, the use of complex orthopedic structures is necessary for the treatment of posttraumatic complications in accordance with the nature of functional and anatomical and cosmetic disorders, as well as carrying out restorative operations (osteoplasty, refracture and osteosynthesis, arthroplasty, etc.).
Diagnosis of a fracture of the upper jaw
X-ray diagnosis of fractures of the upper jaw is often very complicated, since on the X-rays in the lateral projection, a layering of two maxillary bones is obtained. Therefore, the x-ray of the upper jaw is usually done only in one (sagittal) projection (a survey radiograph), while attention should be paid to the contours of the skaloalveolar ridge. the infraorbital margin and the borders of the maxillary sinuses. Breaking them (kinks and zigzags) indicates a fracture of the upper jaw.
With craniofacial separation (a fracture along the line of Le Fort III), the radiography of the facial skeleton in the axial projection is of great assistance in diagnosing. In recent years, also successfully used tomography and panoramic radiography.
In recent years, there have appeared such diagnostic technologies (computer, magnetic resonance imaging), which allow simultaneous diagnosis of damage to both the facial and the brain cranium. So, Y. Raveh et al. (1992), T. Vellemin, I. Mario (1994) divided fractures of the frontal, maxillary, latticed bones, orbit into two types and one subtype - (1a). To the first type they include frontal-naso-latticular and medial-orbital fractures without breaking the bones of the base of the skull. In subtype 1a, damage to the medial wall of the optic canal and compression of the optic nerve are also attached to this.
Type II includes frontal-naso-latticework and medial-orbital fractures involving the base of the skull; the internal and external parts of the facial and cerebral cranium with intracranial displacement of the posterior wall of the frontal sinus, the anterior part of the skull base, the upper wall of the orbit, the temporal and basic bones, the region of the Turkish saddle are damaged; there are ruptures of the dura mater. In this type of injury, there is a cerebrospinal fluid, a hernial protrusion of the brain tissue from the fracture of the fracture, a bilateral telecanthus is formed with the interstitial area spreading, the optic nerve is squeezed and damaged.
Such a detailed diagnosis of a complex craniocerebral trauma allows us to compare the bone fragments of the base of the skull and face simultaneously 10-20 days after the injury, which makes it possible to reduce the length of stay of the injured in the hospital and the number of complications.
What do need to examine?
How to examine?
Who to contact?
Assisting the victims with a trauma to the maxillofacial area
Treatment of patients with jaw fractures involves the restoration of their lost form and function as soon as possible. The solution of this task includes the following main stages:
- comparison of displaced fragments,
- fixing them in the correct position;
- stimulation of bone tissue regeneration in the fracture region;
- prevention of various kinds of complications (osteomyelitis, false joint, traumatic sinusitis, peri-osseous phlegmon or abscess, etc.).
Specialized care for jaw fracture should be given at the earliest possible time (in the first hours after injury), as timely repositioning and fixing of fragments provide more favorable conditions for bone regeneration and healing of damaged soft tissues of the oral cavity, and also help stop primary bleeding and prevent development complications of inflammatory nature.
The organization of assistance to victims with a trauma of the maxillofacial area should provide continuity of medical measures along the whole route of the victim from the scene to the medical institution with mandatory evacuation to the destination. The scope and nature of the assistance provided may vary depending on the situation at the scene of the incident, the disposition of medical posts and institutions.
Distinguish:
- first aid, which is directly on the scene, sanitary posts and carried out by the victims (in self-help or mutual assistance), a paramedic, a medical orderly;
- pre-medical care provided by a medical assistant or nurse with the goal of supplementing first aid measures;
- first medical assistance, which should be rendered within 4 hours from the time of injury, if possible; it is carried out by non-specialist doctors (in rural district hospitals, at medical stations, ambulance stations);
- qualified surgical care, which should be provided in medical institutions no later than 12-18 hours after injury;
- specialized care, which should be provided in a specialized institution within one day after the injury. The time limits for the provision of various types of assistance are optimal.
First aid at the scene
The favorable outcome of the treatment of injuries to the maxillofacial area depends to a large extent on the quality and timeliness of first aid. From its correct organization depends not only health, but sometimes the life of the victim, especially when bleeding or asphyxiation occurs. Often one of the main features of injuries of the maxillofacial area is the discrepancy between the type of the victim and the severity of the lesion. This feature needs to be paid attention of the population, conducting sanitary and educational work (in the Red Cross system, during classes on civil defense).
The medical service should pay much attention to training in first aid, especially in those industries where injuries are high (mining, agriculture, etc.).
When providing first aid to the victim with a trauma of the person at the scene , first of all, it is necessary to give a position warning asphyxiation, ie, to lay on his side, turning his head towards the wound or face down. Then, an aseptic dressing should be applied to the wound. In case of chemical burns of the face (acids or alkalis), immediate flushing of the burnt surface with cold water is necessary to remove the residues of the substances that caused the burn.
After first aid is provided at the scene (sanitary post), the victim is evacuated to a medical aid point where they are provided with first aid by the nursing staff.
Many patients with wounds of the maxillofacial area can independently reach medical posts located near the scene of the accident (health centers of factories, factories). Those injured who can not move independently are transported to medical institutions in compliance with the rules for preventing asphyxia and bleeding.
The first pre-medical care for injuries of the maxillofacial area can be provided by the average medical personnel called to the scene.
[9]
First aid
As well as urgent, the help on vital indications is rendered on a place of incident, on sanitary posts, in health posts, paramedic and feldshersko-obstetric points. Thus efforts should be directed first of all on a stop of a bleeding, the prevention of asphyxia and a shock.
The average medical personnel (dental technician, paramedic, midwife, nurse) must know the basics of the diagnosis of facial injuries, first aid elements and the peculiarities of the transportation of patients.
The amount of pre-medical care depends on the nature of the injury, the condition of the patient, the situation in which this assistance is provided, and the qualifications of these health professionals.
Medical personnel should find out the time, place and circumstances of the injury; examining the victim, put a preliminary diagnosis and perform a number of medical and preventive measures.
Fighting bleeding
The abundant network of blood vessels in the maxillofacial region creates favorable conditions for the occurrence of bleeding when the face is damaged. Bleeding can occur not only outward or into the oral cavity, but also into the depths of tissues (latent).
In case of bleeding from small vessels, it is possible to tampon the wound and apply a pressure bandage (unless it causes a threat of asphyxiation or a displacement of the fragments of the jaws). With the help of a pressure bandage, you can stop bleeding in most injuries of the maxillofacial area. In cases of injuring large branches of the external carotid artery (lingual, facial, maxillary, superficial temporal), temporary stop of bleeding with emergency care can be performed by finger pressure.
Prevention of asphyxiation and methods to combat it
First of all, it is necessary to correctly assess the patient's condition, drawing attention to the nature of his breathing and position. In this case, phenomena of asphyxiation can occur, the mechanism of which can be different:
- displacement of the tongue back (dislocation);
- closure of the lumen of the trachea with blood clots (obturation);
- compression of the trachea with hematoma or edematous tissue (stenotic);
- closure of the entrance to the larynx with a hanging rag of the soft tissues of the palate or tongue (valve);
- aspiration of blood, vomit, earth, water, etc. (aspiration).
To prevent asphyxia the patient should be seated, slightly tilting it forward and lowering his head down; with severe multiple injuries and with a loss of consciousness - lay on your back, turning your head in the direction of injury or sideways. If the injury allows, the patient can be laid face down.
The most common cause of asphyxia is the tongue lapping that occurs when the body of the lower jaw, especially the chin, is split, with double mental fractures. One of the effective methods to combat this (dislocation) asphyxiation is fixation of the tongue with a silk ligature or piercing it with a safety pin or hairpin. To prevent obstructive asphyxia, you should carefully inspect the oral cavity and remove blood clots, foreign bodies, mucus, food debris or vomit.
Anti-shock activities
These measures should first of all provide for the timely stopping of bleeding, the removal of asphyxia and the implementation of transport immobilization.
The fight against shock in the wounds of the maxillofacial area includes the whole complex of measures taken in cases of shock in case of damage to other areas of the body.
To prevent further infection of the wound, an aseptic (protective) gauze dressing (for example, an individual package) should be applied. It should be remembered that with fractures of the face, you can not tighten the bandage to avoid mixing fragments, especially with fractures of the lower jaw.
It is forbidden for the average medical personnel to apply seams to soft tissue injuries in case of any damage to the face. With open wounds in the maxillofacial area, including all jaw fractures within the dentition, the mandatory at this stage of care is the introduction of 3000 AE tetanus antiserum on Bezredko.
For transport immobilization, fixing bandages are imposed - a conventional gauze, a sling, a circular, rigid chin, or a standard transport bandage consisting of a chin sling and a soft head cap.
If the doctor does not have these standard remedies, he can apply the usual gauze (bandage) cap of Hippocrates in combination with a sling-like marlevinkintovoy bandage; However, in those cases when the patient is transported for a long distance to a specialized institution, it is more expedient to impose a gypsum wound dressing.
It is necessary to clearly fill the referral to the medical institution, indicating everything that has been done to the patient, and to ensure the correct way of transportation.
If you have a history of a patient for unconsciousness, examination, care, and transportation should only be done while lying down.
The equipment of the paramedic station should provide for everything necessary to provide first aid for the first time in case of trauma to the person, including feeding and quenching the thirst of the patient (drinker, etc.).
When mass casualties occur (as a result of accidents, disasters, etc.), it is very important that they be properly evacuated and transported by a medical assistant or nurse, that is, prioritizing the evacuation and determining the situation of the victims during transport.
[10]
First medical aid
The first medical aid is provided by the doctors of the regional, district, rural district hospitals, central hospitals; district and city medical health centers, etc.
The main task at the same time is to help with vital indications: fighting with bleeding, asphyxia and shock, checking, and if necessary - correcting or replacing previously applied bandages.
The fight against bleeding is carried out by bandaging the vessels in the wound or its tight tamponade. With massive bleeding from the "oral cavity," which can not be stopped by conventional methods, the doctor must perform an urgent tracheotomy and tightly tampon the oral cavity and pharynx.
