Medical expert of the article

New publications
Iridocyclitis
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
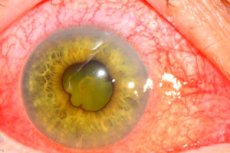
Iridocyclitis is an inflammation of the anterior uveal tract of the eye, which includes the iris and ciliary body. The condition is a form of uveitis, a disease characterized by inflammation of the middle layer of the eye (the uvea), and may also be known as anterior uveitis.
Epidemiology
The epidemiology of iridocyclitis involves the study of the incidence, distribution, and risk factors of this inflammatory eye disease. Specific data may vary by geographic region, ethnicity, and age group.
Prevalence and frequency
- Iridocyclitis is the most common form of uveitis, accounting for approximately 50-60% of uveitis cases in developed countries.
- This condition can occur at any age, but it is most common in young and middle-aged people.
Geographical and ethnic features
- The prevalence and types of uveitis, including iridocyclitis, may vary in different parts of the world. For example, infectious causes of uveitis are more common in developing countries.
- Some types of uveitis, such as those associated with HLA-B27, are more common in Caucasians.
Gender and age
- Iridocyclitis can occur in either sex, although some studies suggest a slight predominance in women or men depending on the subtype of the disease.
- The age of patients at the first detection of iridocyclitis often ranges between 20 and 50 years, but the disease can develop in children and the elderly.
Causes iridocyclitis
According to the etiopathogenetic characteristics, they are divided into infectious, infectious-allergic, allergic non-infectious, autoimmune and those developing in other pathological conditions of the body, including metabolic disorders.
Infectious-allergic iridocyclitis occurs against the background of chronic sensitization of the body to internal bacterial infection or bacterial toxins. Infectious-allergic iridocyclitis most often develops in patients with metabolic disorders in obesity, diabetes, renal and hepatic insufficiency, and vegetative-vascular dystonia.
Allergic non-infectious iridocyclitis can occur with drug and food allergies after blood transfusions, administration of serums and vaccines.
Autoimmune inflammation develops against the background of systemic diseases of the body: rheumatism, rheumatoid arthritis, childhood chronic polyarthritis (Still's disease), etc.
Iridocyclitis can manifest itself as symptoms of complex syndromic pathology: ophthalmostomatogenital - Behcet's disease, ophthalmourethrosynovial - Reiter's disease, neurodermatouveitis - Vogt-Koyanagi-Harada disease, etc.
Risk factors
Risk factors for iridocyclitis may include both exogenous (external) and endogenous (internal) factors. The main ones are listed below:
Endogenous factors:
- Genetic predisposition: Certain genetic markers, such as HLA-B27, are associated with uveitis, including iridocyclitis.
- Autoimmune diseases: Systemic inflammatory diseases such as rheumatoid arthritis, ankylosing spondylitis, systemic lupus erythematosus, and sarcoidosis increase the risk of developing iridocyclitis.
- Immunocompromised states: Patients with immunocompromised states or those taking immunosuppressive therapy may be more susceptible to developing iridocyclitis.
Exogenous factors:
- Infections: Bacterial, viral, fungal, and parasitic infections can lead to the development of iridocyclitis.
- Eye injuries: Injuries or surgeries to the eye can damage the uveal tract and cause inflammation.
- Toxic effects: Certain chemicals or medications can cause inflammation inside the eye.
Systemic diseases:
Medical conditions including Behcet's disease, psoriasis, ulcerative colitis, and Crohn's disease may also increase the risk of developing iridocyclitis.
Other factors:
- Age: Iridocyclitis can occur at any age, but some forms, such as those associated with rheumatic diseases, are more common in young and middle age.
- Gender factor: Some studies have shown that men with certain genotypes may be more prone to developing iridocyclitis.
- Racial and ethnic factors: Certain forms of uveitis are more common in certain racial and ethnic groups.
Risk management includes a thorough medical history, search for associated systemic diseases, regular monitoring of health status, and prompt initiation of treatment for any associated systemic diseases detected.
Pathogenesis
The inflammatory process in the anterior section of the vascular tract can begin with the iris (iritis) or with the ciliary body (cyclitis). Due to the common blood supply and innervation of these sections, the disease moves from the iris to the ciliary body and vice versa - iridocyclitis develops.
The above-mentioned structural features of the iris and ciliary body explain the high frequency of inflammatory diseases of the anterior segment of the eye. They can be of different nature: bacterial, viral, fungal, parasitic.
