Medical expert of the article

New publications
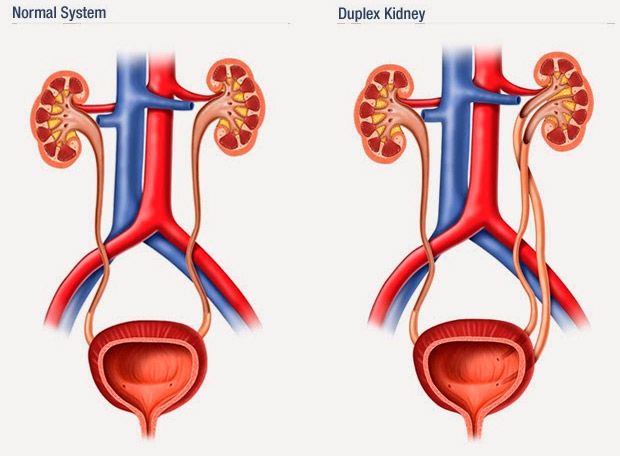
Kidney doubling
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Causes kidney doublings
Kidney doubling occurs when two foci of differentiation induction are formed in the metanephrogenic blastema. In this case, two calyceal-pelvic systems are formed, but complete separation of the blastemas does not occur, and therefore the kidney is covered with a common fibrous capsule. Each half of the doubled kidney has its own blood supply. Renal vessels can branch off separately from the aorta, or they can form a common trunk, dividing at the renal sinus or nearby. Some intrarenal arteries pass from one half to the other, which can be of great importance during resection of the kidney.
Symptoms kidney doublings
Most often, the upper half is underdeveloped, very rarely both halves are functionally identical or the lower half is underdeveloped. The underdeveloped half resembles kidney dysplasia in its morphological structure. The presence of parenchymatous renal dysplasia in combination with urodynamic disorders due to the splitting of the ureter creates the prerequisites for the occurrence of diseases in the abnormal kidney.
Most often, the symptoms of kidney duplication duplicate the symptoms of the following diseases: chronic (53.3%) and acute (19.8%) pyelonephritis, urolithiasis (30.8%), hydronephrosis of one of the halves (19.7%). Kidney duplication can be suspected by ultrasound, especially with dilation of the upper urinary tract.
Where does it hurt?
Forms
 [ 10 ], [ 11 ], [ 12 ], [ 13 ], [ 14 ]
[ 10 ], [ 11 ], [ 12 ], [ 13 ], [ 14 ]
Accessory (third) kidney
An additional (third) kidney is one of the rarest anomalies of this organ. The defect is almost always unilateral. Its origin is similar to the genesis of kidney duplication, but too rapid differentiation leads to a complete separation of two metanephrogenic blastemas and the formation of two kidneys. An additional kidney always has its own fibrous capsule, blood supply system, renal pelvis and calyces system, and ureter, which often opens with an additional third orifice into the urinary bladder below and medially to the two main orifices, but can also merge with the ureter of the main kidney as a split ureter (ureter fisus).
Diagnostics kidney doublings
Excretory urography helps diagnose kidney doubling. However, the most difficult task is to determine complete or incomplete doubling. The use of magnetic resonance urography and MSCT significantly simplifies this task, but does not solve it completely. The presence of ureterocele is a factor that complicates the diagnosis of complete or incomplete kidney doubling. Cystoscopy in the vast majority of cases helps to establish the diagnosis.
Diagnostics of an additional kidney
With the development of highly informative methods of ultrasound and radiation diagnostics (ultrasound, spiral CT, MRI), the number of observations of the additional kidney increases. The most common disease with an additional third kidney is hydronephrosis.
What do need to examine?
How to examine?
What tests are needed?
Who to contact?