In the case of the appearance of signs of suffocation, treatment measures are determined by the cause that caused it. With dislocation asphyxia, stitch the tongue. A thorough examination of the oral cavity and the removal of blood clots and foreign bodies eliminate the threat of obstructive asphyxia. If, despite these measures, asphyxia nevertheless developed, an urgent tracheotomy is indicated .
The anti-shock measures are carried out according to the general rules of emergency surgery.
Then, with jaw fractures, you must always apply a fixative bandage for transport (temporary) immobilization and water the patient in the usual way or with the help of a drinker with a rubber tube on the nose.
Methods of temporary fixation of jaw fragments
Currently, there are the following methods of temporary (transport) immobilization of jaw fragments:
- chinstrap dressings;
- sling-like gypsum or band-aid;
- intermaxillary binding by wire or plastic thread;
- standard kit and others. For example, the continuous connection of the figure-eight, the tongue-labial connection, the ligature of Yu. Galmosha, the continuous wire ligature according to Stout, Ridson, Obvegzer, Elenka, well described by Yu. Galmosh (1975).
The choice of the method of temporary immobilization of fragments is determined by the localization of fractures, their number, the general condition of the affected person and the presence of sufficiently firm teeth to fix the tire or bandage.
In fracture of the alveolar process of the upper or lower jaw, after comparing the fragments, an external gauze dressing is used, pressing the lower jaw to the upper jaw.
For all fractures of the body of the upper jaw, after repositioning the fragments on the upper jaw, a metal spoonful of A. A. Limberg is put on, or a bandage bandage is placed on the lower jaw.
In the absence of teeth of the upper jaw, a gasket from the stance or wax is placed on the gums.
If the patient's mouth has dentures, they are used as a strut between the dental arches and an additional sling dressing is applied. In the front part of the plastic dentition, you need to make a hole for the spout of an appetizer, a drainage tube or a teaspoon to make it possible for the patient to eat.
If both jaws have teeth, then with fractures of the body of the lower jaw, the fragments are strengthened with an intermaxillary ligature bandage, a stiff standard sling or a gypsum lint. Which is imposed on the lower jaw and attached to the cranial vault.
In fractures in the area of condylar processes of the lower jaw, an intraoral ligature or a rigid bandage with an elastic pull to the head cap of the victim is used. In cases of fractures of condylar processes with malocclusion (open), the lower jaw is fixed by means of a spacer between the last antagonizing large molars. If there are no teeth on the injured lower jaw, you can use prostheses in combination with a stiff sling; if there are no prostheses, apply a hard sling or a gauze bandage.
When combined fractures of the upper and lower jaws apply the above described methods of separate fixation of fragments, for example, a spoonful of Rauer-Urbanskaya in conjunction with ligature binding between teeth at the ends of the fragments of the lower jaw. Ligature should cover in the form of eight on two teeth on each fragment. If there is no threat of intra-uterine bleeding, tongue twisting, vomiting, etc., you can apply a hard sling.
At the stage of rendering the first medical assistance, it is necessary to correctly resolve the issue of the timing and mode of transportation of the victim, to determine, if possible, the evacuation purpose. In the presence of complicated and multiple fractures of a person's bones, it is advisable to reduce the number of "evacuation stages" to a minimum, directing such patients directly to the stationary maxillofacial departments of republican, regional and regional (city) hospitals and hospitals.
When combined trauma (especially trauma to the skull), the issue of transportation of the patient should be handled carefully, carefully and in conjunction with appropriate specialists. In these cases, it is more expedient to call specialists of oblast or city institutions to consult a rural district hospital than to transport patients with concussion or brain contusion there.
In the presence of a dentist in the district hospital, the first medical help in conditions such as non-penetrating damage to the soft tissues of the face, which do not require the production of primary plasty, fractures of the teeth, fractures of the alveolar processes of the upper and lower jaw, uncomplicated single fractures of the mandible without mixing, fractures of the bones of the nose , which do not require correction, dislocations of the lower jaw that managed to be fixed, burns of the face of I-II degree, can be supplemented with elements of specialized care.
Patients with combined trauma to the face, especially if there is a concussion of the brain, should be hospitalized in the district hospitals. When deciding on their transportation in the first hours after injury to specialized departments, the general condition of the patient, the mode of transport, the condition of the road, the distance to the medical institution should be taken into account. The most suitable mode of transport for these patients can be considered a helicopter and, with good road conditions, specialized ambulances.
After the first medical aid in the district hospital of patients with fractures of the upper and lower jaws, multiple trauma of the bones of the face complicated by trauma of any localization, penetrating and extensive damages of soft tissues requiring primary plasty are sent to specialized departments of the regional, city or regional hospital. The question of where the patient should be sent to the district hospital (if there are dentists there) or to the maxillofacial department of the nearest hospital, is decided depending on local conditions.
Qualified surgical care
Qualified surgical care is provided by surgeons and traumatologists in polyclinics, at trauma centers, in surgical or trauma departments of city or district hospitals. It should be provided primarily to those affected who need it according to vital indications. These include patients with signs of shock, bleeding, acute blood loss and asphyxia. For example, if unidentified at previous stages or bleeding from the large vessels of the maxillofacial region fails to reliably bind the bleeding vessel, then the external carotid artery is bandaged on the corresponding side. At this stage, all the victims with injuries to the maxillofacial area are divided into three groups.
The first group - requiring only surgical care (wounds of soft tissues without true defects, burns of I-II degree, frostbite of the face); for them this stage of treatment is final.
The second group is in need of specialized treatment (wounds of soft tissues, requiring surgical processing of plastic elements, damage to the bones of the face, burns of III-IV degree and frostbite of the face requiring surgical treatment); after providing emergency surgical care, they are transported to the maxillofacial hospitals.
The third group is non - transportable victims, as well as persons with combined injuries of other areas of the body (especially craniocerebral trauma), which in their severity are leading.
One of the reasons for re-surgical treatment of the wound is an intervention without a preliminary radiographic examination. If it is suspected that the bones of the face are fractured, it is mandatory. The increased regenerative capacity of the facial tissues allows surgical intervention, sparing the tissues as much as possible.
When providing qualified surgical care to the victims of the II group who will be sent to specialized medical institutions (if they do not have contraindications for transportation), the surgeon must:
- to produce prolonged anesthesia of the fracture site; and even better - prolonged analgesia of the entire half of the face, or according to the method of P. Yu. Stolyarenko (1987): through a needle prick under the bone ledge on the lower edge of the zygomatic arch at the junction of the temporal process of the malar bone with the zygomatic process of the temporal bone;
- to cut the wound with antibiotics, to inject antibiotics inwards;
- to carry out the simplest transport immobilization, for example, to impose a standard transport bandage;
- to be convinced of absence of a bleeding from a wound, asphyxia or its threat at transportation;
- monitor the administration of tetanus antiserum;
- ensure proper transportation to a specialized medical institution, accompanied by medical personnel (determine the mode of transport, the patient's situation);
- clearly indicate in the accompanying documents everything that is done to the patient.
In cases where there are contraindications to the direction of the victim in another medical institution (group III), he is provided with qualified assistance in the surgical department with the involvement of dentists at hospitals or clinics that are required
General surgeons and traumatologists, in turn, should be familiar with the basics of assisting in the trauma of the maxillofacial area, observe the principles of surgical treatment of the wounds of the face, know the basic methods of transport immobilization of fractures.
Treatment of victims with combined injuries of the face and other areas in the surgical (trauma) hospital should occur with the participation of the maxillofacial surgeon.
If there is a maxillofacial department or dental office in the district hospital, the head of the department (dentist) should be responsible for the condition and organization of trauma dental care in the district. To properly take into account maxillofacial injuries, contact of the dentist with feldsher's points and district hospitals should be established. In addition, it is necessary to analyze the results of treatment of patients with trauma of a person who were in district and regional institutions.
The direction to the maxillofacial department is subject to patients with complex and complicated injuries of the face when it is necessary to carry out the primary plastic surgery of soft tissues and apply the newest methods of treating facial bone fractures, including primary bone plasty.
Specialized emergency care and subsequent treatment of an upper jaw fracture
This type of care is provided in the stationary maxillofacial departments of the republican, regional, regional, city hospitals, in clinics of surgical dentistry of medical universities, research institutes of stomatology, in the maxillofacial departments of research institutes of traumatology and orthopedics.
When admitting victims to the inpatient department of the hospital, it is expedient to distinguish three sorting groups (according to VI Lukyanenko):
The first group - in need of urgent measures, in qualified or specialized care in dressing or operating: wounded in the face with continued bleeding from under bandages or oral cavity; Those who are in a state of asphyxia or with unstable external respiration, after a tracheotomy with a tight tamponade of the oral cavity and pharynx, are in an unconscious state. They are sent to the operating room or dressing room on stretchers first.
The second group - who need to clarify the diagnosis and determine the lead in the severity of damage. These include the wounded with combined injuries of the jaws and face, ENT organs, skulls, organs of vision, etc.
The third group is to be sent to the department in the second turn. This group includes all victims who are not included in the first two groups.
Before the beginning of surgical treatment the victim should be examined clinically and radiological. Based on the data obtained, the extent of the intervention is determined.
Surgical treatment, regardless of whether it is early, delayed or late, should be one-stage and, if possible, complete, include local plastic surgery on soft tissues and even bone plastic of the lower jaw.
As indicated by AA Skager and TM Lurie (1982), the nature of the regenerative blastema (osteogenic, chondrogenic, fibrous, mixed) is determined by the oxybiotic activity of tissues in the fracture zone, and therefore all traumatic and therapeutic factors affect the speed and quality of reparative osteogenesis mainly through local blood supply. As a result of damage, there are always violations of the circulation of the local (wound and fracture area), regional (maxillofacial area) or general (traumatic shock) character. Local and regional circulatory disorders are usually more prolonged, especially in the absence of immobilization of fragments and the occurrence of inflammatory complications. As a result, the reparative reaction of tissues is distorted.
