Medical expert of the article

New publications
Examination of cranial nerves. IX and X pairs: Lingual and vagus nerves
Last reviewed: 07.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

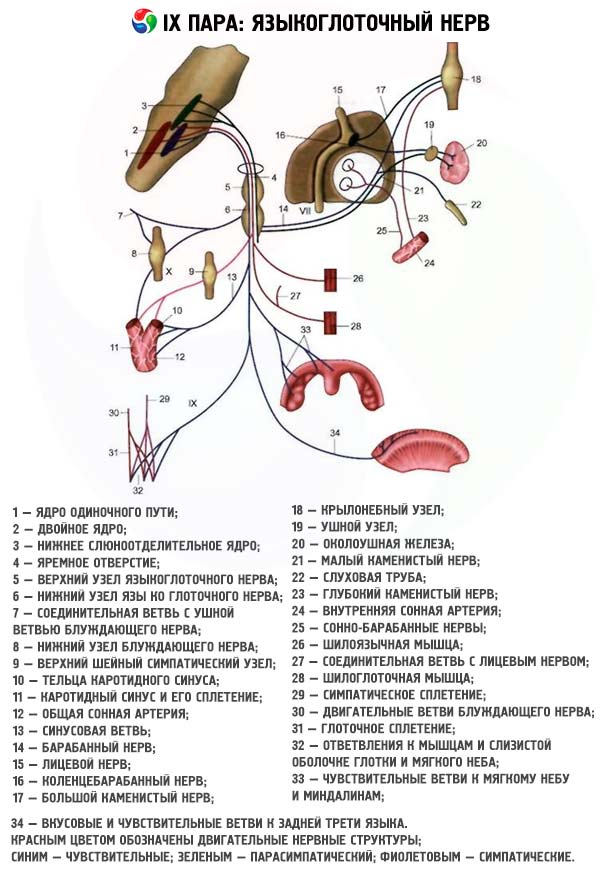
The motor branch of the glossopharyngeal nerve innervates the stylopharyngeus muscle (m. stylopharyngeus).
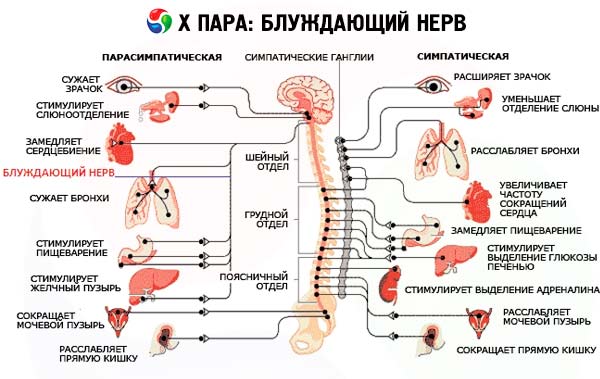
The autonomic parasympathetic secretory branches go to the otic ganglion, which in turn sends fibers to the parotid salivary gland. The sensory fibers of the glossopharyngeal nerve supply the posterior third of the tongue, the soft palate, the pharynx, the skin of the external ear, the mucous membrane of the middle ear (including the inner surface of the tympanic membrane) and the eustachian tube; visceral sensory afferents carry impulses from the carotid sinus; gustatory fibers conduct the sense of taste from the posterior third of the tongue. The vagus nerve innervates the striated muscles of the pharynx (except for the stylopharyngeus muscle), the soft palate (except for the muscle that tenses the soft palate, supplied by the trigeminal nerve ), the tongue (m. palatoglossus), the larynx, the vocal cords and the epiglottis. The vegetative branches go to the smooth muscles and glands of the pharynx, larynx, internal organs of the thoracic and abdominal cavities. Visceral sensory afferents conduct impulses from the larynx, trachea, esophagus, internal organs of the thoracic and abdominal cavities, from the baroreceptors of the aortic arch and chemoreceptors of the aorta. The sensory fibers of the vagus nerve innervate the skin of the outer surface of the auricle and external auditory canal, part of the outer surface of the tympanic membrane, pharynx, larynx, and the dura mater of the posterior cranial fossa.
The glossopharyngeal and vagus nerves share several nuclei in the medulla oblongata and pass close to each other; their functions are difficult to separate, so they are studied simultaneously.
When collecting anamnesis, they find out whether the patient has problems with swallowing or speech (voice).
Voice
Attention is paid to the clarity of speech, timbre and sonority of the voice. If the vocal cords are dysfunctional, the voice becomes hoarse and weak (even to the point of aphonia). Due to dysfunction of the soft palate, which does not sufficiently cover the entrance to the nasopharynx during phonation, a nasal tone of the voice (nasolalia) occurs. Dysfunction of the larynx muscles (damage to the vagus nerve) affects the pronunciation of high sounds (ee-ee-ee), which requires convergence of the vocal cords. In order to exclude weakness of the facial muscles (VII pair) and the muscles of the tongue (XII pair) as a possible cause of speech impairment, the patient is asked to pronounce labial (p-p-p, mi-mi-mi) and anterior lingual (la-la-la) sounds or syllables that include them. Nasal voice is revealed when pronouncing syllables that contain guttural sounds (ga-ga-ga, kai-kai-kai). The patient is also asked to cough forcefully. A patient with acute unilateral paralysis of the vocal cords is unable to pronounce the sound "ee-ee-ee" or cough forcefully.
Soft palate
The soft palate is examined when the patient pronounces the sounds "a-a-a" and "e-e-e". They evaluate how fully, strongly and symmetrically the soft palate rises during phonation; whether the uvula of the soft palate deviates to the side. In case of unilateral paresis of the muscles of the soft palate, the soft palate lags behind on the affected side during phonation and is pulled by healthy muscles to the side opposite to the paresis; the uvula deviates to the healthy side.
Palatal and pharyngeal reflexes
A wooden spatula or a strip (tube) of paper is carefully touched to the mucous membrane of the soft palate alternately on both sides. The normal response is to pull the soft palate upward. Then the back wall of the pharynx is touched, also on the right and left. The touch causes swallowing, sometimes gagging movements. The reflex response is expressed to varying degrees (in elderly people it may be absent), but normally it is always symmetrical. The absence or reduction of reflexes on one side indicates peripheral damage to the IX and X pairs of cranial nerves.