The dense network of wide vessels of the uveal tract with slow blood flow is practically a septic tank for microorganisms, toxins and immune complexes. Any infection that develops in the body can cause iridocyclitis. The most severe course is observed in inflammatory processes of viral and fungal nature. Often the cause of inflammation is a focal infection in the teeth, tonsils, paranasal sinuses, gall bladder, etc.
Among exogenous influences, the causes of the development of iridocyclitis can be contusions, burns, injuries, which are often accompanied by the introduction of infection.
According to the clinical picture of inflammation, serous, exudative, fibrinous, purulent and hemorrhagic iridocyclitis are distinguished; according to the nature of the course - acute and chronic; according to the morphological picture - focal (granulomatous) and diffuse (non-granulomatous) forms of inflammation. Focal inflammation is characteristic of hematogenous metastatic introduction of infection.
The morphological substrate of the main inflammation focus in granulomatous iridocyclitis is represented by a large number of leukocytes, there are also mononuclear phagocytes, epithelioid, giant cells and a necrosis zone. Pathogenic flora can be isolated from such a focus.
Infectious-allergic and toxic-allergic iridocyclitis occur in the form of diffuse inflammation. In this case, the primary lesion of the eye may be located outside the vascular tract and be located in the retina or optic nerve, from where the process spreads to the anterior section of the vascular tract. In cases where toxic-allergic lesion of the vascular tract is primary, it never has the character of a real inflammatory granuloma, but occurs suddenly, develops quickly as hyperergic inflammation.
The main manifestations are microcirculation disorders with the formation of fibrinoid swelling of the vascular wall. In the focus of the hyperergic reaction, edema, fibrinous exudation of the iris and ciliary body, plasmatic lymphoid or polynuclear infiltration are observed.
 [ 9 ], [ 10 ], [ 11 ], [ 12 ], [ 13 ], [ 14 ], [ 15 ], [ 16 ]
[ 9 ], [ 10 ], [ 11 ], [ 12 ], [ 13 ], [ 14 ], [ 15 ], [ 16 ]
Symptoms iridocyclitis
Iridocyclitis, also known as anterior uveitis, is an inflammatory condition of the eye that affects the iris and ciliary body. Symptoms can vary depending on the severity and duration of the inflammation, but typically include the following:
- Eye pain: One of the first symptoms may be pain in or around the eye, which may worsen when looking at light.
- Redness of the eye: Occurs due to dilation of blood vessels, especially in the area close to the iris.
- Photophobia: Increased sensitivity to light is a common symptom due to irritation and inflammation.
- Decreased vision: Vision may become blurry or blurry intermittently.
- Floaters or "spots" in the eyes: Inflammation can cause small particles to appear in the vitreous, creating the effect of floating spots.
- Swelling of the eye (chemosis): Swelling may be visible around the iris of the eye, changing its color or texture.
- Constricted pupil: The pupil may be smaller than normal and react more slowly to light.
- Eyelid swelling: Mild swelling of the eyelids may be noted.
- Tearing: Due to irritation and pain, the eye may produce excessive tears.
- Eye discomfort: Feeling of a foreign body in the eye, itching or burning.
- A collection of inflammatory cells in the anterior chamber of the eye, which can be seen when examined with special equipment.
These symptoms may develop gradually or occur suddenly and may range from mild discomfort to severe pain, significantly affecting the patient's quality of life. If such symptoms occur, you should immediately contact an ophthalmologist for diagnosis and treatment.
Stages
Depending on the duration and severity of the process, the stages of iridocyclitis are classified as follows:
Acute stage:
- Inflammation occurs rapidly and is accompanied by intense symptoms such as severe pain, redness, photophobia and decreased vision.
- "Precursor cells" and protein deposits (dashes) may form in the anterior chamber of the eye.
Subacute stage:
- Symptoms are less severe and pain and redness may decrease.
- Swelling and inflammation persist, but are less intense.
Chronic stage:
- Chronic iridocyclitis can develop slowly, sometimes without noticeable symptoms of pain and redness.
- Gradual deterioration of vision and development of complications due to constant inflammation are possible.
Remission:
- The period when symptoms of iridocyclitis are absent.
- Remission can be complete, when the inflammation disappears completely, or partial, when symptoms are reduced to a minimum.
