Medical expert of the article

New publications
Follicular lymphoma
Last reviewed: 05.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The diagnosis is follicular lymphoma. Such an incomprehensible and scary disease at first glance belongs to the category of the mildest and relatively safe pathologies associated with malignant neoplasms. At the same time, what is pleasing is that the pathology in question responds well to complex medical therapy, and, therefore, is treatable.
Causes follicular lymphoma
It is worth mentioning right away that there is no reason to rejoice too much. Modern medicine has not yet managed to achieve complete remission. It cannot be expected even when the surgical treatment went well and the tumor was completely removed. Even with such an outcome of treatment, the disease usually returns after three years, in the best case - after five years.
The disease in question received this terminology because in most cases the malignant neoplasm began to form and develop in the covering cells of the epidermis, pathologically changing the hair follicles, or as they are also called, follicles.
To date, no oncologist will undertake to name all the causes of follicular lymphoma, since its nature has not yet been fully studied. We can only say that one of the sources that provoke pathological degeneration of the cell is gene mutations. But what served as a catalyst for these metamorphoses - this question remains open for now.
However, several reasons that doctors have managed to establish can be cited:
- Surgical intervention associated with organ transplantation.
- Endoprosthetics is an operation to replace a joint with implants.
- Long-term use of certain pharmacological agents, such as immunosuppressants.
- A congenital chromosomal abnormality, but this alone is not enough to trigger the development of follicular lymphoma. For this, this pathology must be "accompanied" by some other factors. For example, this may be trisomy and/or monosomy, which also relates to genetic abnormalities.
- Various autoimmune diseases.
- Quite close contact when working with pesticides, which today is almost inevitable in the agricultural sector of human activity.
- The presence of bad habits in a person. This is especially true for nicotine.
- As a result of receiving a dose of ionizing radiation.
- Contact of any kind with toxic chemical compounds, carcinogenic substances.
- The risk of developing the disease in question increases if people live in an ecologically polluted area. This could be a large metropolis with large industrial facilities. Or, for example, people living in dangerous proximity to a chemical plant.
- An acquired or congenital disorder that affects a person's immune status.
Symptoms follicular lymphoma
The most common areas of localization of the disease in question are: armpits, groin area, human head and neck. Oddly enough, this disease occurs mainly in young people who fall into the age category of up to forty years.
The insidiousness of this pathology, as well as other oncological diseases, is that in the early stages of its progression, nothing bothers the patient and the disease can only be diagnosed by chance, during a routine preventive examination, or during studies that were prescribed in connection with the treatment of another disease.
Once the tumor continues to progress, it can be recognized by palpation. Later, symptoms of follicular lymphoma begin to appear:
- The malignant formation may protrude above the surface of the skin.
- The "swelling" has clear outlines.
- The color of the neoplasm may be slightly pinkish or purple-scarlet.
- Substance of increased density.
- Painful sensations appear at the site of the tumor.
- The neoplasm is capable of bleeding.
- The epidermis becomes ulcerated.
- The patient begins to feel weakness throughout the body.
- The difference between inflammation of the lymph nodes (from an infectious lesion) is that they are not only painful, but also not sensitive to antibiotics.
- Increased production of sweat by the corresponding glands.
- Doctors observe a chromosomal translocation t(14:18).
- An increase in body temperature may be observed.
- A person begins to lose weight without any reason.
- Problems with the digestive tract appear.
- Decreased performance.
- Nausea.
- There may be a feeling of fullness in the abdomen, a feeling of pressure in the face or neck, difficulty breathing. This may be due to increased pressure on the digestive organs from the spleen, liver or directly the lymph node (with a certain localization of the tumor) or on other organs of the human body.
- Dizziness, even to the point of fainting.
- Depending on the location, the patient may have problems with swallowing, which is associated with an increase in the volume of the pharyngeal lymphatic ring.
- Fever can appear without any obvious reason.