With adequate blood supply to the damage zone, in conditions of fragility stability, a primary, so-called angiogenic formation of bone tissue occurs . In less favorable vascular-regeneration conditions, which are created mainly in the absence of stability in the area of joints of fragments, a connective tissue or cartilaginous regenerate is formed, ie, "reparative osteosynthesis" occurs, especially when there is no timely and correct comparison of the fragments. Such a course of reparative regeneration requires more tissue resources and time. It may result in secondary bone fracture fusion, but at the same time, scar tissue with chronic inflammation foci, which can manifest clinically in the form of exacerbation of traumatic osteomyelitis, is sometimes permanently retained or permanently left in the fracture zone .
From the point of view of optimization of the vascular-regeneration complex, closed reposition and fixation of fragments of the facial bones have the advantage over open osteosynthesis with wide exposure of the ends of the fragments.
Therefore, the following principles are based on the modern treatment of bone fractures:
- ideally accurate comparison of fragments;
- Bringing the fragments along the entire surface of the fracture to the position of close contact (cohesion);
- a strong fixation of reponated and fractured fracture surfaces, which excludes or almost excludes any visible mobility between them for the entire period necessary for the complete fusion of the fracture;
- preservation of mobility of temporomandibular joints, if the surgeon has an apparatus for extraoral reposition and fixation of fragments of the lower jaw.
This ensures faster fusion of bone fragments. Observance of these principles ensures the primary fusion of the fracture and allows to shorten the period of treatment of patients.
Additional general and local treatments with fresh fractures complicated by inflammation
Specialized care for maxillofacial lesions involves a set of measures aimed at preventing complications and accelerating the regeneration of bone tissue (physiotherapy, physiotherapy, vitamin therapy, etc.). It should also provide all patients with the necessary nutrition and proper oral care. In large departments it is recommended to allocate special wards for traumatological patients.
With all types of care, you need to clearly and correctly fill out medical records.
Measures that prevent the development of complications include the introduction of tetanus antitetanus, local administration of antibiotics in the preoperative period, sanitation of the oral cavity, temporary immobilization of fragments (within the limits of possible). It should be remembered that infection with fractures within the dentition can occur not only when the mucous membrane is broken or the skin is damaged, but also in the presence of peri-vertebral inflammatory foci of teeth located in the fracture region or in the immediate vicinity of it.
If necessary, in addition to imposing a standard transport dressing, intermaxillary fixation is performed with the help of ligature binding of teeth.
The method of anesthesia is chosen depending on the situation and the number of patients admitted. In addition to the general condition of the patient, it is necessary to take into account the localization and character of the fracture, as well as the time that it is supposed to spend on orthopedic fixation or osteosynthesis. In most cases, fractures of the body and the jaw branch (with the exception of high condylar fractures accompanied by dislocation of the mandible head) can be limited to local conductor and infiltration anesthesia. Conducting anesthesia is best performed in the area of the oval aperture (if necessary from both sides) to turn off not only the sensitive but also the motor branches of the mandibular nerve. More potent local anesthesia is more effective. An extended conductive blockade is also used, and a combination thereof is used with calypsoal in subnarcotic doses.
To solve the problem of how to deal with a tooth directly in the fracture, it is necessary to determine the ratio of its roots to the plane of the fracture. There are three possible positions:
- The crack of the fracture runs along the entire lateral surface of the root of the tooth - from its neck to the apex opening;
- in the crack of the fracture is the tip of the tooth;
- the fracture of the fracture passes obliquely with respect to the vertical axis of the tooth, but outside its alveoli, without damaging the periodontal and the walls of the alveolus of the tooth.
The third position of the tooth is most favorable from the point of view of the consolidation forecast (without the development of a clinically noticeable inflammatory complication), and the least - the first, as there is a rupture of the mucous membrane of the gum in the tooth's neck and the gaping fracture gap, causing inevitable infection of the jaw fragments with a pathogenic microflora oral cavity. Therefore, even before immobilization it is necessary to remove teeth in the first position, as well as broken, dislocated, fractured, destroyed caries, complicated pulpitis or chronic periodontitis. After tooth extraction it is recommended to isolate the fracture zone by plugging the hole with iodine gauze. NM Gordiyuk and co-authors. (1990) recommend tampon the wells with canned (in 2% chloramine solution) amnion.
It is very important to determine the nature of the microflora in the fracture region and to investigate its sensitivity to antibiotics. Intact teeth located in the second and third positions can be provisionally left in the fracture, but in this case the complex treatment should include antibiotic and physiotherapy. If, in the process of such treatment, the first clinical signs of inflammation in the fracture zone appear, the left tooth is treated conservatively, the canals of its roots are sealed, and if they are obstructed, they are removed.
Tooth germs, the teeth with unformed roots and has not erupted teeth (in particular, the third large indigenous) in the absence of around inflammation can also be conventionally left in the field of crisis because, in our experience and observations of other authors, well-being in the zone left in the gap a fracture of the teeth clinically determined on the day of patient discharge from the hospital is often deceptive, unstable, especially in the first 3-9 months after the trauma. This is due to the fact that sometimes the pulp of bicorny teeth located in the fracture zone, accompanied by damage to the mandibular vascular bundle, is subjected to profound inflammatory-dystrophic changes resulting in necrosis. When the neurovascular bundle of a single-root tooth is damaged, necrotic pulp changes are observed in most cases.
According to the data of different authors, preservation of teeth in the fracture is possible only in 46.3% of patients, as the rest develop periodontitis, bone resorption, osteomyelitis. At the same time, dental rudiments and teeth with incompletely formed roots, preserved under the condition of absence of signs of inflammation, have high viability: after a reliable immobilization of fragments, the teeth continue to develop (in 97%) and dare to erupt in a timely manner, and their electroexcitability in the long-term periods is normalized. Teeth that have been re-implanted into the fracture fracture die on average in half of the patients.
In the presence of, in addition to damage to the maxillofacial region, concussions or bruises of the brain, violations of the function of the circulatory system, respiratory and digestive systems, etc., take the necessary measures and prescribe the appropriate treatment. It is often necessary to resort to consultations of various specialists.
Due to the anatomical connection of the bones of the cerebral skull and face, all the structures of the cerebral part of the skull suffer from a trauma of the maxillofacial region. The strength of the acting factor in its intensity usually exceeds the limit of elasticity and strength of individual bones of the face. In such cases, neighboring and deeper parts of the facial and even cerebral part of the skull are damaged.
The peculiarity of the combined trauma of the face and brain is that damage to the brain can also occur in the absence of a stroke in the brain area of the skull. The traumatic force that caused the fracture of the facial bones is transmitted directly to the nearby brain, causing neurodynamic, pathophysiological and structural changes in it to varying degrees. Therefore, combined damage to the maxillofacial region and the brain can be caused by the impact of the traumatic agent only on the facial part of the skull, or on the facial and cerebral sections of the skull at the same time.
Clinically closed craniocerebral injury is manifested by cerebral and local symptoms. To general cerebral symptoms include loss of consciousness, headache, dizziness, nausea, vomiting, amnesia, and to local - a violation of the cranial nerves. All patients with an indication of an anamnesis for concussion of the brain need complex treatment together with a neurosurgeon or neuropathologist. Unfortunately, concussion of the brain, combined with a trauma to the bones of the face, is usually diagnosed only in cases with pronounced neurologic symptoms.
Complications of jaw fracture, prevention and treatment
All complications arising on the basis of fractures of the jaws can be divided into general and local, inflammatory and non-inflammatory; in time they are divided into early and distant (later).
By common early complications include violations of the psycho-emotional and neurological status, changes in the circulatory system and other systems. Prevention and treatment of these complications are performed by maxillofacial surgeons in conjunction with appropriate specialists.
Among local early complications, dysfunction of the masticatory apparatus (including temporomandibular joints), traumatic osteomyelitis (in 11.7% of the affected), hematoma suppuration, lymphadenitis, arthritis, abscesses, phlegmon, sinusitis, delayed consolidation of fragments, etc. Are most often observed.
To prevent possible general and local complications, it is advisable to carry out novocaine trigemino-sympathetic and sino-carotid blockades, which make it possible to turn off the cerebral reflexogenic zones, so that the liquorodynamics, respiration, and cerebral circulation are normalized.
Trigemino-sympathetic blockade is performed according to the well-known technique of MP Zhakova. Sinocarotid blockade is carried out as follows: under the back of the victim lying on his back, at the level of the blades lay a roller, so that the head was slightly thrown back and turned in the opposite direction. On the inner edge of the sternocleidomus muscle, 1 cm below the level of the upper edge of the thyroid cartilage (projection of the carotid sinus), the needle is injected. As the needle moves in, novocaine is injected. When the fascia of the neurovascular bundle is punctured, a certain resistance is overcome and a ripple of the carotid sinuses is felt. Enter 15-20 ml of 0.5% p-ro novocaine.
Given the increased risk of septic complications in patients with damage to the maxillofacial region, brain and other areas of the body, it is necessary to appoint massive doses of antibiotics (after intradermal testing for individual tolerance) already in the first day after admission to the hospital.
When complications arise from the respiratory organs (which are often the cause of death of such patients), hormonotherapy and dynamic radiographic observation (with the involvement of appropriate specialists) are shown. Specialized care for such patients should be provided by the maxillofacial surgeon immediately after removal of the victims from shock, but not later than 24-36 hours after injury.
Various kinds of local and general adverse factors (infection of the oral cavity and destroyed teeth, crushing of soft tissues, hematoma, insufficiently rigid fixation, depletion of the patient due to disruption of normal nutrition, psycho-emotional stress, disorders of the nervous system, etc.) contribute to occurrence of inflammatory processes. Therefore, one of the main points of treatment of a victim is to stimulate the healing process of a jaw fracture by increasing the regenerative abilities of the patient's body and preventing inflammation in the area of injury.
In recent years, in connection with the increased resistance of staphylococcal infection to antibiotics, the number of inflammatory complications in injuries to the bones of the face increases. The greatest number of complications in the form of inflammatory processes occurs with fractures localized in the angle of the lower jaw. This is due to the fact that the chewing muscles located on both sides of the fracture region are reflexively refracted, penetrate into the gap and are trapped between the fragments. As a result of the fact that the mucosa of the gum is closely welded to the periosteum of the alveolar process and is broken at the slightest mixing of the fragments, a gaping inlet gate is constantly formed for the infection, through which pathogenic microorganisms, saliva, sloughing epithelial cells and food masses. With swallowing movements, the muscle fibers contracted by fragments are shortened, as a result of which saliva enters the depth of the bone gap actively.
