Medical expert of the article

New publications
Nasal scleroma
Last reviewed: 12.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Scleroma is a chronic infectious disease of the respiratory tract, characterized by the appearance of dense infiltrates in their mucous membrane, a slow progressive course, the appearance in the final stage of disfiguring scars that deform and stenose the affected anatomical formations. The causative agent of the disease is considered to be the Volkovich-Frisch bacillus. The disease is slightly contagious, characterized by its distribution in epidemic foci of Belarus, Ukraine, countries of Eastern and Central Europe. The incubation period for rhinoscleroma is unknown. The disease usually develops gradually, lasts for years, sometimes decades. Exacerbation of the process is observed during pregnancy. Women get sick somewhat more often than men and children. The disease often begins at the age of 11-30 years. Most people with rhinoscleroma live in rural areas.
Scleroma has been known since the Middle Ages. It was considered a special form of syphilis, tuberculosis, found similarities with sarcoma or cancer, and only in the second half of the 19th century it began to be studied as a separate nosological form. One of the first to describe the clinical picture of scleroma was V.A. Karavaev (1911-1892) in 1858 - an outstanding Russian and Ukrainian surgeon, ophthalmologist and rhinologist, one of the founders of ophthalmology and rhinoplasty. In 1870, F. Hebra - an outstanding Austrian dermatologist, the head of the Austrian dermatological school in the 19th century - proposed to call this disease rhinoscleroma, since the 10 cases of this disease described by him concerned lesions of the external nose. In 1888, N.M. Volkovich gave this disease a new name - scleroma of the respiratory tract, since it affects not only the nose, but the entire respiratory tract, right down to individual bronchi. In 1876, J. Mikulicz found in scleroma infiltrates and described peculiar foamy (light) cells, called Mikulicz cells. In 1876, the Austrian bacteriologist A. Frish discovered the causative agent of scleroma - a gram-negative encapsulated rod, a pure culture of which was isolated several years later and its morphological features were described by N.M. Volkovich.
 [
[ Pathological anatomy
There are 4 stages in the development of scleromatous infiltrate.
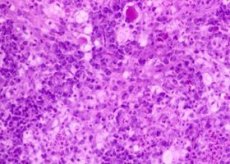
- Stage I is characterized by thickening of the nasal mucosa (or other localization in the upper respiratory tract) and the formation of brown-red or dark-red infiltrates, which initially have a soft-elastic consistency, then a dense cartilaginous consistency, and are not prone to decay. At this stage, the infiltrate contains inflammatory cells (lymphocytes, plasma cells, histiocytes, and neutrophils). Among these formed elements, larger (20-50 μm), vacuolated cells with an eccentrically located nucleus and protoplasm rich in chromatin (Mikulicz cells) begin to stand out.
- In stage II, histiocytic infiltration begins to predominate, and the process of transformation of histiocytes into Mikulicz cells develops. In and around these cells, a huge number of Volkovich-Frisch rods and peculiar Russell bodies consisting of hyaline, 30-40 µm in size, are found.
- In stage III, a decrease in the number of histiocytes, an increase in the number of Mikulicz cells, connective tissue elements and the formation of collagen fibers are observed.
- At this stage, the process of scarring of scleromatous infiltrates begins, which reaches its apogee in stage IV, during which Mikulicz cells and histiocytes disappear and are replaced by collagen fibers, the number of which increases with the formation of dense scar tissue. This process leads to persistent narrowing of the lumen of the respiratory tract (partial or complete obstruction of the nasal passages, with other localization in the respiratory tract - to stenosis of the larynx, trachea and bronchi.
As a rule, scleromatous lesions begin to develop in the mucous membrane of the nose. Their further spread can occur both in an ascending and descending direction, affecting the nose, lips, sometimes the corners of the mouth, uvula, nasopharynx, soft and hard palate, upper respiratory tract, rarely - lacrimal canals, auditory tubes, middle ear and conjunctiva of the eye.
Symptoms of nasal scleroma
At the initial stage, there are no significant complaints. Pathological changes in the nasal mucosa do not cause pain and proceed without general reactions. The nasal mucosa presents a picture of banal chronic catarrhal inflammation. The development of the inflammatory process causes itching in the nose, frequent sneezing, mucous or mucopurulent discharge. The nasal mucosa has a pale pink color. At this stage, the disease is often masked by allergic manifestations, but the antiallergic drugs used do not stop the development of the disease, and after several years, atrophy of the nasal mucosa and nasal conchae develops, as a result of which the nasal passages expand. Then, crusts with an unpleasant, specific "sweetish" odor appear in the nasal cavity, different from ozenous and syphilitic. Nosebleeds become more frequent, hyposmia develops. At this stage, rhinoscleroma is often confused with ozena, but upon closer examination with a microscope, small papillary thickenings of the mucous membrane can be seen on the nasal mucosa either in the anterior parts of the nose or in the choanae. Most often, these changes occur in places of physiological narrowing of the upper respiratory tract. The period of the peak of the disease is characterized by the appearance and rapid increase of scleroma infiltrates, which lead to difficulty and then to complete shutdown of nasal breathing, a decrease in olfactory acuity to complete anosmia.
