Medical expert of the article

New publications
Scleroma
Last reviewed: 05.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Scleroma (rhinoscleroma, scleroma of the respiratory tract, scleroma disease) is a chronic infectious disease caused by the Frisch-Wolkovich bacillus (Klebsiella pneumoniae rhinoscleromatis), characterized by the formation of granulomas in the walls of the upper respiratory tract (mainly the nose), which subsequently undergo fibrosis and cicatricial wrinkling, leading to stenosis of individual sections of the respiratory tract.
ICD-10 code
J31.0. Chronic granulomatous rhinitis.
Epidemiology of scleroma
The disease is spread all over the world in the form of large, medium and small foci. Endemic for scleroma are considered to be Central and Eastern Europe, including Western Ukraine and Belarus, Italy, Central and South America. Africa, Southeast Asia, Egypt, India, the Far East. The area endemic for scleroma has certain characteristics. First of all, these are low-lying areas of the earth with sparse forests and swamps, where the population mainly lives engaged in agriculture. Scleroma is more common in women. Cases of scleroma have been noted in some isolated villages. Often, members of one family are affected, where 2-3 people are sick. The disease is associated with low socio-economic status, and in developed countries, for example, the USA, it is very rare. The situation may change due to population migration.
To date, the exact mechanisms and conditions of human infection have not been established. Most researchers believe that the infection is transmitted from a patient by contact and through shared items. It has been noted that during bacteriological examination of material from the affected organs of family members with scleroma, Klebsiella pneumoniae rhinoideromatis with the same characteristics is isolated.
Causes of scleroma
At present, the infectious nature of the disease is beyond doubt. This is confirmed by the natural focal spread of the disease and the contact route of infection transmission. The causative agent of scleroma is the gram-negative Frisch-Volkovich papilla (Klebsiella pneumoniae rhinoscieromatis), first described in 1882 by Frisch. Klebsiella pneumoniae rhinoscleromatis is detected in all patients, especially in the active period of infiltrate and granuloma formation, dystrophy of the mucous membrane.
Pathogenesis of scleroma
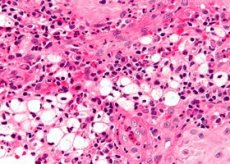
Klebsiella pneumoniae rhinoscleromatis is classified as an encapsulated microorganism. The presence of a capsule protects the bacilli and inhibits the process of phagocytosis by macrophages, which leads to the formation of specific large Mikulicz cells, distinguished by a peculiar foamy structure of protoplasm. At the onset of the disease, local disorders in the respiratory tract are not observed. In the second, active period, changes develop in various parts of the respiratory tract, which can occur in the form of dystrophic or productive phenomena with the formation of an infiltrate, granuloma in various parts of the respiratory tract. The epithelium covering the sclerotic infiltrate is usually not damaged. Infiltrates can have endophytic growth, spreading to the skin of the external nose, causing its deformation, or exophytic, leading to respiratory dysfunction (in the nasal cavity, nasopharynx, larynx and trachea).
The final stage of transformation of scleroma infiltrate is formation of a scar, which sharply narrows the lumen of the airway cavities in limited areas or over a considerable distance, leading to stenosis and sharp impairment of the functional state. In the scarring stage, connective tissue elements prevail, scleroma rods and Mikulich cells are not detected.
Scleroma is characterized by the transition of granuloma immediately to the cicatricial stage, the absence of destruction and disintegration of the infiltrate. Bone tissue is never affected by scleroma.
Symptoms of scleroma
At the onset of the disease, patients complain of weakness, fatigue, headache, loss of appetite, sometimes thirst, and arterial and muscular hypotension. Local changes in the respiratory tract are not observed.
Noteworthy is the decrease in tactile and pain sensitivity of the mucous membrane of the respiratory tract. Such symptoms may be observed for a long time and have no specific character. However, given the constancy and stability of these manifestations, one can suspect scleroma and refer the patient for a specific bacteriological examination. During this period, Klebsiella pneumoniae rhinoscleromatis can be detected in the material from any part of the respiratory tract, most often from the mucous membrane of the nasal cavity.