Evidence of increasing inflammation of the bone and soft tissues are usually rapidly occurring skin hyperemia, tenderness, infiltration, etc.
The development of complications is facilitated by such factors as periodontitis (in 14.4% of patients), delayed hospitalization and untimely rendering of specialized care, elderly patients, chronic comorbidities, bad habits (alcoholism), decreased reactivity of the body, improper diagnosis and choice of treatment method, disorders functions of the peripheral nervous system, resulting from a fracture (damage to the branches of the trigeminal nerve), etc.
An important factor inhibiting the consolidation of jaw fragments is traumatic osteomyelitis, which, along with other inflammatory processes, especially occurs when the reposition and immobilization of fragments were carried out at a later date.
It is necessary to take into account that as a result of any trauma around the wound an inflammatory reaction develops. Regardless of the nature of the damaging agent (physical, chemical, biological), the pathogenetic mechanisms of the developing inflammatory process are of the same type and are characterized by a disturbance of the state of microcirculation, oxidation-reduction processes and the action of microorganisms in damaged tissues. For injuries neiz tachometric is bacterial contamination of the wound. The severity of the purulent-inflammatory process depends on the characteristics of the causative agent of the infection, the immunobiological state of the patient's organism at the time of introduction of the pathogen, on the degree of vascular and metabolic tissue disorders at the site of injury. The stability of damaged tissues sharply decreases to a purulent infection, conditions are created for the propagation of the pathogen and the manifestation of its pathogenic properties, which cause an inflammatory reaction and exert a destructive effect on the tissue.
At the site of the damaging factor, optimal conditions are created for the activation of proteolytic enzymes released from microorganisms, affected tissues, leukocytes, and the formation of inflammatory mediators - histamine, serotonin, kinin, heparin, activated proteins, etc., which cause microcirculation, transcapillary exchange, coagulation of blood. Tissue proteases, the products of microbial activity, contribute to the disturbance of oxidation-reduction processes, the dissociation of tissue respiration.
Accumulation as a result of this under-oxidized products, the development of tissue acidosis leads to secondary disorders of microhemodynamics in the lesion focus, the development of local avitaminosis.
Especially severe damages in tissue regeneration processes are noted when C-vitamin deficiency occurs in them , leading to inhibition of collagen synthesis of connective tissue and wound healing; while the content of vitamin C in sluggish granulations of infected wounds is significantly reduced.
In any trauma, a significant place in the limitation of the inflammatory process is given to the haemostatic reaction, since the formation of the fibrin layer and the deposition of toxic substances and microorganisms on its surface hinders the further spread of the pathological process.
Thus, with purulent complications of injuries, a closed chain of pathological processes occurs that promote the spread of infection and prevent healing of wounds. Therefore, the early use of various biologically active drugs that have anti-inflammatory, antimicrobial, antihypoxic and stimulating reparative effects processes is pathogenetically justified in order to reduce purulent complications and increase the effectiveness of complex treatment.
The Kiev Research Institute of Orthopedics, Ministry of Health of Ukraine, carried out research on the mechanism of action of biologically active substances and recommended for use in pyoinflammatory diseases amben, galascorbine, Kalanchoe, propolis.
Unlike natural inhibitors of proteolysis (trisilol, kontrikal, iniprol, tsolola, gordoksa, pantripina) ambene easily penetrates through all cell membranes and can be applied topically in the form of 1% solution, intravenously or intramuscularly at 250-500 mg every 6-8 hours. Within 24 hours the drug is excreted by the kidneys unchanged. With topical application, it penetrates well into tissues and within 10-15 minutes completely neutralizes tissue fibrinolysis of damaged tissues.
In pyoinflammatory complications of jaw fractures, amoxiclav, a combination of clavulanic acid with amoxicillin, is administered successfully , which is administered intravenously by 1.2 g every 8 h or orally 375 mg 3 times a day for 5 days. Patients who underwent a routine procedure, the drug is administered intravenously, 1.2 g 1 time per day, or orally in the same doses.
The biological activity of galascorbine is much higher than that of ascorbic acid due to the presence of ascorbic acid in the preparation in combination with substances possessing P-vitamin activity (polyphenols). Halasorbine promotes the accumulation of ascorbic acid in organs and tissues, thickens the vascular wall, stimulates wound healing processes, accelerates the regeneration of muscle and bone tissue, normalizes oxidation-reduction processes. Galaskorbin is administered orally 1 g 4 times a day; locally - in 1-5% freshly prepared solutions or in the form of 5-10% ointment.
Propolis contains 50-55% of vegetable resins, 30% of wax and 10-18% of essential oils; it contains various balsams, it contains cinnamic acid and alcohol, tannins; It is rich in microelements (copper, iron, manganese, zinc, cobalt, etc.), antibiotic substances and vitamins of groups B, E, C, PP, P and provitamin A; has an analgesic effect. Its antibacterial effect is most pronounced. The antimicrobial properties of propolis have been established with respect to a number of pathogenic gram-positive and gram-negative microorganisms, with the ability to raise the sensitivity of microorganisms to antibiotics, to change the morphological, cultural and tinctorial properties of various strains. Under the influence of propolis wounds are quickly cleared of purulent and necrotic cover. It is used as an ointment (33 g propolis and 67 g lanolin) or sublingually - in the form of tablets (0.01 g) 3 times a day.
To prevent complications of inflammatory nature and stimulation of osteogenesis, other measures are recommended. Some of them will be given below:
- The introduction of antibiotics (taking into account the sensitivity of the microflora) in the soft tissues surrounding the open fracture area, starting from the first day of treatment. Local administration of antibiotics can reduce the number of complications by more than 5 times. With the introduction of antibiotics in later periods (on the 6th-9th day and later), the number of complications does not decrease, but the elimination of the already developed inflammation is accelerating.
- Intramuscular administration of antibiotics in the presence of indications (increasing infiltration, increase in body temperature, etc.).
- Local UHF therapy from the 2nd to the 12th day of the trauma (10-12 min daily), the total quartz irradiation from the 2nd to the 3rd day (about 20 procedures), calcium chloride electrophoresis on the fracture region - from 13 -14th day before the end of treatment (up to 15-20 procedures).
- Assign inside multivitamins and 5% calcium chloride solution (one tablespoon three times a day, washed down with milk); Especially ascorbic acid and thiamine are especially useful.
- In order to accelerate the consolidation of fragments OD Nemsadze (1991) recommends additionally the following medicines: anabolic steroid (for example, nebol per os, 1 table 3 times a day, for 1-2 months, or retabolyl 50 mg intramuscularly 1 time per week for 1 month); sodium fluoride 1% rr, 10 cap. 3 times a day for 2-3 months; protein hydrolyzate (hydrolysin, casein hydrolyzate) for 10-20 days.
- In order to reduce spasm of blood vessels in the fracture zone (which, according to AI Eliashev (1939), lasts 1-1.5 months and inhibits bone formation), and to accelerate the consolidation of fragments, OD Nemsadze (1985) offers in 3 days After trauma intramuscularly inject spasmolytic drugs (gangleron, dibazol, papaverine, trental, etc.) for 10-30 days.
- Intramuscular injection of lysozyme 100-150 mg twice a day for 5-7 days.
- The use of a complex of antioxidants (tocopherol-acetate, flacumine, ascorbic acid, cysteine, eleutherococcus extract or acetaminophen.
- The use of local hypothermia by the method described by AS Komok (1991), provided that a special device for local hypothermia in the maxillofacial area is used; allows to ensure the temperature regime of injured tissues, including the mandibular bone, in the + 30 ° C mode - + 28 ° C; due to the balanced cooling of tissues with the help of the outer and intraoral chambers, the temperature of the refrigerant circulating in them can be lowered to + 16 ° C, which makes the procedure well tolerated and allows it to continue for a long time. AS Komok points out that a decrease in the local temperature of the tissues in the zone of fracture of the lower jaw to levels: on the skin +28 ° C, the mucous membrane of the cheek + 29 ° C and the mucosa of the alveolar process of the mandible + 29.5 ° C - elimination of venous congestion, puffiness, prevents the development of hemorrhages and bruises, eliminates pain reactions. The layered, uniform, moderate hypothermia of tissues in the cooling mode + 30 ° C - + 28 ° C within the next 10-12 hours after the double-jaw immobilization in combination with the medicament means allows us to normalize the blood flow in the tissues by the third day, eliminate the temperature responses and inflammatory phenomena , causes a pronounced analgesic effect.
At the same time, AS Komok stresses the complexity of this method, since, according to him, only a complex of electrophysiological techniques, including electrothermometry, rheography, rheodermatometry and electro-algasimetry, allows us to objectively assess the blood flow, heat transfer and innervation in injured tissues and the dynamics of changes in these indicators under the influence of ongoing treatment.
According to VP Korobov et al. (1989), correction of metabolic shifts in the blood in fractures of the lower jaw can be achieved either by a ferramid or, more effectively, by a coamid, which facilitates the acceleration of bone fragments coalescence. In case of development of acute traumatic osteomyelitis, the abscess is opened, the fracture gap is washed; desirable and fractional autohemotherapy - reinfusion UV-irradiated blood 3-5 times along with active anti-inflammatory antiseptic therapy according to the generally recognized scheme; in the stage of chronic inflammation it is recommended to activate bone regeneration according to the scheme: levamisole (150 mg orally once a day for 3 days, break between cycles - 3-4 days, 3 cycles), or T-activein subcutaneously (0.01% 1 ml for 5 days), or the action of a helium-neon laser on the biologically active points of the face and neck (10-15 seconds per point with a light output of no more than 4 mW for 10 days). After the onset of stiffness in the fracture zone, dosed mechanotherapy and other general biological effects were prescribed. According to the authors, the duration of treatment in the hospital is reduced by 10-12 days, and temporary incapacity for work - for 7-8 days.