Depending on the localization of the process, rhinoscleroma can acquire various visual aspects. Galloping forms of scleroma are rare, sometimes with spread to the nasal bones, hard palate, alveolar process. The development of scleroma infiltrates at the level of the nasal valve leads to nasal obstruction, and damage to the external nose sometimes occurs as a rhinophyma-like scleroma. Other anatomical formations are rarely affected. The formation of coulisse-like strands in the nasopharynx sometimes leads to its almost complete separation from the pharynx. Spreading to the soft palate, the process leads to its wrinkling and deformation, which causes difficulty in swallowing, especially liquid food, and phonation disorder.
The general condition of the patient with scleroma remains satisfactory and is disturbed only by difficulty breathing due to the development of chronic general hypoxia. In this case, patients often have noticeably disturbed basal and nitrogen metabolism, hypochromic anemia, lymphocytosis, eosinophilia develop, and in some cases monocytopenia is observed. ESR is constantly elevated.
Evolution and complications
The disease develops very slowly, over a number of years and even decades. Cases of spontaneous recovery are unknown, while the use of even the most active and modern treatment does not guarantee a complete cure; we can only talk about temporary remission or suspension of the disease. The sclerotic process can spread either along the length or by "jumping" through healthy areas of the mucous membrane, affecting individual segments, starting from the nose and reaching the choanae, nasopharynx, auditory tubes, pharynx, larynx, trachea and bronchi. The paranasal sinuses are rarely affected.
The most common complications are airway obstruction, chronic hypoxia, pneumonia, and pulmonary tuberculosis. In these cases, patients reach extreme levels of exhaustion and die either from irreversible metabolic changes or from asphyxia (even with timely tracheotomy), if the process has caused obstruction of the trachea and bronchi.
Diagnosis of nasal scleroma
In the initial stage of the disease, diagnosis is difficult, since the inflammatory phenomena in the nose are very similar to those in banal catarrhal rhinitis. However, in all cases of prolonged "runny nose", accompanied by even barely noticeable productive processes in the mucous membrane of the nose, a specific smell from the nose, taking into account the epidemiological history, the presence of rhinoscleroma should be suspected. Further examination of the patient should pursue the goal of identifying this disease. However, it should be borne in mind that laboratory testing does not always give a positive result, but even in the absence of the latter, scleroma cannot be excluded. Diagnosis is facilitated at the stage of pronounced clinical and morphological manifestations. Endoscopy of the upper respiratory tract, biopsy, radiography, agglutination reaction of non-encapsulated strains of the Frisch-Volkovich bacillus, skin allergic reactions, and possibly even the complement fixation reaction of the patient's serum and the serum of rabbits immunized with the Frisch-Volkovich bacillus are important for establishing the diagnosis. According to a number of authors, a positive Bordet-Zhangu reaction is the most constant in scleroma, but it cannot be considered specific for this disease. Sowing scleroma material (nasal discharge, crushed biopsy specimens) on agar-agar allows isolating the Frisch-Volkovich bacillus culture in 80-90% of cases. Although rare, microscopic examination of scleroma tissues may reveal giant vacuolated Mikulicz cells, fuchsinophilic Russell bodies, and numerous plasma cells.
What do need to examine?
Differential diagnostics
Rhinoscleroma, like scleroma of any other localization, at different stages of development may have a certain similarity with various diseases. At the debut stage, it is differentiated from catarrhal or simple atrophic rhinitis, ozena, syphilitic lesions. Cases of combined diseases of ozena and scleroma have been described. At the mature stage, scleromatous infiltrates can be taken for manifestations of any disease characterized by the appearance of infiltrates and tumors, including tuberculosis, syphilis, leprosy, benign and malignant tumors, etc.
Treatment of nasal scleroma
Numerous treatment methods proposed during the 19th and 20th centuries yielded virtually no positive results. Among these methods, the following should be mentioned: biological (vaccine therapy, autoimplantation of scleromatous tissue, irradiated blood transfusions), chemical (iodine preparations, carbolic and chromic acid, zinc chloride, neosalvarsan, quinine and bismuth preparations, etc.), physical (diathermocoagulation, radiation therapy), mechanical (bougienage), surgical (removal of cicatricial stenosis, plastic surgery, tracheotomy). At present, relatively favorable results are obtained by treatment with streptomycin (locally in the form of ointments and aerosols, parenterally in long courses of 2-3 months and X-ray therapy. In addition, auromycin, terramycin and intravenous infusions of a 5% solution of PAS are used with encouraging results. The anti-sclerotic effect of cortisone in scleroma is not manifested.
General treatment is prescribed in connection with metabolic disorders: calcium preparations, vitamin therapy, preparations that normalize acid-base balance, complete carbohydrate and protein nutrition.
The prognosis for complete recovery in advanced cases is unfavorable.