Forms
Forms of iridocyclitis can also be classified by the nature of the inflammation:
Granulomatous iridocyclitis:
- Characterized by the formation of granules and usually a more severe course.
- May be associated with systemic diseases such as sarcoidosis or tuberculosis.
Nongranulomatous iridocyclitis:
- The inflammatory process is less pronounced, with fewer inflammatory cells and no granulomas.
- It usually has a milder course and may be associated with autoimmune diseases such as rheumatoid arthritis or juvenile idiopathic arthritis.
It is important to consider that iridocyclitis can also be classified by etiology (infectious, non-infectious), by prevalence (anterior, intermediate, posterior, diffuse) and by other characteristics, which influences the choice of treatment and prognosis.
Other forms of iridocyclitis
The main forms of iridocyclitis are:
- Anterior uveitis (iritis): This is the most common form of uveitis, in which inflammation is limited to the anterior portion of the uveal tract, primarily the iris.
- Intermediate uveitis (cyclitis): Inflammation of the ciliary body.
- Panuveitis: Inflammation affects all parts of the uveal tract, including the iris, ciliary body, and the choroid itself.
- Posterior uveitis: Inflammation of the posterior portion of the uveal tract, primarily the choroid, is less common and considered a more serious condition due to the risk of complications including retinal detachment.
Iridocyclitis is also classified
Acute iridocyclitis is an inflammation of the anterior uveal tract of the eye, including the iris (iridocyclitis) and ciliary body (cyclitis). The condition can occur suddenly and is characterized by a number of symptoms, including eye pain, redness, decreased vision, sensitivity to light (photophobia), and sometimes a decrease in pupil size (miosis).
Subacute iridocyclitis is a moderate inflammation of the iris and ciliary body of the eye. It is not as acute or rapidly progressive as acute iridocyclitis, but it still causes significant discomfort and requires medical intervention. Symptoms may develop more slowly and may be less intense, but eye soreness, redness, lacrimation, photophobia, and temporary decreased vision may still be present.
Chronic iridocyclitis is a long-term, periodically recurring inflammation of the anterior segment of the eye, which includes the iris and ciliary body. The condition can last for months or even years, sometimes with periods of exacerbation and remission. Unlike the acute form, chronic iridocyclitis may have less pronounced symptoms and is often diagnosed only after late complications or changes in the eye are discovered.
Serous iridocyclitis is a form of inflammation of the anterior segment of the eye, in which the vascular membrane of the eye is mainly affected without significant expression of exudation of cellular elements. In this case, the exudate that is formed is predominantly protein in nature (serum), hence the name "serous".
This form of iridocyclitis may be associated with systemic diseases such as sarcoidosis, Behcet's disease, or systemic lupus erythematosus, or occur as an isolated ocular disease.
Exudative iridocyclitis is a type of uveitis in which inflammation of the anterior segment of the eye is accompanied by the release of exudate containing both protein components and cellular elements. This form of iridocyclitis is characterized by a more pronounced infiltration of inflammatory cells into the anterior chamber of the eye and the vitreous body.
Exudative iridocyclitis may be the result of an infectious process, an immunological reaction, or associated with systemic diseases such as rheumatoid arthritis, Crohn's disease, or may be idiopathic (without a known cause).
Suppurative iridocyclitis is a serious inflammatory eye disease characterized by the penetration of pus into the anterior chamber of the eye, which usually indicates a severe infectious process. This condition can be caused by various pathogens, including bacteria, fungi, or parasites.
Fibrinous iridocyclitis is a form of inflammatory disease of the anterior segment of the eye, in which fibrin is formed - a protein that is involved in the process of blood clotting and the response to inflammation.
In fibrinous iridocyclitis, strands or networks of fibrin form in the anterior chamber of the eye and can be visualized with a slit lamp.
Iridocyclitis associated with ankylosing spondylitis (Bechterew's disease) is one of the most common extra-articular manifestations of this systemic disease. Ankylosing spondylitis is a chronic inflammatory rheumatological disease primarily affecting the spine and sacroiliac joints.
Features of iridocyclitis in Bechterew's disease: Iridocyclitis occurs in approximately 25-30% of patients with Bechterew's disease.
- The inflammation is usually one-sided and may alternate between the eyes.
- The course is often characterized by sudden exacerbations and declines.
- The diagnosis of ankylosing spondylitis is confirmed based on clinical symptoms, laboratory data (eg, HLA-B27), and imaging findings (MRI, X-ray).