- Hearing loss.
It is worth noting that the symptoms, depending on the location of the affected lymph node, may combine various manifestations from those listed above.
Sometimes this disease can be detected and diagnosed only when the malignant process begins to affect the bone marrow. The good thing is that asymptomatic lymphoma is quite rare.
Non-Hodgkin's follicular lymphoma
Follicular lymphoma itself, according to medical classification, belongs to the non-Hodgkin's type. As sad as it may sound, modern medicine only in some cases manages to recognize the disease at an early stage of its origin. In 70% of cases, the patient seeks advice from a specialist when obvious manifestations of the disease begin. For example, frequent nausea and the person begins to faint. This is due to the fact that the disorders have already captured the bone marrow.
Often, non-Hodgkin's follicular lymphoma is diagnosed at an early stage of development during a comprehensive medical examination, using modern high-precision diagnostic equipment. It is in this regard that doctors insist that a person should undergo a full preventive examination at least once a year. Such an approach to one's health will significantly reduce the risk of full-scale damage to the human body, and irreversible pathological changes.
Non-Hodgkin's lymphomas are caused by cancerous neoplasms of the B- and T-cell type. The source of such pathology can originate in any lymph node or other organ, and then "infect" the lymph. Subsequently, metastasis occurs in three ways: hematogenous, lymphogenous, hematogenous-lymphogenous.
Such lymphomas have their own qualification, which differs in morphology, clinical symptoms, and also parameters of the disease. Depending on the area of localization, doctors distinguish lymphomas - cancerous neoplasms affecting the lymphoid layers with primary origin, not affecting the bone marrow, and leukemias - cancerous changes, already primarily affecting the bone marrow layers.
All age categories of the population are susceptible to this disease, but still a higher percentage falls on people who have already reached 60 years of age.
To date, the etiology of lymphosarcomas is not completely known. Therefore, when talking about the causes that can provoke the disease, it is necessary to talk about those aspects that increase the risk of its origin and development. These include:
- Viral pathologies. For example, AIDS, Epstein-Barr virus, hepatitis, especially hepatitis C.
- Infectious lesion of Helicobacter pylori, which, as some scientists believe, is the “culprit” of ulcerative lesions of the mucous membrane of the digestive tract.
- Congenital or acquired immunodeficiency can increase the likelihood of the disease.
- And other reasons already mentioned above.
The non-Hodgkin's type of follicular lymphoma has its own, fairly extensive classification:
Lymphatic sarcomas localized in lymph nodes are called nodal, in case of other localization (salivary glands, tonsils, thyroid gland, epidermis, brain, lungs, etc.) - extranodal. Follicular (nodular) or diffuse is made by the structural component of the neoplasm.
There is also a division according to the speed of the disease:
- Indolent - progression is smooth. Without treatment, such a patient can live from seven to ten years. Treatment gives a fairly favorable prognosis.
- Aggressive and highly aggressive course of the disease. Without medical therapy, such a patient can live from several months to one and a half to two. Treatment gives a fairly favorable prognosis.
Today, oncological medicine counts more than 30 different types of non-Hodgkin's lymphomas. Most of them (about 85%) are B-cell lymphomas (B-lymphocytomas), and the remaining 15% are T-cell lymphomas (T-lymphocytomas). Each of these types has its own subtypes.
B cell follicular lymphoma
This type of disease clearly dominates in the diagnosis of the disease. In children, this type of lymphatic system disorder is almost never encountered.
Doctors classify type B cell lymphoma as:
- Diffuse large B-cell lymphoma is the most common type of the disease. 31% of diagnosed non-Hodgkin's lymphomas have this type. The main parameters of the disease are aggressiveness and high rate of progression. But, despite such negative characteristics, with timely medical intervention, it has high prerequisites for a full recovery.
