Medical expert of the article

New publications
Restenosis
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
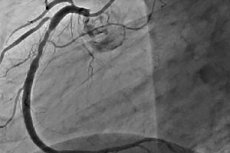
Restenosis is the development of a recurrent narrowing of 50% or more at the site of percutaneous coronary intervention. Restenosis is usually accompanied by recurrent angina, which often requires repeated interventions. As PCI has evolved, the incidence of restenosis has decreased, and its nature has also changed.
 [
[ Restenosis after transluminal balloon coronary angioplasty (TBCA)
After TBCA, the rate of restenosis in the first 6 months is 30-40%. The main mechanism of its development is local negative remodeling of the vessel, which, in essence, is an elastic collapse of the arterial lumen, expanded by the balloon during the procedure. Local thrombus formation and neointimal growth also play a relative role. There are clinical (type 2 diabetes mellitus, acute coronary syndrome (ACS), history of restenosis), angiographic (LAD lesion, small vessel diameter, chronic total occlusion (CTO), long lesion, degenerated venous bypass grafts) and procedural (large residual stenosis, small increase in vessel diameter as a result of balloon inflation) risk factors for restenosis after TBCA. In case of restenosis, a repeated intervention is usually performed. The success of repeated TBCA at the site of restenosis is comparable to the first procedure. However, with each subsequent TBCA for restenosis, the risk of recurrent restenosis increases significantly. After the 3rd attempt, it reaches 50-53%. In addition, with each repeat TBCA, the developing restenosis is more pronounced than the first. Risk factors for restenosis after the second TBCA for restenosis are the early appearance of the first restenosis (60-90 days after the procedure), LAD damage, multivessel damage, type 2 diabetes mellitus, arterial hypertension, unstable angina, and multiple balloon inflations during the first procedure. Given the high frequency of restenosis and the mechanism of its development, coronary stents were introduced into clinical practice, which theoretically should have eliminated negative vessel remodeling after TBCA.
The first studies to demonstrate the efficacy of stenting were the STRESS and BENESTENT studies published in 1993. BENESTENT included 516 patients with newly diagnosed stenosis in coronary arteries greater than 3 mm in diameter, who were randomized into two groups: conventional TBCA (n = 257) and TBCA with stent placement (n = 259). After 3 years, the rate of restenosis during angiography was 32% in the conventional TBCA group and 22% in the stenting group. The relative reduction in the rate of restenosis was 31% (p < 0.01). The stenting group also had a lower need for repeat myocardial revascularization (10 vs. 20.6% in the conventional TBCA group; p < 0.01), which was associated with a lower rate of angina recurrence in the stenting group.
According to the STRESS study (n = 407), the rate of restenosis was also lower in the stenting group (n ~ 205) than in the conventional PTCA group (n = 202) - 31.6 vs. 42.1% (p < 0.01). The advantage of using stents over conventional angioplasty in case of restenosis at the PTCA site was demonstrated in the REST study, in which 383 patients with restenosis were randomized to stenting or repeat percutaneous transluminal coronary angioplasty. Angiographically detected repeat restenosis was 18% lower in the stenting group (18 vs. 5.32%; p < 0.03). Repeated myocardial revascularization, which is an indicator of clinically significant restenosis, was also required significantly less frequently in the group of patients who underwent stenting (10 vs 27%; p < 0.001). Thus, better results with the use of stenting were proven not only in native arteries, but also in the case of intervention for restenosis that developed after TBCA.
Restenosis after bare stent implantation (BSI)
Although uncovered coronary stents have reduced the incidence of restenosis by 30-40% compared to TBCA, 17-32% of patients develop in-stent restenosis even after stenting, requiring repeat revascularization. The mechanism of in-stent stenosis (ISS) development differs from that in TBCA. After stenting, the main contribution to restenosis is neointima formation, rather than negative remodeling, as in TBCA, which is virtually absent at the stent implantation site. Neointima is formed by migration and proliferation of smooth muscle cells producing extracellular matrix, which together with cells makes up the neointima. In addition, thrombus persistence at the stenting site is also important in patients with diabetes.
The main classification of in-stent stenosis (ISS) is the classification proposed by Mehrаn, which includes four types depending on the extent and severity of the lesion: I type ISS - local (< 10 mm in length), II type - diffuse (> 10 mm in length), III type - proliferative (> 10 mm and extending beyond the stent) and IV type - ISS leading to occlusion. The first type is divided into subtypes depending on the location in the stent: 1a - on the bend or between stents, 1b - marginal, 1c - inside the stent, 1d - multifocal.
Risk factors for the development of VRS are interventions on venous bypass grafts, chronic occlusions, ostial lesions, small vessel diameter, presence of residual stenosis, stenting for VRS, small post-procedural vessel diameter, LAD lesion, long stent length, presence of diabetes, implantation of several stents in one lesion. There are indications of the influence of genetic factors, in particular polymorphism of the glycoprotein IIIa gene and mutations of the methylenetetrahydrofolate reductase gene - the gene encoding interleukin-1. In the case of development of marginal stent restenosis, the main risk factor is a pronounced atherosclerotic lesion in the stented segment.