For the prevention or treatment of traumatic osteomyelitis of the jaws, many other means and methods have been proposed, for example, demineralized bone suspension, "Nitazol" aerosol, staphylococcal anatoxin with autocrine, vacuum aspiration of fracture fracture and washing of bone wound under pressure with a 1% solution of dioxygen; immunocorrecting therapy. EA Karasyunok (1992) reports that he and his co-workers in the experiment studied and clinically proven the expediency of using against a background of rational antibiotic therapy 25% solution of acetamine inside 20 ml 2 times a day for 10-14 days, as well as scoring the area fracture by the apparatus of USPK-7H in the continuous labile mode, introduction by electrophoresis of a 10% solution of lincomycin hydrochloride. The use of this technique led to a reduction in complications from 28% to 3.85% and a reduction in temporary incapacity for work of 10.4 days.
R. 3. Ogonovsky, IM Got, OM Syria, I. Ya. Lomnitsky (1997) recommend the use of cellular xenobrefotransplantation in the treatment of long-term healing fractures of the jaws. To do this, a suspension of devitalized bone marrow cells of 14-day embryos is inserted into the fracture slit. On day 12-14 the authors observed a thickening of the periosteal-bone callus, and on the 20-22 day - the onset of persistent consolidation of the fracture, which had not been consolidated for 60 days of immobilization. The method allows you to get rid of repeated surgical interventions.
Domestic and foreign literature abounds with other proposals, which, unfortunately, are still available only to doctors working in clinics well equipped with the necessary equipment and medicines. But every doctor should be aware of the presence of other, more accessible means of preventing complications in the treatment of fractures of the bones of the face. For example, one should not forget that such a simple procedure as calcium chloride electrophoresis (the introduction of 40% of the solution from the anode at a current of 3 to 4 mA) promotes the rapid compaction of the formed callus. If the fracture is complicated by inflammation, in addition to antibiotic therapy, it is advisable to use an alcohol-novocain blockade (0.5% of novocaine in 5% alcohol). Complex treatment according to the described scheme allows to shorten the periods of immobilization of fragments for 8-10 days, and for fractures complicated by an inflammatory process, for 6-8 days.
A significant reduction in the length of hospitalization, we observed when introducing osteogenic cytotoxic serum (stimoblast) 0.2 ml in the isotonic sodium chloride solution (1: 3 dilution) into the fracture region. Serum was administered on the 3rd, 7th, 11th day after the injury.
Some authors recommend to include in the complex treatment of UHF and UHF therapy in combination with general ultraviolet irradiation and calcium chloride electrophoresis to accelerate the consolidation of jaw fragments, and VP Pyurik (1993) - to apply an interbranch introduction of the patient's bone marrow cells 1 mm 3 cells per 1 cm 2 of bone fracture surface).
Proceeding from the mechanism of development of inflammatory complications of fractures in the area of corners of the lower jaw, for their prevention, early immobilization of bone fragments in combination with targeted anti-inflammatory drug therapy is necessary . In particular, after treatment of the oral cavity with a solution of furacilin (1: 5000), infiltration anesthesia should be performed in the fracture region of 1% p-rop novocaine (on the skin side), and making sure that the needle is in the fracture (blood in the syringe and anesthetic - into the mouth), to produce a multiple washout (with furatsilin solution) of the contents from the slit into the oral cavity through the damaged mucous membrane (LM Vartanyan).
Before proceeding to immobilize the jaw fragments with the help of rigid intermaxillary fastening (extension) or by the method of the least traumatic (percutaneous) osteosynthesis with Kirshner's needle, it is recommended to infiltrate soft tissues in the area of the mandibular fracture with a broad-spectrum antibiotic solution. The application of a more significant injury (for example, exposure of the angle of the jaw and application of the bone seam) is undesirable, since it contributes to the intensification of the onset inflammatory process.
In the presence of developed traumatic osteomyelitis, it is possible to fix fracture after the sequestrectomy with a metal spike inserted through the fracture, but it is more effective to fix the fragments of the lower jaw by external extra-focus compressors, which, with fractures complicated by traumatic osteomyelitis (in the acute stage of the course), provide consolidation in usual terms (not exceeding the healing of fresh fractures) and contribute to the reduction of the inflammatory process due to the fact that the computer Assumption is carried out without prior intervention in the focus of defeat. Extrafocal fixation of fragments allows further surgical intervention (open abscess, phlegmon, remove sequesters, etc.) without disturbing immobilization.
Traumatic osteomyelitis almost always has a lingering course, does not disrupt the essentially general condition of the patient. Long-lasting swelling of soft tissues in the fracture zone is associated with stagnation, peri-rest reaction, infiltration of lymph nodes. The rejection of bone sequestration from the fracture of the fracture occurs slowly; their size is usually insignificant (several millimeters). Periodically, exacerbations of osteomyelitis, periostitis and lymphadenitis with the formation of perimandibular abscesses, phlegmon and adenophlegmon are possible. In these cases, it is necessary to dissect tissues for the evacuation of pus, drain the wound and prescribe antibiotics.
In the chronic stage of osteomyelitis, it is advisable to use the compression approach of jaw fragments, or to assign pentoxyl 0.2-0.3 g 3 times a day for 10-14 days (either after tooth-splitting or after percutaneous osteosynthesis), or injected (through Dufo needle) into crevice fracture 2-3 ml of powdered suspension of lyophilized fruit allogeneity. It is recommended to administer the suspension once, under local anesthesia, 2-3 days after reposition and fixation of the fragments, ie, when the wound heals on the gum prevent the outflow of the suspension into the oral cavity. Thanks to such tactics, the intermaxillary traction can be removed, both in single and double fractures, 6-7 days earlier than usual, reducing the total duration of disability by an average of 7-8 days. The extraoral injection into the fracture region of 5-10 ml of 10% alcohol in 0.5% of novocaine also accelerates the clinical consolidation of the fragments by 5-6 days and reduces the duration of disability by an average of 6 days. The use of allogeneity and pentoxyl allows a significant reduction in the number of inflammatory complications.
There are data on the effectiveness of application for the purpose of stimulating osteogenesis (in the zone of traumatic osteomyelitis) of various other methods and means: focal dosed vacuum, ultrasound, magnetic therapy according to NA Berezovskaya (1985), electrostimulation; low-intensity radiation from a helium-neon laser, taking into account the stage of the post-traumatic process; local oxygen therapy and three-, fourfold x-irradiation in doses of 0.3-0.4 fairy (with pronounced signs of acute inflammation, when it is necessary to remove swelling and infiltration or to accelerate abscessing, to stop the pain symptom complex and create favorable conditions for wound healing); thyrocalcitonin, ekteritsida in combination with ascorbic acid, nerobol in combination with protein hydrolyzate, fosfren, gemostimulin, preparations of fluorine, osteogenic cytotoxic serum, carbostimulin, retabolil, eleutterococcus; inclusion in the diet of the patient paste "Okean" from krill, etc. In the stage of chronic traumatic osteomyelitis after necrectomy, some authors use X-ray therapy at a dose of 0.5-0.7 grams (5-7 irradiations) in order to eliminate local signs of aggravation of the inflammatory process, accelerate the cleansing of the wound from necrotic mass, improve sleep, appetite and overall well-being of patients. Good results with traumatic osteomyelitis of the lower jaw are obtained in the case of a combination of sequestrectomy with radical treatment of the bone wound, filling the bone defect with breasts and rigid immobilization of the jaw fragments.
When a fracture is combined with periodontitis, the inflammatory phenomena in the soft tissues of the fracture region are particularly pronounced. In such patients arriving on the 3rd-4th day, pronounced phenomena of gingivitis, bleeding gums, fetid smell from the mouth, and discharge of pus from the pathological pockets are observed. Consolidation of the fracture with periodontitis is more prolonged. In such cases it is recommended, along with fracture treatment, to carry out complex treatment of periodontitis.
A great value in the treatment of fractures of the lower jaw is therapeutic exercise. After 1-2 days after immobilization with a single-jawed tire or an extraoral device, you can start active exercises for chewing (with minimal amplitude of movement), facial muscles and tongue. With intermaxillary traction, from the 2nd to the 3rd day after the fracture (shinning) and until the removal of the rubber pull, general toning exercises, exercises for facial muscles and tongue, exercises for volitional tension for the masticatory muscles can be used. After primary consolidation of the fracture and removal of the intermaxillary rubber tract, active exercises for the lower jaw are prescribed.
Disturbance of blood flow in the area of masticatory muscles leads to a decrease in the intensity of mineralization of the regenerate in the gap of the angular fracture (VI Vlasova, IA Lukyanchikov), which is also the cause of frequent complications of an inflammatory nature. Timely prescribed mode of motor activity (exercise therapy) significantly improves electromyographic, gnathotomimetric and dynamometric indicators of the function of the masticatory muscles. Early functional load on the alveolar processes with the help of denture-gum prostheses used for fractures within the dentition (if there is one toothless fragment that can be manually adjusted and held by the base of the prosthesis, and also in cases of rigidly stable immobilization by osteosynthesis ), also contributes to the reduction of the period of incapacity for work for an average of 4-5 days. When included in the complex of therapeutic measures of functional chewing loads, regenerate is more quickly restructured, restores its histological structure and function, while retaining its anatomical shape.
To reduce the degree of hypodynamic disorders in the masticatory muscles and in the region of the fracture of the mandible, it is possible to apply the method of bioelectrical stimulation (common in general traumatology, sports and space medicine) of temporal parietal and proper chewing muscles with the help of the Mioton-2 apparatus. The procedures are carried out daily for 5-7 minutes for 15-20 days, starting from the 1-3 day after immobilization. Electrostimulation leads to a reduction of these muscles without the occurrence of movements in the temporomandibular joints; due to this in the maxillofacial area, blood circulation and neuroreflex connections are restored more quickly, muscle tone is preserved. All this also contributes to reducing the period of consolidation of the fracture.
