Medical expert of the article

New publications
Treatment of primary open-angle glaucoma
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The goal of monitoring patients with primary open-angle glaucoma is to maintain or improve the condition. The doctor and the patient are interested in the functional preservation of the patient's visual organ throughout his or her life. To start or change treatment, it is necessary to prove the presence or absence of the possibility of developing functional disorders due to glaucoma in a given patient. To do this, the doctor must know the stage of glaucoma, the severity of changes at that stage of glaucoma, and the expected duration of glaucoma. For this purpose, it is recommended to use a glaucoma diagram.
The stage of glaucoma is determined using a disc nomogram. The degree of impairment is determined by serial assessments of the history, visual field, and optic disc. The duration of damage from primary open-angle glaucoma is determined by a reasonable assumption about the patient's life expectancy.
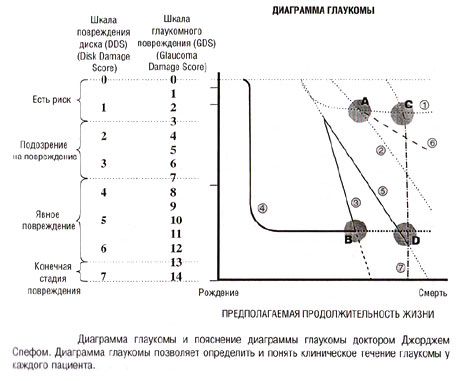
Glaucoma Diagram and Explanation of Glaucoma Diagram by Dr. George Spech. Glaucoma diagram helps to identify and understand the clinical course of glaucoma in each patient.
The y-axis of the diagram represents the stage of glaucoma, and the x-axis represents the expected life expectancy. Each line has a certain slope and bend, and they are displayed in different ways:
- dotted lines represent the slope and curvature of graphs obtained from serial studies such as repeated annual optic disc photography or repeated perimetry;
- solid lines reflect the clinical course of the disease according to the anamnesis data;
- The dotted lines show expected changes in the future.
These hypothetical extrapolated future treatment courses are based on the nature of previous courses and on knowledge of what has happened to the patient since a certain point in the treatment process.
The graph shows the treatment courses of 7 patients with different manifestations of glaucoma.
- The patient at point “A” has weakly expressed glaucoma changes, and presumably still has a third of his life ahead of him.
- The patient at point "B" has severe glaucoma, with approximately a third of his life ahead of him.
- The patient at point “C” has weakly expressed glaucoma changes and has a few years of life left.
- The patient has severe glaucoma at point "D" and has several years of life left.
Patient #1 has a third of his life ahead of him at point "A", and is in the early stage of glaucoma. Approximately a third of his life ago, the patient had an increase in intraocular pressure, and treatment was prescribed. After the treatment was discontinued, no damage to the optic disc or deterioration of the visual fields was observed. It is logical to assume that if intraocular pressure remains at the normal level, the graph will continue according to line #1. By the end of his life, the patient will not develop any glaucoma damage.
Patient #2 at point "A". Minimal glaucoma changes, one third of life left. This patient had a constant increase in intraocular pressure. Early damage to the optic disc and visual field impairment developed. If the disease continues along dotted line #2 without treatment, obvious asymptomatic damage will develop. However, the patient will not go blind for the rest of his life.
Patients #3 and #4 at point "B". Severe glaucoma, approximately one third of life ahead. Patient #3 has rapid progression of changes, blindness will occur long before the end of life. Patient #4, who suffered an eye injury in childhood and who at the same time had decreased vision as a result of steroid-induced glaucoma, has had stable vision for most of his life, so it is logical to expect that the condition will remain stable.
Patients at points "C" and "D" have a few years left to live, but patients at point "C" (like patients #1 and #2 in point "A") have minimal glaucomatous changes, while patients at point "D" (like patient #4 in point "B") have severe glaucoma.
Patient #5 has a clinical course that is similar to that of patient #3 (pronounced glaucoma with rapid progression of changes), but approximately in the middle of life the course of the glaucoma process became less severe. However, without effective intervention, blindness will occur before the end of the patient's life. Let's compare patients #4 and #5, who have the same degree of glaucoma changes at point "D" and the same expected life expectancy (pronounced glaucoma and several years before the end of life). Patient #4 has a stable clinical course of the disease, so there is no need to change the treatment. And patient #5 urgently needs to reduce intraocular pressure.