Diagnosis of the disease at an early stage can be of decisive importance in relation to the effectiveness of treatment, dispensary observation and a positive prognosis.
In the second, active period, changes are observed in various parts of the respiratory tract, in the form of dystrophic or productive forms. It is possible to detect atrophy of various parts of the mucous membrane of the nose, pharynx, larynx, the formation of viscous mucus and dry crusts. In the productive form, the formation of an infiltrate, granuloma in various parts of the respiratory tract is noted. The sizes of the affected areas vary from limited small rashes to continuous tumor-like formations without destruction of the mucous membrane, without the formation of atresia and synechia at the points of contact of infiltrates of opposite parts of the mucous membrane. Infiltrates can have endophytic growth and spread to the skin of the external nose, causing its deformation, or exophytic, leading to a violation of the respiratory function (in the nasal cavity, nasopharynx, larynx and trachea).
In addition to respiratory failure, reflex, protective, resonant dysfunctions develop, and the sense of smell is significantly reduced. Difficulty breathing (laryngeal stenosis), hoarseness, and a decrease in the protective function are noted.
Infiltrates of the nasal cavity are most often observed in the anterior sections at the level of the anterior end of the inferior turbinates and on the opposite sections of the nasal septum. They are rare in the middle section of the nasal cavity. Infiltrates are most often located in the choanae area with a transition to the soft palate and uvula, the upper sections of the tonsil arches, leading to their deformation. When infiltrates become cicatrized, incomplete nasopharyngeal atresia is formed.
It is typical that in one patient infiltrates and cicatricial changes can be simultaneously located in different parts of the respiratory tract. Sometimes after granuloma cicatrization, one can observe the formation of an infiltrate in the adjacent area of the mucous membrane. In the larynx, infiltrates are more often localized in the subglottic section, causing a violation of the respiratory, protective and voice-forming functions.
It should be noted that in a number of patients with scleromatous infiltrates, areas with signs of dystrophy of the mucous membrane (mixed form) are found.
The clinical picture of scleroma in the active stage (obvious signs of the disease) depends on the form of the process. In the case of atrophy, patients complain of dryness in the nose, viscous, thick discharge, crust formation, decreased or lost sense of smell. Sometimes a large number of crusts in the nasal cavity is accompanied by the appearance of a sweetish-cloying smell, which is felt by others, but differs from that in ozena. During an objective examination of the patient, areas of atrophic mucous membrane and crusts are visible.
In the case of the formation of a scleroma granuloma, the mucous membrane has dense, different-sized infiltrates of a yellowish or grayish-pink color, covered with intact epithelium. When cicatricial changes occur, patients complain of dysfunction of the nose and larynx. The scleroma process in the larynx can also lead to stenosis and require urgent tracheotomy.
Classification
The scleroma process proceeds slowly, over years and decades, and goes through several periods of its development: initial (latent), active, regressive. The initial stage is characterized by non-specific symptoms of rhinitis. Distinctive features of the active period are infiltration or atrophy. The formation of scars indicates the regressive stage.
Scleroma mainly affects the respiratory tract, but the process can occur in isolation and in any organ or totally, affecting the nose, pharynx, larynx, trachea and bronchi in any form of manifestation, which is also used in the classification.
The main forms of the process are: dystrophic, productive and mixed.
Screening
In case of chronic rhinitis, especially in areas endemic for scleroma, it is necessary to remember the possible damage of the nasal mucosa by Klebsiella pneumoniae rhinoscleromatis and use additional specific research methods.
Diagnosis of scleroma
Diagnosis of the disease is based on the analysis of the patient's medical history and complaints. It is necessary to pay attention to: the place of residence, assessing the natural focal nature of the development of scleroma: the presence of patients among family members. It is important to assess the patient's age, since the disease is often detected at 15-20 years. In children, the scleroma process is more often localized in the larynx and can lead to its stenosis.