It is important for patients with ankylosing spondylitis to have regular eye examinations to ensure early detection and treatment of iridocyclitis, and to closely follow the doctor's recommendations for general treatment of the disease to reduce the risk of complications.
Viral iridocyclitis is inflammation of the iris (iritis) and ciliary body (cyclitis) that is caused by a viral infection. It is most commonly associated with viruses such as herpes simplex virus (HSV), varicella-zoster virus (VZV), which causes chickenpox and shingles, and cytomegalovirus (CMV).
Herpetic iridocyclitis is an inflammation of the anterior segment of the eye caused by infection with herpes viruses, most commonly herpes simplex virus (HSV) or varicella-zoster virus (VZV). These viruses may cause a primary infection or become active after a period of latency, causing recurrent inflammation.
Bacterial iridocyclitis is inflammation of the iris (iritis) and ciliary body (cyclitis) caused by a bacterial infection. It is a rarer form of iridocyclitis than viral iridocyclitis and is usually caused by bacteria entering the eye from the outside environment or spreading through the bloodstream from other sites of infection in the body.
Tuberculous iridocyclitis is a manifestation of extrapulmonary tuberculosis in which Mycobacterium tuberculosis (the bacterium that causes tuberculosis) causes inflammation in the structures of the eye, including the iris and ciliary body. This type of iridocyclitis can develop in patients with active tuberculosis as well as those with latent infection.
Syphilitic iridocyclitis is an inflammatory disease of the eye caused by the bacterium Treponema pallidum, which is the causative agent of syphilis. Iridocyclitis can develop at any stage of syphilis, but is most often associated with the secondary and tertiary periods of the disease.
Rheumatoid iridocyclitis, also called rheumatoid arthritis (RA)-associated uveitis, is one of the serious complications of this connective tissue disease. In rheumatoid arthritis, iridocyclitis may occur as a result of autoimmune inflammation.
Allergic iridocyclitis is an inflammation of the iris and ciliary body of the eye caused by an allergic reaction. It is a rare condition, as most allergic reactions in the eye manifest as conjunctivitis. However, in the case of allergic iridocyclitis, the inflammation may be more severe and require specific treatment.
Autoimmune iridocyclitis is a form of uveitis that involves inflammation of the iris and ciliary body, and is most often associated with systemic autoimmune diseases. In these cases, the immune system mistakenly attacks the tissues of the eye, leading to inflammation.
Posttraumatic iridocyclitis is an inflammation of the iris and ciliary body of the eye that occurs after an eye injury. The injury may be penetrating or non-penetrating and includes blows to the eye, penetrating wounds, burns, or surgery.
Fuchs' heterochromic iridocyclitis is a chronic, often unilateral inflammatory eye disease characterized by discoloration of the iris (heterochromia), precipitates on the corneal endothelium, and often the development of cataracts and secondary glaucoma.
Recurrent iridocyclitis refers to recurring inflammation of the iris and ciliary body of the eye. These episodes of inflammation can be caused by a variety of reasons, including autoimmune diseases, infections, or injuries, and may recur at varying intervals.
- Periods of acute redness, pain, photophobia and decreased vision, alternating with periods of remission.
- During a relapse, precipitates and cellular elements may appear in the anterior chamber of the eye.
Determining the form of iridocyclitis is important for diagnosis, treatment and prognosis.
Complications and consequences
Outcome of iridocyclitis:
- favorable with complete recovery (normal properties of the cornea and visual functions are restored);
- mild corneal discoloration, pigment precipitates on the cornea and clouding of the lens, partial atrophy of the pupillary border, deformation of the pupil, destruction of the vitreous body;
- complicated cataract; secondary uveitis
- atrophy of the eyeball;
- retinal detachment;
- corneal opacity (if keratitis occurs).
The last three types of complications lead to a sharp decrease in vision, even to blindness.
Diagnostics iridocyclitis
Diagnosis of iridocyclitis involves clinical evaluation and may require a number of diagnostic procedures:
- History: Important to identify previous trauma, infections, associated systemic diseases, or previous history of uveitis.
- Ophthalmological examination:
- Slit lamp: To examine the anterior segment of the eye in detail, detecting inflammatory cells in the anterior chamber (cells and flav) and other signs of inflammation such as posterior synechia (adhesion of the iris to the lens).
- Tonometry: Measurement of intraocular pressure, which may be low or high in uveitis.
