
Atypical mononuclear cells
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Virocytes are lymphocytes with morphological features of monocytes. Consider the features of atypical mononuclear cells, the causes of their appearance, diagnostic methods and analyzes for mononuclear cells.
Mononuclear cell structures contain one nucleus and are considered to be young cells entering into the fight against viruses. Their presence indicates an infectious or viral lesion of the body. In some cases, even a simple viral infection causes an increase in virotsitov in the blood. If the level of atypical mononuclear cells exceeds the threshold of 10% in the leukocyte formula, then this indicates an infectious mononucleosis.
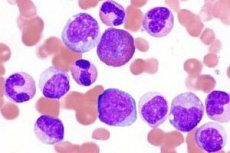
By the size, color of the cytoplasm and the shape of the nucleus, atypical cells resemble lymphocytes and monocytes of peripheral blood. There are two types of virotsitov: lymphocyte-like and monocytic-like, which differ in their size and composition of the cytoplasm. Mononuclear cells have a polymorphism of the core shape with a spongy structure, the color of the cells from blue to pronounced-basophilic. Many scientists consider them to be low-grade T-lymphocytes.
Atypical mononuclear cells in children
Virocytes can occur in the blood of patients of any age. Atypical mononuclear cells in children indicate a viral disease - mononucleosis. The disease occurs due to the Epstein-Barr virus, which affects the parenchymal organs and cells of the lymphoid tissue. Infectious process is localized in the pharynx, liver and spleen. Atypical cells appear with chickenpox, since the virus belongs to the same genus as the causative agent of mononucleosis. Its effect reduces the protective properties of the immune system, opening the way for other pathologies.
Most often, atypical mononuclear cells are found in children 8-10 years old. This is due to the fact that this age category is susceptible to many infectious diseases. The least affected are children under 1 year of age, at this age they find about 0.5% of all cases of mononuclear cells. Infection is transmitted by airborne droplets, by contact between children, but it is unstable to the environment.
Symptoms of atypical mononuclei in children:
- Increased body temperature.
- Enlargement of lymph nodes.
- Increased spleen / liver.
- Changes in total blood composition.
- Plaque on the tonsils.
- Increased sweating.
In rare cases on the body of the child appear rashes of a petichial nature (without a certain localization) and icteric staining of the skin. According to medical statistics, most often the virus is found in boys, the peak incidence falls on the autumn-winter and spring period. Malicious microorganisms get on the mucous membrane of the upper respiratory tract and spread throughout the body, affecting the lymph nodes, liver and spleen. The incubation period takes 5 to 15 days.
To restore the normal level of virotsitov in the blood, symptomatic and restorative therapy is carried out, which are aimed at eliminating the signs of infection. Antibiotics are not used, since they do not affect the virus. Therapeutic properties are vitamins of group B, C, P.
 [8], [9], [10], [11], [12], [13], [14], [15]
[8], [9], [10], [11], [12], [13], [14], [15]
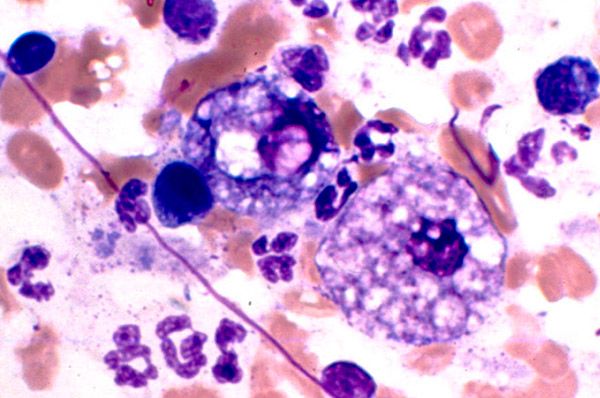
Morphology of atypical mononuclear cells
The structure of viral cells largely determines the mechanism of their action and damage to the body. The morphology of atypical mononuclear cells indicates that their pathogen is the Epstein-Barr virus. These cells belong to herpes viruses, have a complex structure and contain DNA in the form of a double helix. The virus is resistant to low temperatures and drying.
Infection is transmitted by airborne, contact and gemokontaktnym ways. The disease occurs in the form of sporadic outbreaks. As a rule, infection is diagnosed in preschool and school age children, mainly in boys. Children under one year do not get sick because of passive immunity. The disease is a seasonal phenomenon, the aggravation is observed in the winter-spring period. The disease does not recur, mortality is low, but there are data on single cases of rupture of the spleen, CNS lesion and stenosis of the larynx.
Penetration of the virus is through the mucous membrane of the upper respiratory tract and oropharynx. Adhesion occurs by the use of receptors, which are located on the surface of the cells of the epithelium. Propagation of the virus leads to the destruction of cells, which causes the release of new generations of infection into the bloodstream. Atypical mononuclears are infected with B-lymphocytes with altered functional and morphological properties. Pathological changes in the immune system lead to the fact that the body is not able to completely neutralize the virus, which can be latent in life for B-lymphocytes for life.