Particular attention should be paid to the general complaints of the patient (weakness, fatigue, headache) under the above circumstances (endemic focus, young age, presence of scleroma diseases in the locality or family.
With obvious manifestation of scleroma in the respiratory tract, complaints are determined by the form of the disease (dryness, crusts, difficulty breathing, hoarseness, etc.).
 [ 11 ], [ 12 ], [ 13 ], [ 14 ], [ 15 ]
[ 11 ], [ 12 ], [ 13 ], [ 14 ], [ 15 ]
Physical examination
If scleroma is suspected, a thorough examination of all parts of the respiratory tract should be carried out using generally available methods used in otolaryngology, as well as, if possible, modern endoscopic methods (fibroendoscopy of the nasal cavity and nasopharynx, pharynx, larynx, trachea and bronchi). The functional state of the respiratory tract must be determined.
Laboratory research
It is necessary to examine the microflora from different parts of the respiratory tract.
In doubtful cases, in the absence of growth of Klebsiella pneumoniae rhinoscleromatis, specific serological reactions can be used. Also conducts a histological examination of biopsy material.
Instrumental research
The diagnosis can be facilitated by the use of endoscopic and radiological examination methods, in particular CT.
Differential diagnosis of scleroma
Differential diagnostics of scleroma is carried out with granuloma processes in tuberculosis, syphilis, Wegener's granulomatosis. Scleroma differs from the listed diseases by the absence of destruction and disintegration of the infiltrate, as well as the transformation of the granuloma directly into scar tissue. Bone tissue is never affected by scleroma. Klebsiella pneumoniae rhinoscleromatis is found on the surface of the mucous membrane and under the epithelial layer and thicker than the granuloma, together with specific large Mikulicz cells and freely lying hyaline Russell bodies. The epithelium covering the scleroma infiltrate is usually not damaged.
[ 16 ], [ 17 ], [ 18 ], [ 19 ], [ 20 ], [ 21 ], [ 22 ]
Indications for consultation with other specialists
In case of deformation of the external nose due to the spread of sclerotic infiltrates to the skin of the wings of the nose, a consultation with a dermatologist is indicated; if the lacrimal ducts are involved in the process, an ophthalmologist consultation is necessary; in the initial stage of the disease with general manifestations (weakness, fatigue, headaches, etc.), a consultation with a therapist is necessary.
Goals of treatment for scleroma
The goals of treatment are to eliminate the pathogen, reduce inflammation, prevent respiratory failure, and remove infiltrates and scars. Currently, these measures can lead to recovery at any stage of the disease.
Indications for hospitalization
Indications for hospitalization include the need for complex treatment of scleroma, including surgical treatment, as well as severe respiratory dysfunction requiring bougienage, and in some cases tracheotomy or laryngofissure.
Non-drug treatment
Vugulation (crushing) of infiltrates, anti-inflammatory R-therapy with doses from 800 to 1500.
Drug treatment of scleroma
Streptomycin is prescribed at a dose of 0.5 g 2 times a day for a course of treatment lasting 20 days (maximum total dose - 40 g).
Surgical treatment of scleroma
Surgical excision of infiltrates and scars.
Further management
Patients with scleroma require dispensary observation and, if necessary, repeated courses of drug therapy. It may be necessary to replace medications and eliminate new infiltrative formations by means of bougienage, crushing, X-ray therapy, etc.
The period of incapacity depends on the degree of respiratory dysfunction and the methods of elimination taken, and is approximately 15-40 days.
It is necessary to pay attention to employment and disability assessment.
The patient is advised to observe personal hygiene rules.
Prevention of scleroma
Preventive measures should be aimed at preventing the possibility of transmitting the infection from a sick person. This involves improving living conditions, increasing well-being, observing the rules of general and individual hygiene, changing the natural conditions in the affected area. The measures visible in this direction in some areas in recent years have given a significant decrease in the number of cases of scleroma.