Restenosis occurs predominantly during the first 6-8 months after percutaneous coronary intervention. Most patients develop clinical symptoms at about the same time. VRS is usually manifested by recurrent angina. Unstable angina occurs less frequently (11-41% of cases). AMI develops in 1-6% of patients. Thus, the most common cause of angina during the period of 1-6 months after stenting is the development of VRS, which, as a rule, requires repeated revascularization. There are several methods for treating VRS. Conventional TBCA can be performed, which leads to further stent expansion (56% contribution to the final increase in vessel diameter) and pushes the neointima through the stent cells (44% contribution to the final increase in diameter). However, residual restenosis is observed in most cases at the site of the intervention (on average 18%). In addition, after TBCA, repeat revascularization is required in 11% of cases, more often in patients with multivessel disease, low LVEF, in case of interventions on venous bypass grafts or early occurrence of the first VRS. The risk of developing repeated VRS after TBCA also depends on the type of lesion and ranges from 10% in case of local restenosis to 80% in case of intra-stent occlusion. Implantation of the LES at the site of VRS does not reduce the risk of its recurrence compared to TBCA alone.
The second method of treating VRS is brachytherapy, which involves introducing a radioactive source into the lumen of the coronary artery, preventing the proliferation of smooth muscle cells and, accordingly, reducing the risk of restenosis. However, the high cost of equipment, the technical complexity of the procedure, and the increased incidence of late stent thrombosis (LT) have almost completely excluded brachytherapy from clinical use.
A revolutionary moment in the treatment of VRS was the introduction of drug-eluting stents. Compared with LES in native arteries, they reduce the risk of VRS by 70-80%. The first data on the effectiveness of DES in patients with already developed VRS were obtained in the TAXUS III registry of patients, in which, when using SPG1 in such patients, the frequency of VRS recurrence was only 16% after 6 months, which is lower than in the previously mentioned studies with TBCA. In the TRUE registry, which included patients after SES implantation for LES restenosis, after 9 months, repeat revascularization was required in less than 5% of patients, mainly with diabetes mellitus and ACS. The TROPICAL study compared the frequency of repeated restenosis in patients after DES implantation at the site of restenosis with the data of the GAMMA I and GAMMA II studies, in which brachytherapy was used as a treatment method. After 6 months, The incidence of recurrent restenosis was significantly lower in the SPS group (9.7 vs 40.3%; p < 0.0001). It is important to note that the incidence of stent thrombosis and myocardial infarction was also lower in the SPS group (TS 0.6 vs 3.9%; p = 0.08; MI - 1.8 vs 9.4%; p = 0.004). The advantage of SPS over brachytherapy was confirmed in the randomized SISR study, in which 384 patients with developed VRS in the NSC were randomized to brachytherapy or SPS implantation groups. After 9 months, the need for repeat revascularization was higher after brachytherapy (19.2%) than in the SPS implantation group (8.5%), which reflected a more frequent recurrence of restenosis. After 3 years, the advantage of SPS in terms of reducing the need for repeat revascularization due to recurrent stent restenosis remained (19 vs 28.4%). There was no significant difference in the incidence of thrombosis between the groups.
The main factors for the development of recurrent VRS in patients with LES in the case of SPS implantation are a small vessel diameter (< 2.5 mm), diffuse type of restenosis, and the presence of chronic renal failure requiring hemodialysis. In the randomized study TAXUS V ISR, SPS also demonstrated high efficiency in the treatment of VRS, reducing the rate of recurrent restenosis by 54% compared to brachytherapy.
Randomized trials comparing the efficacy of TBCA for VRS and DES implantation were also conducted. In the randomized RIBS-II trial, after 9 months, repeat restenosis was 72% less common after DES implantation than after TBCA, which reduced the need for repeat revascularization from 30 to 11%. The ISAR DESIRE trial compared the efficacy of TBCA for VRS with SPP or SPS implantation. After 6 months, it turned out that both DES were more effective in preventing repeat restenosis than TBCA (its incidence was 44.6% with TBCA, 14.3% in the SPS group, and 21.7% in the SPS group), which reduced the need for repeat revascularization. In a direct comparison of SPP and SPS, it was found that SPS reduced the need for repeat revascularization significantly more effectively than SPP (8 vs. 19%). Thus, DES implantation reduces the incidence of recurrent LES VRS compared with both TBCA and brachytherapy, which reduces the number of repeat PCIs and therefore makes their implantation the procedure of choice in such patients.
Restenosis after drug-eluting stent (DES) implantation
Despite the 70-80% decrease in the incidence of in-stent stenosis when using DES compared to LES, they could not completely exclude the development of this iatrogenic consequence of stenting. Its overall incidence remains on average less than 10%. In addition to the quantitative decrease in the incidence of restenosis, they also significantly changed the type of restenosis that occurs. Thus, after DES implantation, restenosis is usually focal. Clinically, as in the case of LES, it most often manifests itself as a relapse of stable angina (77%), less often (8%) it is asymptomatic. In 5% of cases, it manifests itself as unstable angina, and in 10%, its first symptom is non-Q-wave myocardial infarction. The main factors in the development of DES restenosis are type 2 diabetes mellitus, small vessel diameter, and the extent of the lesion. There are no clear recommendations for the management of such patients. Alternative options are re-implantation of a DES (of the same type or a different one), TBCA, or brachytherapy. The average rate of re-restenosis with a second DES is 24%, and it is the same whether the same type of DES is implanted or a different one.