According to VI Chirkin (1991), the inclusion in the usual complex of rehabilitation measures of multichannel bio-controlled proportional electrostimulation of temporal, chewing muscles and muscles lowering the lower jaw, in the subthreshold and therapeutic regimen in patients with unilateral trauma, allowed by the 28th day in full restore blood filling of tissues, increase the volume of opening the mouth to 84%, and the amplitude of the M-response to 74% in comparison with the norm. It was possible to normalize the chewing function, and patients for chewing food samples spent so much time and used as many chewing movements as healthy individuals.
In patients with bilateral surgical trauma of the masticatory muscles, the procedures of multichannel biocontrolled proportional electrical stimulation in subthreshold, therapeutic and training regimens can begin from early periods (7-9 days after surgery), which provides positive shifts in the blood filling of the trauma zone, as evidenced by rheographic studies, which by the time of tire removal reached the norm.
It was possible to achieve an increase in the volume of opening the mouth to 74%, the amplitude of the M-response also increased to 68%. Almost normalized, served functional electromyography, the function of chewing, the indices of which have reached the level of average indicators of healthy individuals. The author believes that the method of multichannel reova- zoophagy, stimulation electromyography of the masticatory muscles, the recording of periodonto-muscular reflex and the method of multichannel functional electromyography with standard food tests are most objective in the study of the masticatory system and can be the choice methods for examining patients with both jaw fractures and with a surgical (operating) injury to the masticatory muscles.
The procedures of multichannel biocontrolled proportional electrostimulation of the masticatory muscles in three modes according to the method recommended by the author allow to start functional rehabilitation treatment from early terms. This type of treatment is most suitable for the natural function of the chewing system, it is well dosed and controlled, which provides for today the highest results of restoration of function and allows to reduce the total time of disability for 5-10 days.
The problem of treatment and rehabilitation of patients with fractures of the lower jaw accompanied by injuries of the lower lunar nerve deserves special consideration. According to SN Fedotov (1993), lesions of the lower alveolar nerve were diagnosed in 82.2% of the patients with a fracture of the mandible, of which 28.3% were mild, 22% moderate and 31.2% severe. To an easy category of damage are those in which the reaction of all teeth on the side of the fracture was in the range of 40-50 μA, and in the area of the skin of the chin and mucous membrane of the oral cavity, slight hypesis was observed; to the middle category - the reaction of teeth to 100 μA. If the reaction is more than 100 μA and partial or complete loss of soft tissue sensitivity - the damage is considered to be severe. At the same time, neurological disorders with fractures of facial bones and their treatment in practical medicine are given insufficient attention. The depth of nerve damage, according to SN Fedorov, even more increases with surgical methods of connecting fragments. As a result of this, long-term sensitive disorders develop, neurotrophic destructive processes in the bone tissue, slowing of the fusion of fragments, decreased function of chewing and painful pain.
Based on his clinical observations (336 patients), the author developed a rational complex of restorative treatment of fractures of the lower jaw, accompanied by injuries of the third branch of the trigeminal nerve, using physical methods and medicinal stimulating drugs (neurotropic and vasodilating). To prevent secondary lesions of the lower alveolar nerve and its branches during the surgical treatment of fractures, a new version of osteosynthesis of fragments with metal spokes is proposed, based on a sparing relation to the teeth, as well as to branchings of the lower alveolar nerve.
One patient with neurological disorders already on the 2nd-2nd day after the immobilization of the fragments, the author assigned exposure to the UHF electric field or the solux lamp; in the presence of pain along the course of the lower alveolar nerve, an electrophoresis of 0.5% solution of novocaine with epinephrine according to AP Parfenov (1973) was used. Another patient, according to the indications, was assigned only ultrasound. After 12 days, in the stage of primary corneal formation, electrophoresis with 5% calcium chloride solution was administered.
Simultaneously with physical treatment from 2 to 3 days, medicinal stimulant preparations were also used: vitamins B 6 V 12; dibasol by 0.005; at deep disorders - 1 ml of 0.05% solution of prosirin according to the scheme. At the same time, drugs stimulating blood circulation were prescribed (papaverine hydrochloride 2 ml of a 2% solution, nicotinic acid 1% 1 ml, compliance 2 ml of 15% solution, for a course of 25-30 injections).
After a 7-10 day break, if nerve damage persisted, electrophoresis with 10% potassium iodide solution or electrophoresis with enzymes was prescribed, for a course of 10-12 procedures; Galantamine 1% 1 ml was used for the course of 10-20 injections, paraffin and ozocerite applications. After 3-6 months with the preservation of neurological disorders, treatment courses were repeated until complete cure. An obligatory component of the treatment recommended by SN Fedotov is the constant monitoring of its effectiveness according to the data of neurological research methods. The use of the described complex of restorative treatment promoted a more rapid recovery of the conduction of the lower alveolar nerve: for mild functional disorders, for 1.5-3 months, medium and heavy, for 6 months. In the group of patients who were treated with traditional methods, the conductivity of the lower alveolar nerve with minor disorders was restored within 1.5-3-6 months, with moderate and severe disorders in 6-12 months. According to SN Fedorov, about 20% of patients over a year remained persistent and profound disorders of pain sensitivity. Damage to the lower alveolar nerve of medium severity and heavy, in all probability, is accompanied by a hyperextension of the nerve trunk at the moment of displacement of fragments, bruises with a break of nerve fibers, partial or complete breaks. All this slows down reinnervation. An earlier restoration of the trophic function of the nervous system had a beneficial effect on the quality and timing of the consolidation of the fragments. In the first (main) group of patients, consolidation of fragments occurred on average in 27 + 0.58 days, the incapacity for work was 25 ± 4.11 days. The chewing function and muscle contractility reached normal values by 1.5-3 months. In the second (control) group, these indicators were 37.7 + 0.97 and 34 + 5.6 days, respectively, and the chewing function and contractile ability of the muscles were restored later - by 3-6 months. These measures for the healing of patients with trauma should be carried out in the rehabilitation rooms.
In addition to traumatic osteomyelitis, abscesses and phlegmon in the jaw fracture against the background of slow inflammation of the bone, submandibular lymphadenitis, which does not respond to the usual methods of treatment, may appear . Only with a detailed complex examination of such patients with the use of radiography, indirect radionuclide scan-lymphography using a colloidal solution of 198 AU, immunodiagnostic samples, it is possible to confidently diagnose the secondary (posttraumatic) actinomycosis of the submandibular lymph nodes.
It is possible that the fractures of the mandible can be complicated by actinomycosis and tuberculosis simultaneously (more often in patients with tuberculosis). Possible and more rare, but no less severe complications of injuries of the maxillofacial area: angina Zhansulya-Ludwig; later bleeding after osteosynthesis, complicated by inflammation; asphyxia after intermaxillary traction, sometimes leading to death of the patient due to blood aspiration with bleeding from the lingual or from the carotid artery; false aneurysm of the facial artery; thrombosis of the internal carotid artery; secondary paralysis of the facial nerve (with a fracture of the lower jaw); emphysema of the face (with a fracture of the upper jaw); pneumothorax and mediastinitis (with a fracture of the malar bone and upper jaw), etc.
The length of stay of patients on inpatient treatment depends on the localization of the trauma of the maxillofacial area, the course of the period of consolidation, the presence of complications.
The specified terms are not optimal, in the future, as the economic crisis and the expansion of the bed fund are overcome, it will be possible to prolong the stay of patients in the hospital until the end of treatment for trauma of the face of different localization. Patients with injuries of the maxillofacial area from the countryside should stay in the hospital for a longer period, as they, as a rule, can not come to the city for outpatient observation and treatment because of the distance range. The availability of well-established trauma care, rehabilitation rooms for patients with similar traumas in the city's dental facilities allows for a shortening of the length of their stay in the hospital.
Ambulatory treatment (rehabilitation) of victims with injuries of maxillofacial area
The organization of an outpatient stage of treatment of victims with injuries to the maxillofacial area is not always sufficiently clear, since patients are in many cases under the supervision of doctors of various institutions who do not have sufficient training in traumatology of the maxillofacial area.
In this regard, you can recommend using the experience of the rehabilitation room at the maxillofacial clinic of Zaporizhzhya GIDUV and the regional dental clinic, which implemented in its practice exchange cards containing all information about the treatment of the injured in the hospital, in the polyclinic at the place of residence and in the rehabilitation room.
When rehabilitating patients with injuries of the maxillofacial area, it should be borne in mind that such traumas are often combined with closed craniocerebral trauma, and also are accompanied by a violation of the function and structure of the temporomandibular joints (TMJ). The degree of severity of these disorders depends on the localization of the fracture: in fractures of the condylar process, degenerative changes in both joints are observed more often than with extraarticular fractures. Initially, these disorders have the character of functional insufficiency, which in 2-7 years can develop into degenerative changes. Unilateral arthrosis develops on the side of damage after single fractures, and bilateral - after double and multiple. In addition, in all patients with fractures of the lower jaw, judging by electromyography, pronounced changes in the masticatory muscles are noted. Therefore, to ensure continuity in the trauma patients in dental clinics, they should be taken by a trauma dentist who provides comprehensive treatment of patients with injuries to the face of any localization.
Particular attention should be paid to the prevention of complications of inflammatory and psycho-neurological disorders - cephalgia, meningoencephalitis, arachnoiditis, autonomic disorders, hearing and hearing impairment, etc. To this end, it is necessary to use physiotherapeutic methods of treatment and physiotherapy more widely. It is necessary to carefully monitor the condition of the fixative bandages in the oral cavity, the condition of the teeth and mucous membrane, and also to perform timely and rational dentistry. When determining the timing of immobilization, the duration of temporary incapacity for work and treatment, it is necessary to individually approach each patient, taking into account the nature of the injury, the course of the disease, the age and the profession of the patient.
In the rehabilitation dental office, the patient must complete the treatment. Therefore, by a special order on the appropriate health care, the doctor of this office is given the right to issue and prolong the sheets of temporary incapacity for work regardless of the place of work and residence of the patient. It is desirable to organize one dental rehabilitation cabinet for 200-300 thousand people. In the case of a reduction in the frequency of injury, the tasks of the cabinet can be expanded by providing surgical patients with other profiles prescribed from the inpatient for outpatient treatment.