- In cellular follicular lymphoma - the level of diagnosis of this type is 22 cases out of a hundred recognized non-Hodgkin's lymphomas. The course of pathology is indolent, but there are cases when the course is transformed and acquires an aggressive diffuse form. Oncologists have such a criterion as five-year survival. So this category of the disease shows that 60 - 70 people out of a hundred live this five-year period. From 30 to 50% of patients with such a diagnosis are able to overcome the border of ten years. This type has the features of a secondary follicle. The cell includes centrocytes and centroblasts. This type of pathology, according to the cellular composition, is divided into three cytological types. According to the cellular composition, III cytological types of follicular lymphoma are distinguished.
- B-cell lymphomas affecting marginal cells – the diagnostic percentage is not high. They are not aggressive and have a low growth rate. If detected early in development, they respond well to treatment.
- Mantle cell lymphoma - this pathology accounts for about 6% of cases. The disease is quite specific. Only a fifth of those affected survive the five-year mark.
- Small cell lymphocytic lymphoma and chronic lymphocytic leukemia – about 7% of patients are susceptible to this disease. This type of pathology is similar to non-Hodgkin's lymphoma. It is not particularly aggressive, but has low sensitivity to antitumor treatment.
- B-cell mediastinal lymphoma – frequency of diagnosis is 2%. Mostly diagnosed in women aged 30 to 40 years. Only half of patients can be cured.
- Burkitt's lymphoma - incidence is about two percent. The course of the disease is aggressive, but with intensive therapy it is possible to achieve complete recovery (50% of patients).
- Waldenstrom's macroglobulinemia - only 1% of cases. Leads to an increase in the viscosity of blood fluid, which leads to thrombosis and disruption of the integrity of blood vessels. With such a disease, a person can live both 20 years and less than a year.
- Hairy cell leukemia is quite rare and affects older people. 1
- Central nervous system lymphoma – the source of the lesion is the CNS, after which metastases begin to affect the cells of the bone and brain. Only 30% of patients survive five years.
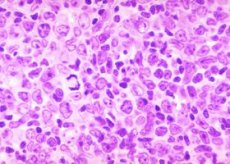
Follicular lymphoma type 2 cytological
One of the main criteria in making a diagnosis and correctly prescribing chemotherapy is the result of histological analysis. Practitioners have confirmed the need to divide the disease in question into cytological types (by morphological principle), depending on the number of large cells determined in the patient's body.
Oncologists differentiate:
- 1 cytological type – the presence of small split cells.
- Follicular lymphoma type 2 cytologically is a collection of large and small cells, morphologically comparable to each other.
- 3 cytological type - large follicle cells.
In case of repeat biopsy, transformation of the first type into the second may be observed, but never into the third.
When diagnosing the type, doctors rely on the results of a cytological study. From here, oncologists establish the type (depending on the number of centroblasts determined in the field of view of the microscope):
- Type 1 – from zero to 5.
- Type 2 – from 6 to 15.
- Type 3 – more than 15. This type is divided into:
- In subtype 3-a, centrocytes are already observed in the field of vision.
- In subtype 3-b, centroblasts form extensive formations without centrocytes.
Cancerous neoplasms of the 2nd cytological type are quite aggressive in progression and require more radical measures of therapy with chemotherapy drugs. But the overall figures of the survival rate of patients of all cytological groups are approximately the same.
Follicular lymphoma 3a cytological type
If a patient is diagnosed with follicular lymphoma of cytological type 3a, the prognosis for this person is very unfavorable. In patients with this pathology, even after they have undergone a full examination and high-quality adequate treatment, recurrent signs of disease recurrence are observed much more often and earlier than in others (with follicular lymphoma of type 1 or 2).
This prognosis can be somewhat improved by introducing doxorubicin therapy into the treatment protocol for such a patient. And the presence of centrocytes in the field of view is a reason for oncologists to prescribe a significantly aggressive therapy to the patient. Type 3a (cytological classification) - this stage is assigned when the spread of the malignant process affects one or two distant lymph nodes.
