Medical expert of the article

New publications
Human arterial pulse
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

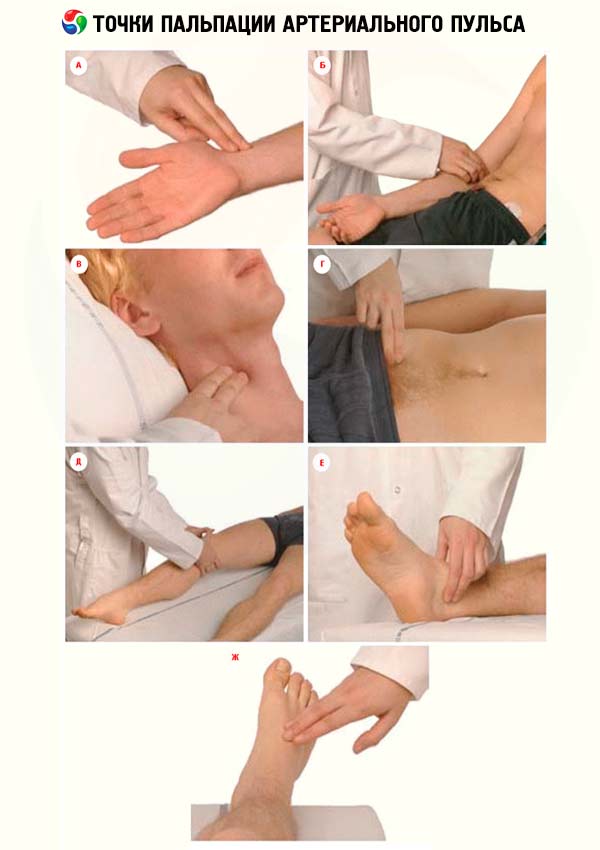
The examination of peripheral arteries usually begins with an inspection, during which visible pulsation may be detected, for example, in the carotid arteries in the neck. However, the most important is the palpation of the peripheral arterial pulse. The pulse is determined on the carotid, brachial, radial, femoral, popliteal and foot arteries. The assessment of the peripheral arterial pulse and its characteristics on the radial arteries are generally accepted.
 [
[ Measuring arterial pulse
Pulse (pulsus) is a rhythmic oscillation of the artery wall caused by changes in its blood filling as a result of heart contractions. The main clinical method for assessing the condition of the arteries and their pulsation is palpation. The pulse is examined in the area of the radial artery in its distal part. This place is most convenient for assessing the pulse, because the artery lies here immediately under the skin on a dense bone, although anomalies in its location are possible, but they are comparatively rare. When palpating the pulse, the arm muscles should not be tense. First, the pulsation of the radial arteries is examined simultaneously on both arms; if there is no asymmetry, the pulse is determined on one arm. With the fingers of the right hand, the doctor grasps the forearm of the person being examined near the wrist joint so that the thumb is located on the back of the forearm, and two or three others are on its front surface in the area of the radial artery. Using two or three fingers, carefully palpate the area of the artery, squeezing it with varying force until the peripheral blood flow stops completely. Usually, the radial artery is palpated as an elastic cord. In case of atherosclerotic lesions, the artery walls may be thickened, it becomes tortuous. The pulse is examined to assess the following basic properties: frequency, rhythm, tension, filling, size, and shape of the pulse wave.
Pulse is normal
Normally, the pulse oscillations are symmetrical on both corresponding arteries. Different pulse characteristics on the right and left radial arteries are the basis for different pulses (p. difference). This difference concerns the filling and tension of the pulse, as well as the time of its appearance. If the pulse on one side is less filling and tense, one should think about narrowing of the artery along the path of the pulse wave. A significant weakening of the pulse on one side may be associated with a dissecting aortic aneurysm, peripheral embolism or vasculitis, including aortic damage (most often aortitis ) at different levels. In the latter case, gradual damage to the mouth of one of the large arteries leads to the disappearance of pulsation on the radial artery ( Takayasu syndrome ).
During the period of the pulse wave decrease, a small new rise can be felt. Such a double pulse is called dicrotic. The dicrotic rise is also inherent in the normal pulse, which is recorded on the sphygmogram. When palpating the pulse, dicrotia is rarely detected, the dicrotic wave is explained by the fact that at the beginning of diastole, part of the aortic blood makes a small movement backward and seems to hit the closed valves. This impact creates a new peripheral wave, following the main one.
With a correct rhythm, but significant fluctuations in the magnitude of cardiac output, the so-called alternating pulse (p. alternans) is noted, in which the filling of individual pulse waves fluctuates.
Thus, various changes in the properties of the pulse are noted. Among them, the most important, in addition to frequency and rhythm, are the filling and tension of the pulse. In typical cases, a healthy person has a rhythmic pulse of moderate (or satisfactory) filling and not tense.