In rural areas, the treatment of victims with injuries to the maxillofacial area should be carried out in district clinics (hospitals) under the supervision of the district dental surgeon.
The system of treatment of patients with a trauma of the person should include a systematic examination of the long-term results of treatment.
Stationary dental offices of regional hospitals and regional (regional) dental clinics should implement an organizational and methodical guide for the provision of dental care in the region, including patients with trauma to the face.
The centers of specialized dental care are often clinical bases of the maxillofacial surgery faculties of medical schools and institutes (academies, faculties) of the improvement of doctors. The presence of highly qualified personnel makes it possible to widely apply here the newest methods of diagnosis and treatment of various injuries of the maxillofacial area and, moreover, allows considerable savings.
Before the main dentist and oral and maxillofacial surgeon of the region, the city, the head of the maxillofacial department are the following tasks to improve the state of care for victims with a trauma to the face:
- Prevention of injuries, including the elucidation and analysis of the causes of occupational injuries, especially in agricultural production; participation in the implementation of general preventive measures to prevent industrial, transport, street, sports trauma; prevention of injuries of children; carrying out of wide explanatory work among the population, especially young working age, with the purpose of preventive maintenance of household traumatism.
- Development of the necessary recommendations for the provision of first and first medical assistance to patients with trauma at health centers, paramedic stations, trauma centers, ambulance stations; acquaintance of the average medical personnel and physicians of other specialties with the elements of the first and first medical assistance in cases of trauma to the face.
- Organization and conduct of permanent cycles of specialization and improvement of dentists, surgeons, traumatologists, general practitioners on the issues of rendering assistance to patients with personal injuries.
- Application and further development of the most advanced methods of treatment of jaw fractures; prevention of complications, especially inflammatory; more widespread use of complex methods of treatment of traumatic injuries of a person.
- Preparation of nursing staff who have basic skills in providing first aid to patients with injuries to the face and jaws.
When analyzing the qualitative indicators of the work of dental institutions, one should also take into account the state of care for patients with personal injuries. Particular attention should be given to the analysis of errors made in the provision of assistance. It is necessary to distinguish between diagnostic, therapeutic and organizational errors, for which it is recommended to maintain a special journal (for each city and district).
The choice of the method of repositioning and fixing jaw fragments with chronic fractures
Depending on the prescription of the fracture of the upper or lower jaw and the degree of stiffness of the fragments, orthopedic or surgical methods are used. Thus, with fractures of the alveolar process of the upper jaw with a hard-to-remove displacement of the fragments, steel-wire tires designed for skeletal traction are used. The elasticity of the steel wire contributes to the rectification of the debris along the horizontal and vertical lines. In particular, if a fragment of the anterior part of the alveolar process is displaced posteriorly, a smooth bus-brace is applied, fixing it in the usual way to the teeth on either side of the fracture line; teeth fragments are attached to the wire by so-called "pendant" ligatures with a low voltage. Gradually (simultaneously or within a few days - depending on the age of the fracture), pulling the ligature wire by twisting, slowly patch up the fragment of the alveolar process. For the same purpose, it is possible to use thin rubber rings covering the neck of the tooth and fixing anteriorly on the wire, which in this embodiment need not be steel.
If the lateral portion of the alveolar process of the upper jaw is displaced internally, the steel wire tire is bent in the shape of a normal dental arch. Gradually, the fragment returns to the correct position with respect to the lower dental arch. In the case of mixing the lateral segment of the alveolar process outwardly, it is inwardly guided by means of an elastic traction installed across the hard palate.
With the stiffness of the downwardly displaced fragment of the alveolar process of the upper jaw for traction, one can use rubber rings or a Shelhorn bandage applied through the surface of the closing of the teeth.
With the stiffness of the fragments of the lower jaw, intermaxillary traction is used with the help of toothbrushes. If there are no teeth on the stiff jaw fragments, you can use apparatuses for repositioning and fixing fragments, or reposition and fix fragments through extraoral or intraoral access.
Examination of temporary incapacity for work with jaw fractures
Every citizen has the right to material security in old age, in case of illness, full or partial loss of ability to work, and also loss of the bread-winner.
This right is guaranteed by social insurance of workers, employees and peasants, temporary disability allowances and many other forms of social security.
Loss of ability to work after a trauma is ascertained in case of impossibility to carry out socially useful work without damage to health and efficiency of production.
With jaw fractures, temporary and permanent loss of ability to work is possible, the latter is divided into full and partial.
If the dysfunctions of the jaws that impede professional work are reversible and disappear in treatment, disability is temporary. With full temporary disability, the victim can not perform any work and needs treatment in accordance with the regime prescribed by the doctor. For example, patients with jaw fractures in the acute period of trauma with severe pain syndrome and impaired function are completely temporarily incapacitated.
Partial temporary incapacity for work is ascertained in cases when the victim is not able to work in his specialty, but can perform other work without damage to his health, at which rest or allowable load on the damaged organ is ensured. For example, a sinker in a mine that received a fracture of the lower jaw, with a delayed consolidation of fragments, is usually unable to work for 1.5-2 months in its specialty. However, after the elimination of acute events 1.5 months after the injury, the worker can be transferred to an easier job (for a period not exceeding 2 months) by the decision of the VKK: the lift driver, the lamp charger, etc. When transferring to another job due to the consequences of jaw fracture leaves of incapacity for work are not issued.
Expert examination of the victim should begin with the establishment of a correct diagnosis, which helps determine the labor forecast. Sometimes the doctor, having made the correct diagnosis, does not take into account the labor forecast. As a result, the victim is either prematurely discharged to work, or when he is restored to work, he is unfairly prolonged with a sheet of incapacity for work. The first leads to all sorts of complications that are detrimental to health and delay treatment; the second - to unreasonable expenditure of means on payment of sheets of invalidity.
Therefore, the main differential criterion for temporary disability is the favorable clinical and labor prognosis, characterized by a complete or significant restoration of dysfunction of the jaws as a result of trauma and disability in a relatively short time. Restoration of ability to work in jaw fractures is characterized by the degree of restoration of the function of the damaged jaw, namely: good consolidation of fragments in the correct position, maintaining a normal bite of the teeth, sufficient mobility in the temporomandibular joints, absence of severe disorders of blood and lymph circulation, pain and any other disorders , associated with damage to the peripheral nerves in the maxillofacial region.
Temporary disability for jaw fractures can be caused by labor injury and domestic trauma. Determining the cause of temporary disability in fracture of the jaws is one of the important tasks of the dentist, as it involves addressing issues that require not only medical but also legal competence.
The disease is considered to be associated with a "labor injury" in the following cases: when performing work duties (including on a business trip during office hours), in the performance of an action in the interests of the enterprise, the firm, although without commission from their administration; in the performance of public or state duties, as well as in connection with the fulfillment of special tasks of state, trade union or other public organizations, even if these tasks were not connected with this enterprise or institution; on the territory of the enterprise or institution or in another place of work during working hours, including established breaks, as well as during the time necessary for putting in order the tools of production, clothing, etc. Before and after the end of work; near the enterprise or institution during working hours, including established breaks, if the presence there did not contradict the rules of the established schedule; on the way to work or from work home; when fulfilling the duty of a citizen to protect law and order, saving human life and protecting state property.
To determine the cause of temporary incapacity for work requires an act on the accident, which is timely and in form compiled by the administration of the enterprise where the accident occurred. In the act there should be an indication that an accident occurred during work, a description of his character, etc. In case of group accidents, acts must be compiled for each victim.
An act can not be drawn up if an accident occurred on the way to work or from work. In these cases, it is necessary to have a certificate of the transport administration, a protocol compiled by the police, a certificate of the enterprise or the institution in which the victim works, indicating the time of commencement and completion of his work for this number, as well as certificates of residence.
The greatest difficulties arise in determining the nature of disability (temporary or persistent), as well as in determining the term for the termination of temporary disability, which for each patient is individual.
It should be borne in mind that in some cases the period of temporary disability does not correspond to the period for which the patient is issued a disability sheet (for example, with a domestic trauma, etc.). Therefore, in order to characterize the average period of incapacity, it is necessary to accurately indicate the period between the moment of injury and the moment of return of the victim to labor.
Patients with fractures of the jaws after the end of the inpatient period of treatment continue to be treated in outpatient settings, and before disability is established, the disability is documented by a sheet of incapacity for work. However, the period of stay on the disability sheet of patients recognized as disabled in the future can not be identified with the indicator of the average duration of temporary disability. This period, preceding the transfer of a patient to a disability, is properly called a pre-invalid period.
When deciding on the timing of temporary disability, it is necessary to take into account not only the nature of the trauma, but also the patient's profession, the conditions of his labor and life, the type of injury (labor or personal injury, etc.). So, the fastest working capacity is restored with relatively light sports injuries; In the case of industrial and transport injuries, the period of temporary incapacity for work is longer.
To exclude the possible aggravation, it is necessary to widely apply such objective research methods as palpation, masticiography, roentgenography, osteometry.
The period of incapacity for jaw fractures depends on the characteristics of the profession of the victim: for workers of mental labor, temporary loss of working capacity is less long than for persons engaged in manual labor; they can be discharged to work 20-25 days after the trauma, continuing treatment outpatiently. At the same time, patients whose profession is associated with constant tension and movement of the muscles of the maxillofacial area (artists, lecturers, musicians, teachers, etc.) are allowed to return to work only with the full restoration of the function of the jaws.
Especially long is the period of temporary incapacity for work in patients engaged in heavy physical labor. This list of patients with a disability sheet is extended after removing the fixing tires and devices for another 2-3 days to fully adapt the chewing process. If they are prematurely discharged to work, complications may develop (osteomyelitis, jaw refracture, etc.). In addition, such patients are often unable to complete the full scope of the basic work processes. For example, workers of the coal industry have a longer period of temporary disability than workers in other professions, which is due to the specific nature of work in underground conditions and the nature of injuries, which are often accompanied by damage to the soft tissues of the face.
In persons over 50 years of age, the period of temporary incapacity for work is increased due to a slowdown in consolidation.