- Fundus examination: To evaluate the posterior segment of the eye, including the retina and optic nerve.
- Laboratory tests: Although most cases of iridocyclitis are idiopathic, it is important to rule out systemic infectious and autoimmune diseases. May include:
- Complete Blood Count (CBC)
- Analysis for rheumatoid factor, ANA and HLA-B27 antibodies
- Tests for infectious diseases (eg tuberculosis, syphilis, HIV)
- Urinalysis to evaluate systemic vasculitis.
- Images:
- Optical coherence tomography (OCT): Can be used to study the structure of the retina and detect macular edema.
- Fluorescein angiography (FA): Helps to assess the condition of the vessels of the retina and choroid.
- Ultrasound of the eye: If retinal detachment is suspected or to evaluate the posterior segment if media turbidity is observed.
- Immunological tests: To detect autoimmune diseases.
- Consultations with other specialists: For example, with a rheumatologist, if there is a suspicion of a systemic disease.
After collecting all the necessary information, the doctor will make a diagnosis of iridocyclitis and prescribe appropriate treatment, which may include topical or systemic steroids, immunosuppressive therapy, and drugs to control intraocular pressure if necessary.
What do need to examine?
How to examine?
Differential diagnosis
Differential diagnosis of iridocyclitis involves consideration of other diseases and conditions that can mimic the symptoms of inflammation in the anterior segment of the eye. Here are some of them:
Conjunctivitis:
- Characterized by redness and irritation of the conjunctiva.
- Usually accompanied by itching and discharge, but without the pain and photophobia that are characteristic of iridocyclitis.
Glaucoma:
- An acute attack of angle closure may mimic symptoms of iridocyclitis, including eye redness, pain, and decreased vision.
- Characterized by sharply increased intraocular pressure.
Keratitis:
- Inflammation of the cornea may be accompanied by redness, tearing and pain.
- Often caused by infection or injury.
Endophthalmitis:
- A serious infectious lesion of the internal structures of the eye.
- It is accompanied by severe pain, marked deterioration of vision and often visible purulent discharge inside the eye.
Episcleritis and scleritis:
- Inflammation of the episclera or sclera, respectively, leads to redness and pain.
- It differs from iridocyclitis by the location of the inflammation and usually more superficial redness.
Dry eye syndrome:
- May cause redness, burning and a foreign body sensation in the eye.
- Not accompanied by cellular infiltration of the anterior chamber.
Eye injury:
- Injury to the eye can result in an inflammatory reaction simulating iridocyclitis.
- It is important to take a thorough history to identify possible trauma.
Leber's amaurosis:
- A rare genetic disorder that causes vision loss.
- Usually not accompanied by inflammation, but important to rule out in cases of sudden vision loss in young people.
Systemic diseases:
- Some systemic diseases, such as rheumatoid arthritis, sarcoidosis, systemic lupus erythematosus, can manifest as uveitis.
- A detailed medical examination is required to exclude them.
For accurate diagnosis, it is important to conduct a complete ophthalmological and general clinical examination, sometimes with consultation with highly specialized specialists. In some cases, laboratory and instrumental studies may be required to exclude systemic diseases.
Who to contact?
Treatment iridocyclitis
Treatment for iridocyclitis (inflammation of the iris and ciliary body) depends on the cause, severity, and symptoms. Below are general treatments for iridocyclitis:
Anti-inflammatory drugs:
- Corticosteroids (steroidal anti-inflammatory drugs) are the standard of treatment. They can be given as eye drops, periocular injections, or systemic medications (oral or injection).
- Nonsteroidal anti-inflammatory drugs (NSAIDs) are also used to reduce inflammation and pain.
Drugs for pupil dilation (mydriatics and cycloplegics):
- Drugs such as atropine or scipolamine are used to dilate the pupil. This helps relieve pain, prevent adhesions (posterior synechiae) and stabilize blood flow to the iris.
Antibiotics or antiviral drugs:
- If iridocyclitis is caused by an infection, appropriate antibiotics or antiviral agents may be prescribed.
Immunosuppressants and immunomodulators:
- For autoimmune causes of irritable bowel syndrome, such as rheumatoid arthritis or ankylosing spondylitis, medications to suppress the immune system may be prescribed.
Treatment of the underlying disease:
- If iridocyclitis is secondary to another systemic disease, it is important to treat that underlying problem.
