Medical expert of the article

New publications
Parotid salivary gland
Last reviewed: 07.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The parotid salivary gland (glangula parotidea) is paired, with a serous type of secretion. It has an irregular shape, covered externally by a thin capsule. The mass of the gland is 20-30 g.
The parotid salivary gland, its larger part is located on the outer surface of the branch of the lower jaw, the smaller part is in the retromaxillary fossa formed by the branch of the lower jaw, the internal pterygoid muscle, the mastoid process, the sternocleidomastoid muscle, the posterior belly of the digastric muscle, the lower wall of the external auditory canal. The shape of the gland is very diverse, but many authors find that it is similar to a triangular pyramid, although in reality the parotid salivary gland is difficult to compare with anything.
The parotid salivary gland has three surfaces: external, anterior, posterior, and two bases or, in the words of many authors, "two poles." The anterior edge of the gland somewhat covers the external surface of the masseter muscle, the posterior edge - the sternocleidomastoid muscle; the lower pole often reaches the angle of the lower jaw, and the upper pole sometimes reaches the zygomatic arch.
The parotid salivary gland is enclosed in a sheath formed by the parotid-masticatory fascia, which is the superficial leaflet of the proper fascia of the face. This sheath, together with the masseter muscle, is attached at the top to the zygomatic bones and zygomatic arch, and at the bottom to the outer surface of the angle of the mandible. At the posterior edge of the masseter muscle, the masseter fascia splits and embraces the portion located on the outer surface of this muscle. In front, the proper fascia is a dense leaflet, from which processes penetrate into the thickness of the gland and divide it into lobules. Along the course of the parotid duct, the fascia thickens and contains accompanying vessels and, sometimes, an additional lobe of the gland. The bed of the gland is a space that is limited by the leaves of the parotid-masticatory fascia. The inner leaflet of the fascia of the gland is formed by the sheaths of the sternocleidomastoid and digastric muscles (posterior belly), the sheaths of the muscles extending from the styloid process; in front - the fascial sheath of the internal pterygoid muscle, below and inside - the sheaths of the stylohyoid and digastric muscles (anterior belly). The upper surface of the gland, facing the external auditory canal, and the inner surface of the pharyngeal process of the gland are not covered by fascia and are separated by loose tissue. The parotid salivary gland with a spur enters the gap between the auditory canal and the capsule of the temporomandibular joint. In the area of the pharyngeal process, in the lower part, where the inner surface faces the posterior belly of the digastric and stylohyoid muscles, there is also a strong fascia. The part of the inner surface of the gland without fascial cover is adjacent to the tissue of the peripharyngeal space. The parotid-masticatory fascia passes into the fascial formations of adjacent structures (outside - into the superficial fascia of the neck, behind - into the prevertebral fascia, inside - into the stylopharyngeal aponeurosis and vascular sheath). The thickness of the capsule depends on the age and sex of the person.
The skin is easily displaced, underneath it there is a thin layer of subcutaneous fat tissue surrounding the outer leaflet of the gland fascia and passing into the tissue of adjacent areas, which leads to the unimpeded spread of the tumor infiltrate in all directions. The deep leaflet of the parotid masseteric fascia separates the gland from the lateral wall of the pharynx, the posterior belly of the digastric muscle, from the muscles and ligaments attached to the styloid process, from the posterior surface of the internal pterygoid muscle.
At the posterior edge of the gland, the inner leaflet of the fascia merges with the outer one, and at the angle of the lower jaw, both leaves form a strong partition separating the lower pole from the submandibular.
The fascial sheaths of the vessels and nerves are fused with the capsule of the gland, so no defects are left in the capsule at the sites of their entry or exit. However, the possibility of the pathological process spreading is described along the external carotid artery into the area of the carotid triangle of the neck, and along the internal maxillary artery - into the maxillary-pterygoid fissure of the masticatory space.
At the anterior edge, above the parotid duct, there is sometimes an additional lobe measuring 1-2 cm in diameter. It occurs in 10-20% of individuals and can be a source of tumor development.
The parotid salivary gland secretes its secretion from the parotid salivary duct. Usually it is main and receives lateral canals (from 7 to 18) on its way. In some cases it is formed by the fusion of two ducts of almost equal diameter, sometimes it has a branching structure. The parotid duct emerges at the border of the upper and middle thirds and is directed obliquely upward and forward, and then, turning downwards, goes horizontally along the outer surface of the masseter muscle. At its edge, the duct bends inward, obliquely penetrates the fatty tissue and the buccinator muscle. Then, for 5 cm, the duct is located along the mucous membrane of the cheek and opens in the vestibule of the mouth at the level of the upper second molar or between the first and second upper molars. The opening of the parotid duct has a rounded shape or the shape of a narrow slit, often located on an elevation in the form of a papilla. The diameter of the duct is 3 mm, its length is from 15 to 40 mm. The duct of the accessory lobe of the gland flows into the parotid duct, which gives many researchers a reason not to call it an independent gland. Often the anterior edge protrudes far forward and almost reaches the anterior edge of the masseter muscle. In such cases, the beginning of the parotid duct is masked by the gland.