Consolidation of the fracture of the lower jaw in patients with periodontitis lasts 1.5-2 months longer. In patients without periodontitis, it occurs an average of 3-4 months after injury. Factors of environmental disadvantage should also be taken into account in determining both the duration of the fixation and the period of temporary incapacity for work.
The use of compression extra-focal treatments for jaw fractures, combined with a general effect on the body and treatment of periodontitis, as well as timely and rational local orthopedic and surgical measures aimed at repositioning and fixing jaw fragments, help reduce the time of temporary disability.
If in the acute period of the trauma the issues of examination of work capacity are solved relatively easily, then in the future when the patient develops certain complications (delayed consolidation of fragments, contracture, ankylosis, etc.), difficulties arise in determining the term and type of disability of the victim. Based on the nature of the fracture, its clinical course and the complications that have occurred, the dental surgeon must determine, at least roughly, the duration of temporary disability for the injured and draw up the correct labor prediction, which is the criterion for establishing temporary or permanent disability.
The labor forecast can be favorable, unfavorable and questionable. With a favorable labor forecast, it is possible to restore work ability and return the victim to the former or equivalent work. The labor forecast is unfavorable when, as a result of a trauma or its complications, the victim can not work in his specialty and there is a need to transfer him to another job that corresponds to the state of health, or when the victim is unable to perform any work. Doubtful labor forecast means that at the time of examination there are no data necessary to address the issue of the outcome of jaw fracture and the possibility of rehabilitation. Difficulty is the prognosis for the slow consolidation of jaw fractures complicated by traumatic osteomyelitis. In some cases, when surgical, physiotherapeutic and other methods of treatment are applied, the fracture is in the right position and the work capacity is restored, in others, despite the treatment, bone defects are formed that lead to persistent disability
It should be noted that the labor forecast is closely related to the clinical one, depends on it, but does not always coincide with it. Thus, even in the case of an unfavorable clinical outcome of jaw fractures (irregular fusion without malocclusion, or with toothless jaws), the labor prognosis may be favorable, since it is determined not only by anatomical changes, but mainly by the degree of restoration of function, the development of compensatory adaptations, the profession affected, as well as other factors.
Examination of temporary loss of ability to work with fractures of the lower jaw
The average duration of temporary incapacity for fractures of the mandible is 43.4 days. The terms of rehabilitation depend on the localization of fractures. In cases of fractures in the condylar process and the jaw branch, with a good comparison of bone fragments, the duration of the temporary disability is minimal (36.6 days). Fractures of this localization are usually closed uninfected.
The main factors contributing to rapid consolidation are good blood supply to the bone in the fracture region and the presence of a muscle case, which allows you to remove the intermaxillary rubber cravings for 12-14 days. Early functional treatment helps to accelerate the consolidation of jaw fragments.
The treatment of victims with fracture-dislocations of the condylar processes of the lower jaw is of great difficulty , as a result of which the period of temporary disability of persons engaged in manual labor is on the average 60 days.
To assess the degree of consolidation of jaw fracture, it is useful to use the EOM-01-ц echoosteometer with an oscillation frequency of 120 ± 36 kHz. The indicator of echoosteometry when using, for example, an extra-focus device VA Petrenko et al. (1987) for the treatment of fractures of the condylar process is almost normalized only on the 90th day. Therefore, it is obvious that the mentioned 60-day period, previously established in the "Methodological Recommendations", is subject to either scientific justification or a change, especially in zones of radioisotope, industrial and chemical pollution of soil, water, food.
In cases of fractures of the lower jaw in the presence of a tooth in the fracture, the period of temporary disability is much longer than in fractures outside the dentition.
With central fractures of the lower jaw, the recovery period is almost the same as for the localization of fractures in its lateral divisions (44.2 days).
The recovery period of work capacity for single fractures of the mandible is on average 41.2 days, in patients with double fractures - 44.8 days. Multiple fractures of the lower jaw are the most severe, since with them, there is almost always a significant displacement of fragments that can protrude into the oral cavity. Such fractures are open and susceptible to infection. The average period of temporary incapacity for work is 59.6 days.
With comminuted fractures of the lower jaw, the recovery period is slightly longer than for linear, and is 45.5 days on average.
In patients with fractures of the lower jaw, combined with a concussion of the brain, the average period of incapacity for work is increased to 47.4 days. The issue of the possibility of discharging such patients from a hospital should be solved together with a neurologist.
The terms of disability also depend on what methods are used to treat fractures of the lower jaw. The period of restoration of ability to work in patients with fractures of the mandible, treated with non-surgical methods, averaged 43.7 days, surgical - 41.3 days. The minimum period for the loss of temporary work capacity is observed in the treatment of fractures of the lower jaw without displacement of fragments with kappas from self-hardening plastics (26.3 days) and sling-visible bandage by I.I. Urbanskaya (36.7 days). Disabled victims who for the treatment of mandibular fractures were applied Tooth The Multi- aluminum tires, rebuilt later (44.6 days).
The main reasons for the increase in the period of rehabilitation are long-term intermaxillary fixation without the use of early functional treatment, relative mobility of fragments, traumas of the interdental papillae by gum wires, loosening of the teeth,
[18],
Examination of temporary loss of ability to work with fractures of the upper jaw
The average length of the period of temporary disability for fractures of the upper jaw is 64.9 days.
The average length of the period of incapacity for work depends on the nature of the injury of the upper jaw: in the case of non-industrial trauma it is 62.5 days, and in the case of industrial injury - 68.3 days.
The duration of disability in trauma is to a certain extent determined by the severity of the injury. Restoration of ability to work with a fracture of the alveolar process of the upper jaw occurs on average for 43.6 days, and with a fracture of the body of the upper jaw, the average period of incapacity for work is 69.9 days; according to the type of Le Fort I - 56.0 days, type Le Fort II - 65.4 and type Le For III - 74.7 days.
In uncomplicated fractures of the upper jaw, the period of incapacity for work is 60.1 days on average and 120-130 days for complicated ones.
One of the features of fractures of the upper jaw is their combined character, due to the anatomical proximity of the facial and brain areas of the skull. Traumatic injuries to the bones of the skull and brain are not always diagnosed by dentists, which adversely affects the treatment of patients.
Terms of temporary incapacity for work in isolated and combined fractures of the upper jaw are different. Thus, with a fracture of the upper jaw, combined with a concussion of the brain, they are 70.8 days, with a combination with a fracture of the mandible, the average period of incapacity for work is 73.3 days, with a fracture of the base of the skull 81.0 days, with a fracture of the cranial vault - 126.7, 120.5, with a fracture of other bones - 89.5 days.
Multiple fractures of the bones of the face, skull and trunk give temporary disability within 87.5 days.
The timing of temporary disability also depends on the treatment of upper jaw fractures. When used in patients with fractures of the maxilla of orthopedic methods of treatment, the average period of temporary incapacity for work is 59.2 days (55.4 for uncomplicated and 116.0 for complicated fractures), and surgical methods for 76.0 days (69.3 for uncomplicated and I53.5 for complicated fractures ).
A longer period of temporary disability in surgical treatment of fractures is due to the fact that they are used in the most severe injuries, when orthopedic methods are not shown or are ineffective.
[19]
Temporary disability registration
A dentist has the right to issue to the patient with a jaw fracture a certificate of incapacity for a period not exceeding six days. The Medical Control Commissions (CWC) are given the right to prolong the disability sheet for a longer period (for patients with a lump-sum injury for up to 10 days), but in general not more than 4 months from the date of the injury. In this case, persons who authorize the extension of the disability sheet are required to examine the patient personally. With a long course of the disease, such examinations should be carried out at least once in 10 days, and if necessary - much more often, especially in the first time after injury.
In the case of disability due to occupational injuries, the physician issues a disability certificate, which is a document confirming temporary incapacity for work and entitling the victims to receive social security benefits.
In case of loss of ability to work due to domestic trauma, the medical institution issues a certificate of incapacity for work for five days, and starting from the sixth - a certificate of incapacity for work. In the case when the victim addresses a doctor on the day that he has already worked in the workplace, the doctor, if necessary, issues a disability sheet, dating him on the day of treatment, but relieves the injured from work only from the next day.
Patients with fractures of the jaws treated in the hospital, the sick leave is issued at discharge, but in cases of prolonged stay in it, the disability sheet can be issued before discharge to receive wages.
If, as a result of in-patient treatment, the patient's work capacity is restored, the disability sheet is closed. In the case when the patient, while discharging from the hospital due to the consequences of the fracture, continues to be incapacitated, a sheet of incapacity for work in the hospital is not closed, but on it an appropriate note is made about the need for outpatient treatment. In the future, the list of incapacity for work is extended by the dentist of the treatment and prophylactic institution, in which the patient continues treatment. It should be noted that persons who are injured as a result of intoxication or acting as a result of intoxication and who need outpatient and inpatient care are not issued incapacity to work.
The issue of a discharge for work or direction of a patient with a simple or complicated fracture of the maxilla to the WTEC is decided depending on the clinical and labor prognosis. In those cases when, despite all medical measures, the clinical and labor prognosis remains unfavorable and the disability is stable, patients should be referred to the WTEC to determine the disability group, for example, in case of a fracture of the lower jaw complicated by osteomyelitis with subsequent formation a large defect in bone tissue and when there is a need for restorative bone-plastic surgery. In such cases, the timely establishment of the disability group and the release of the patient from work allow the whole complex of medical measures to restore the health of the victim, after which he can perform work on his or any other specialty. The list of incapacity for work is closed on the day of issuing the conclusion of the WTEC on the establishment of a disability regardless of its causes and group.
Rational employment of disabled people is of great importance, since feasible work contributes to a more rapid recovery or compensation for impaired functions, improves the overall condition of disabled people and increases their material security.
Sometimes accompanying diseases, which in themselves do not cause significant disability, aggravate the patient's condition and, in combination with the underlying disease, cause more pronounced impairment of functions. Therefore, in carrying out the examination of work capacity in such cases, extreme caution and a critical approach are needed in order to correctly assess the relative importance of these changes in the reduction or loss of ability to work.