Laser therapy or surgery:
- In cases of complications such as synechiae (adhesions) or increased intraocular pressure, laser therapy or surgery may be required.
It is important to remember that self-medication for iridocyclitis can be dangerous, and any treatment should be carried out under the strict supervision of an ophthalmologist. Patients with iridocyclitis should regularly visit an ophthalmologist to monitor the condition and adjust treatment depending on the response to therapy.
Prevention
Prevention of iridocyclitis includes several aspects, as this disease can be caused by various reasons and conditions. Some preventive measures:
Timely treatment of infectious diseases:
- Effective treatment of infections that can lead to the development of iridocyclitis, such as herpes, syphilis, tuberculosis and others.
Control of systemic inflammatory diseases:
- Management and monitoring of chronic inflammatory diseases such as rheumatoid arthritis, ankylosing spondylitis, sarcoidosis and others that can cause uveitis.
Eye protection:
- Use safety glasses when working in hazardous conditions or playing sports to prevent eye injuries.
Regular medical examination:
- Regular visits to an ophthalmologist for early detection and treatment of any eye diseases.
Healthy lifestyle:
- Maintaining a healthy lifestyle, including a balanced diet, moderate exercise, and avoiding smoking, may help reduce the risk of chronic inflammatory conditions.
Stress Management:
- Stress management techniques may help in some cases, as stress can contribute to inflammation in the body.
Avoiding UV radiation:
- Wearing sunglasses to protect your eyes from ultraviolet rays, which can contribute to the development of uveitis.
Preventive treatment for high risk:
- In some cases, when a patient is at high risk, preventive medications may be prescribed.
Vaccination:
- Appropriate vaccination can prevent some infections that can lead to iridocyclitis.
Personal hygiene:
- Maintaining good hand hygiene and avoiding eye rubbing can help prevent the transmission of infections that can cause inflammation.
It is important to understand that even if all preventive measures are taken, iridocyclitis may develop, especially if it is part of a systemic inflammatory process. In this case, early detection and treatment are crucial to prevent complications and preserve vision.
Forecast
The prognosis for iridocyclitis, or anterior uveitis, depends on several factors, including the cause of the disease, the timeliness of treatment, the presence of complications, and the patient's overall health. In many cases, iridocyclitis can be successfully controlled with medication, which helps avoid serious vision loss or the development of chronic inflammation.
Factors Affecting Prognosis
- Etiology: Iridocyclitis caused by infections may have a good prognosis with adequate antimicrobial therapy. Uveitis associated with systemic inflammatory diseases may have a more complex course and require more aggressive long-term treatment.
- Timeliness and adequacy of treatment: Rapid initiation of treatment increases the chances of a favorable outcome and reduces the risk of complications. In chronic cases and late treatment, the prognosis worsens.
- Presence of complications: The development of complications such as glaucoma, cataracts or macular edema may worsen the visual prognosis.
- General health: Co-morbidities such as diabetes or immunocompromised states may complicate the treatment of uveitis and worsen the outcome.
The forecast may be as follows
- Favourable: Mild cases of acute iridocyclitis, especially if treatment is initiated promptly, often have a good prognosis with complete restoration of vision.
- Caution: Moderate cases may require long-term treatment, but may also result in full recovery.
- Unfavorable: Severe cases, especially if complicated or chronic, can lead to irreversible vision loss or vision impairment.
Measures to improve prognosis
- Regular monitoring: Regular monitoring by an ophthalmologist will help to identify and adjust treatment in time if necessary.
- Following your doctor's instructions: It is important to follow all of your doctor's instructions carefully and take all of the medications prescribed.
- Lifestyle changes: A healthy lifestyle, including eating right and not smoking, can help reduce inflammation in the body.
- Stress Management: Stress can make inflammatory conditions worse, so it is important to learn effective stress management techniques.
In general, chronic iridocyclitis requires long-term and sometimes lifelong monitoring and treatment.
References
"Uveitis: Fundamentals and Clinical Practice"
- Authors: Robert B. Nussenblatt and Scott M. Whitcup
- Year: Fourth edition 2010
"Clinical Ophthalmology: A Systematic Approach"
- Author: Jack J. Kanski
"The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology"
- Authors: Peter K. Kaiser, Neil J. Friedman
"Ophthalmology"
- Author: Myron Yanoff, Jay S. Duker
Vaughan & Asbury's General Ophthalmology
- Authors: Paul Riordan-Eva, Emmett T. Cunningham