Most anatomists and surgeons define the projection of the parotid duct along the line connecting the tragus of the auricle and the corner of the mouth. In children, the duct is often projected along the line: corner of the mouth and the lobe of the auricle.
The parotid salivary gland is penetrated by numerous blood and lymphatic vessels, nerves and lymph nodes. In most cases, the vessels are located in the thickness of the gland, closer to its anterior surface. Sometimes the vessels pass along the inner surface of the gland. The largest blood vessel is the external carotid artery, which is tightly fused with the parenchyma of the gland and here it divides into its terminal branches: the posterior auricular, superficial temporal, transverse facial and maxillary. The external jugular vein is located outside the external carotid artery. The posterior auricular and transverse facial veins flow into it. Venous blood flows out through the retromandibular vein, which is formed by the confluence of the superficial temporal and maxillary veins.
Innervation: sensory - parotid branches of the auriculotemporal nerve, secretory (parasympathetic) - fibers of the auriculotemporal nerve (from the otic ganglion), sympathetic - from the external carotid plexus.
The parotid salivary gland is innervated by the parotid branches of the auriculotemporal nerve; secretory fibers come from the otic ganglion; sympathetic nerves accompany the superficial temporal artery. The accessory lobe and parotid duct are innervated by branches of the facial nerve.
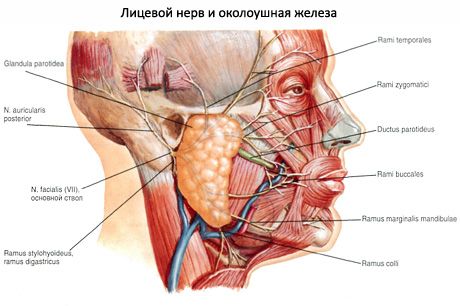
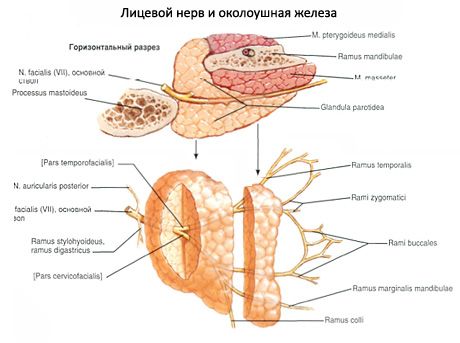
The parotid salivary gland is penetrated by the extracranial part of the facial nerve, which is the VII pair of cranial nerves. The facial nerve exits the skull through the stylomastoid foramen. The length of the nerve to the posterior edge is on average 10 mm. During surgery, as some surgeons note, this section of the nerve can be lengthened by pulling the lower jaw forward. The facial nerve most often penetrates the middle third of the gland. In the parenchyma of the gland, the nerve passes along a common trunk of approximately 15 mm, always outward from the external carotid artery and external jugular vein. Then the facial nerve divides into two branches. One branch goes horizontally, continuing the course of the common trunk, and divides into three branches. The other branch is directed downwards almost at a right angle, passes in the parenchyma of the gland the greatest distance (about 20 mm) and also divides into two branches. Very rarely, the facial nerve divides before entering the organ. In the gland itself, the nerves widely anastomose with each other, which creates significant difficulties when isolating them during surgery. Five main branches of the facial nerve emerge from the gland tissue to the facial muscles: temporal, zygomatic, buccal, mandibular marginal, cervical.
According to the general opinion of researchers, the topography of the five main branches of the facial nerve is extremely variable. Various variants of division of the facial nerve are described. As a landmark in practical surgery for finding the mandibular branch directed to the corner of the mouth, the location of the parotid duct can be used, and for finding the zygomatic branch - a straight line connecting the corner of the eye with the lobe of the auricle.
The parotid salivary gland is also penetrated by the auriculotemporal nerve, which is a branch of the mandibular nerve. The auriculotemporal nerve penetrates the gland slightly below and behind the articular process of the mandible and breaks up into many small trunks, the topography of which is complex. One of the branches accompanies the superficial temporal artery, the other branches form a thickening in the form of a plate, from which numerous thinnest branches depart in different directions (including to the skin of the auricle and the external auditory canal), which anastomose with the sympathetic plexus of the external carotid artery.
The parotid salivary gland has a superficial and a deep part. The superficial part corresponds to the part of the gland that is located on the masseter muscle. The deep part occupies a depression behind the branch of the lower jaw. The facial nerve and its connective tissue sheath, passing through the thickness of the gland, are a landmark, outside of which is the superficial part, inside - the deep part.
Blood supply: parotid branches of the surfaces of the temporal artery, venous outflow into the retromandibular vein.
Lymph drainage: into the superficial and deep parotid lymph nodes.
 [
[ What do need to examine?