Cells morphologically similar to atypical mononuclear cells
Since virotsity indicate the presence of infection in the body, there are other cellular structures with them similar. Lymphocytes are cells morphologically similar to atypical mononuclears. They are similar in shape and size to the nucleus, the cytoplasm. They are found in the blood for various viral diseases (rubella, influenza, measles, chicken pox), autoimmune diseases, allergic reactions, vaccination and various tumors.
Proceeding from this, two types of atypical mononuclear cells are distinguished: monocyte-like and lymphocyte-like. Lymphocyte-like differs from lymphocytes in that they have a foam cytoplasm, they are characterized by polymorphism of the nucleus from a spongy structure. That is, the virocytes are mutated T-lymphocytes. In rare cases, cells with granular a-naphthyl acetate zestase, not inhibited by NaF, are detected. Virocytes have a high activity of acidic phosphatase, lactate, a-glycerophosphate and dehydrogenase succinate.
Blood test for atypical mononuclear cells
Diagnosis of viral and infectious diseases involves conducting various studies. The blood test for atypical mononuclears is performed with clinical symptoms of mononucleosis and similar diseases. Virocytes are determined by a general blood test, which evaluates the qualitative and quantitative cellular composition, the leukocyte formula, the ratio of plasma and cell volume, color indices and ESR.
Modified T-lymphocytes are detected with the help of a lymphocytic formula (percentage ratio of different types of leukocytes). It is used to diagnose infectious, inflammatory and hematological ailments, as well as to evaluate the effectiveness of treatment. Mononucleosis is confirmed in the case when more than 10% of atypical cellular structures are present in the blood.
Atypical mononuclears in mononucleosis
The presence of virorocytes in the blood indicates an infectious disease caused by the Epstein-Barr virus. Atypical mononuclear cells with mononucleosis, as a rule, exceed the threshold of 10%. The incubation period is not exactly established, it varies from 5 to 21 days, and in some cases up to 1-2 months. The disease begins with a sharp rise in temperature, inflammation of the cervical lymph nodes, difficulty in nasal breathing. Later, patients can palpate an enlarged spleen and liver.
If mononucleosis has an atypical form, then the clinical symptomatology is smeared, so the disease can be recognized only by laboratory tests. Prolonged and chronic forms are characterized by hematologic changes and lymphadenopathy, which can persist for 4-6 months. The criterion of severity is the severity of the intoxication syndrome, the duration of the disease and the presence of complications.
Atypical mononuclear cells in the blood require specific treatment. For therapy, glucocorticosteroids and vitamin complexes are used. Antibiotics are not used, because they do not affect the virus. If the liver is involved in the pathological process, the patient is assigned a dietary table №5а / №5. In the absence of proper treatment, the disease has a poor prognosis and threatens complications. Most often, these are neurological disorders that occur aseptic meningitis, encephalitis, and other pathologies.
The norm of atypical mononuclear cells in the blood
To detect the first signs of any diseases, a blood test is used. The norm of atypical mononuclear cells in the blood can diagnose various infectious and viral diseases. Normally, a healthy person should not have them. If their number exceeds 10% barrier, then this indicates an infectious mononucleosis. Cells can be present in lymphocyte blood and in healthy people, they normally contain no more than one-sixth of the total number of lymphocytes. The number of atypical mononuclear cells increases with:
- Autoimmune pathologies.
- Oncology.
- HIV infection.
- Infectious and viral lesions.
- Pathologies of blood.
- Poisoning and prolonged use of medicines.
To determine the level of virotsitov conducted an extensive blood test with the definition of the leukocyte formula. In norm of lymphocytes should be no more than 25-35%, and monocytes 2-6%. In children of childhood, the number of cells is higher than in adults. The lowered level of atypical mononuclears and leukocytes is observed when:
- Liver failure.
- The use of cytostatics.
- Miliary tuberculosis.
- Aplastic anemia.
Their number varies considerably with such pathologies as: blood diseases, poisonings, systemic collagenoses, acute infections. They are responsible for the immune response of the body to various stimuli. Virocytes are capable of differentiation, as they absorb damaged cells, harmful microorganisms and bacteria.
The causes of atypical mononuclear cells
In a healthy body, with normal functioning of all organs and systems, there are no virolets. The causes of atypical mononuclear cells are different. They are detected during a laboratory examination, they are determined as a percentage of the number of leukocyte cells. If the concentration of atypical cells exceeds 10%, then the viral infection is in acute or progressive form. In this case, an additional blood test and medical consultation are performed to clarify the diagnosis.
The main reason for the appearance of virotsitov is infectious and viral diseases. Such ailments are accompanied by fever, an active increase in the liver, spleen and lymph nodes. Mononucleosis can change the quantitative composition of the blood. At the initial stage of the disease, along with an increase in the number of atypical cells, an increase in the number of stab neutrophils is observed, and the number of segmented neutrophils decreases.