Evaluation of the properties and main characteristics of the pulse
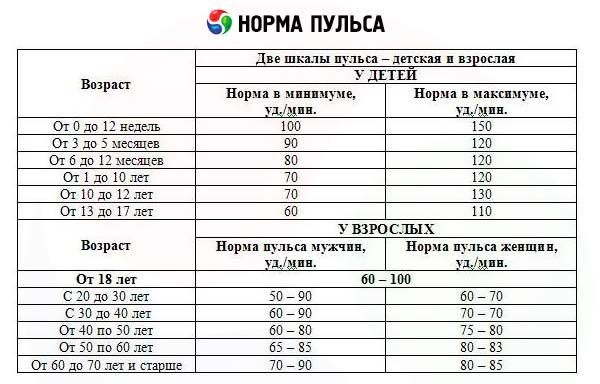
The pulse rate is determined by counting the pulse beats for 15-30 seconds and multiplying the resulting figure by 4-2. If the rhythm is abnormal, the pulse should be counted for the entire minute. The normal pulse rate for men is 60-70 beats per minute, for women up to 80 beats per minute, for children and the elderly the pulse is faster. When assessing the pulse rate, it should be taken into account that its frequency increases with mental excitement, in some people - when communicating with a doctor, with physical exertion, after eating. With a deep breath, the pulse quickens, and with an exhale it becomes slower. Increased pulse rate is observed in many pathological conditions.
The pulse rhythm can be regular (p. regularis) and irregular (p. irregularis). Usually, pulse waves follow each other at intervals of close duration. In this case, pulse waves are normally the same or almost the same - this is a uniform pulse (p. aequalis). In pathological conditions, pulse waves can have different values - an unequal pulse (p. inaequalis), which depends on the difference in the value of diastolic filling and systolic ejection of the left ventricle.
The systolic output during individual contractions of the heart may be so different that the pulse wave during contractions with a small output may not reach the radial artery, and the corresponding pulse fluctuations are not perceived by palpation. Therefore, if the number of heartbeats is determined simultaneously by auscultation of the heart and by palpation of the pulse on the radial artery, a difference will be revealed, i.e. a pulse deficit, for example, the number of heartbeats during auscultation is 90 per minute, and the pulse on the radial artery is 72 per minute, i.e. the pulse deficit will be 18. Such a pulse with a deficit (p. deficiens) occurs with atrial fibrillation with tachycardia. In this case, large differences are observed in the duration of diastolic pauses and, consequently, in the amount of filling of the left ventricle. This leads to a significant difference in the amount of cardiac output during individual systoles. Heart rhythm disturbances can be best characterized and assessed by electrocardiography.
Pulse tension is characterized by the pressure that must be exerted on the vessel to completely interrupt the pulse wave at the periphery. Pulse tension depends on the arterial pressure inside the artery, which can be roughly estimated by pulse tension. A distinction is made between a tense or hard pulse (p. durus) and a soft or relaxed pulse (p. mollis).
Pulse filling corresponds to fluctuations in the volume of the artery during cardiac contractions. It depends on the magnitude of the systolic ejection, the total amount of blood and its distribution. Pulse filling is assessed by comparing the volume of the artery when it is completely compressed and when blood flow is restored in it. According to filling, a distinction is made between a full pulse (p. plenus), or satisfactory filling, and an empty pulse (pp. vacuus). The most striking example of a decrease in pulse filling is the pulse in shock, when the amount of circulating blood and, at the same time, the systolic ejection decrease.
The pulse size is determined based on the overall assessment of the tension and filling of the pulse, their fluctuations with each pulse beat. The pulse size is greater, the greater the amplitude of the arterial pressure. According to the size, a distinction is made between the large pulse (p. magnus) and the small pulse (p. parvus).
The pulse shape is characterized by the speed of the rise and fall of pressure inside the artery. The rise can occur more quickly, which depends on the speed with which the left ventricle ejects blood into the arterial system. A pulse characterized by a rapid rise in the pulse wave and a rapid fall is called fast (p. celer). Such a pulse is observed in case of aortic valve insufficiency, to a lesser extent with significant nervous excitement. In this case, the pulse is not only fast, but also high (p. celer et altus). The opposite pulse shape - p. tardus et parvus is characterized by a slow rise in the pulse wave and its gradual decrease. Such a pulse occurs with stenosis of the aortic orifice.
Auscultation of arteries
Auscultation of the arteries is performed without significant pressure, since high pressure artificially causes stenotic noise. The following main places for listening are noted: carotid artery - at the inner edge of the sternocleidomastoid muscle at the level of the upper edge of the thyroid cartilage; subclavian - under the clavicle; femoral - under the inguinal ligament; renal - in the umbilical region on the left and right. Under normal conditions, tones are heard over the carotid and subclavian arteries: I tone depends on the passage of the pulse wave, II tone is associated with the slamming of the aortic and pulmonary artery valves. Noises in the arteries are heard during their expansion or narrowing, as well as during the conduction of noises generated in the heart.
Auscultation of the vessels in the cubital fossa is of particular importance when determining blood pressure.