Patient #6 also has a few years of life left around point "C", but the progression of glaucoma is somewhat slower than in patients #2 and #5. Patient #6 has very minor glaucoma changes, and does not require treatment despite the progression of the disease. Significant glaucoma damage or vision loss will not develop even without treatment, so the patient will not experience any functional impairment throughout his life.
Patient #7's life expectancy at point "C" is several years, but glaucoma is progressing so rapidly that despite the short life expectancy, blindness will occur long before death.
Using a glaucoma chart to define and describe the clinical course of the disease allows the enemy and the patient to understand that:
Patients #1, #4, and #6 do not require treatment. Patient #1 will never develop damage, patient #4 has significant damage but no deterioration, and patient #6 has such a slow progression of the disease that the patient will not feel it for the rest of his life.
Patients No. 3, 5 and 7 urgently require treatment to prevent blindness long before the end of their lives.
The need for treatment in patient #2 is ambiguous. Since this patient will not have any manifestations of glaucoma, treatment may not be necessary. However, some damage will develop, so if damage is undesirable, therapy is recommended.
Appropriate management of a patient with primary open-angle glaucoma involves balancing the risk of pain or loss of function without intervention, the potential benefit of intervention (slowing or stabilizing visual impairment and significant improvement), and the potential risks of intervention.
The only proven effective treatment for primary open-angle glaucoma is to lower intraocular pressure. Guidelines have been developed to determine the amount by which intraocular pressure should be lowered in each case to prevent deterioration, stabilize the condition, or improve it.
Risks and benefits of treatment
Risk of no intervention |
Risk associated with intervention |
Benefits of intervention |
Pain |
Local side effects:
|
Improving visual functions |
Loss of visual functions:
|
Systemic side effects:
|
Stabilization of the course of the disease |
- |
- |
Slowing down the development of pathological processes |
Risk of loss of function without intervention
Short
- No changes in the optic nerve
- No history of blindness due to glaucoma in the family
- Self-care ability
- Quality care available
- Estimated life expectancy is less than 10 years
- Intraocular pressure is below 15 mmHg.
- Lack of exfoliation and changes characteristic of pigment dispersion syndrome
- Absence of cardiovascular diseases
High
- Changes in the optic nerve
- Family history of blindness due to glaucoma or identification of a glaucoma "gene"
- Inability to care for oneself
- Lack of accessible quality care
- Estimated life expectancy is over 10 years
- Intraocular pressure is above 30 mmHg.
- Exfoliative syndrome
- Presence of cardiovascular diseases
Estimated benefit of treatment*
- The expected benefit is greatest when intraocular pressure is reduced by more than 30%
- The expected benefit is possible with a reduction in intraocular pressure by 15-30%
- No expected benefit with intraocular pressure reduction of less than 15%
* In some cases, only stabilization of intraocular pressure is considered beneficial.
Efficiency of reducing intraocular pressure and the risk of developing side effects
Typical decrease in intraocular pressure |
|
| In response to drug therapy | about 15% (range 0-50%) |
| In response to argon laser trabeculoplasty | about 20% (range 0-50%) |
| In response to an operation aimed at increasing filtration | about 40% (range 0-80%) |
The likelihood of developing side effects as a result of treatment |
|
| Drug therapy | 30% |
| Argon laser trabeculoplasty | almost absent |
| An operation aimed at increasing filtration | 60%* |
* The lower the final intraocular pressure, the higher the likelihood of developing side effects from the surgery.
Some physicians recommend target intraocular pressure (IOP) management, which is the level of intraocular pressure at which further damage does not occur. It is important to remember that target intraocular pressure is only a rough guide to treatment. The only effective way to monitor a patient with primary open-angle glaucoma is to assess the stability of the optic nerve head, visual fields, or both. Thus, if the optic nerve and visual field are stable despite an IOP that is higher than the calculated target, it is inappropriate to lower the pressure to the target IOP. Conversely, if the target pressure is reached and the optic nerve and visual field continue to deteriorate, the target pressure is too high, there is another cause for deterioration unrelated to glaucoma, or the neuronal damage is already so severe that progression continues regardless of the IOP level.
Thus, primary open-angle glaucoma is one of the main causes of irreversible blindness worldwide. Diagnosis primarily involves identifying damage to the optic nerve. The goal of treatment is to maintain the patient's health through minimal interventions necessary to slow down the deterioration of visual functions and maintain them at a sufficient level throughout the patient's life. To do this, the attending physician must know the stage of glaucoma, the level of glaucoma changes, and the expected life expectancy of the patient.