Distinguished by the most likely occurrence of early relapses, such patients also show a higher percentage of five-year survival.
Diagnostics follicular lymphoma
Even at the slightest suspicion of an oncological problem, the local physician - therapist gives his patient a referral to a specialized oncological dispensary, where he undergoes the necessary examination. Diagnosis of follicular lymphoma is carried out by a more narrowly focused specialist - onco-hematologist.
Indications for examination are a number of criteria that determine the pathological clinical picture: growth in the volume of one or more lymph nodes, the appearance of obvious signs of intoxication (systemic poisoning) of the body in the patient, extranodal changes.
To establish the correct diagnosis, which suggests that the patient has non-Hodgkin's lymphoma, the oncologist must take a sample of the cellular substrate of the neoplasm for examination. For this and to obtain a more complete picture of the person's health, both instrumental methods and laboratory tests are prescribed:
- External examination of the admitted patient.
- Palpation of the lymph nodes, allowing the specialist to assess the volume and density of the neoplasm. But not all neoplasms can be examined in this way. Therefore, a comprehensive examination is indispensable.
- A biopsy of the affected lymph node is performed.
- Laparoscopy is a therapeutic or diagnostic examination of the abdominal organs.
- Thoracoscopy is an endoscopic examination of the pleural cavity.
- A bone marrow puncture is taken - this analysis allows us to exclude or confirm the presence of metastases in a given area of the body.
After the above-mentioned measures have been carried out, the cellular material is sent for further examination. The following research is carried out:
- Immunohistochemistry is a technique that makes it possible to accurately determine the location of a particular cellular or tissue component (antigen) by binding it to labeled antibodies.
- Cytological is a study of the structural features of cells, the cellular composition of organs, tissues, and fluids of the human body for the diagnosis of various diseases using magnifying equipment.
- Cytogenetic – microscopic study of human chromosomes, a set of methods that establish connections between hereditary disorders and the structure of cells (especially the structure of the cell nucleus).
- Other studies.
In the process of prescribing a protocol of therapeutic measures for follicular lymphoma, the doctor also prescribes other additional examinations to determine the location of the tumor and the extent of metastasis:
- X-ray of the suspected affected area.
- Ultrasound examination of the lymph nodes, thyroid and mammary glands, liver, spleen, scrotum and other organs.
- Computed tomography of the peritoneum and chest, which allows to recognize even the smallest structural abnormalities.
- Lymphoscintigraphy is a technique that allows obtaining an image of the lymphatic vessels.
- Scintigraphy of bones and internal organs - diagnostics of metastatic malignant tumor.
- Magnetic resonance imaging (MRI) is a method for visually detecting primary and metastatic foci of cancerous tumors.
- General and biochemical blood analysis.
If the examination reveals finely dispersed cellular disposable structures, the oncologist puts the first or second type of pathology. Large-cell lymphoma already indicates a higher degree of malignancy of the process: stage 3a - the lesion has captured one or two lymph nodes, located at a distance from the site of the main localization; stage 3b - this is already a more large-scale lesion of the human body, and more specifically its lymphatic system.
Quite often, in addition to non-Hodgkin's lymphomas, the oncologist also identifies numerous concomitant pathologies that only worsen the situation.
Who to contact?
Treatment follicular lymphoma
It is in connection with the worsening situation with oncological diseases, the percentage of which is increasing from year to year, that oncologists recommend not to ignore preventive examinations. The earlier the disease is diagnosed, the greater the patient's chances not only to continue a quality life after receiving antitumor treatment, but also to save his life as such. Treatment of follicular lymphoma is prescribed for each patient strictly individually, adjusting it during the course of treatment. There are cases when oncologists, giving certain recommendations to the patient, take a wait-and-see attitude, conducting periodic monitoring of the patient's health and the rate of growth of the neoplasm. Due to the relatively low rate of tumor progression, it may take ten years before it begins to manifest itself, so doctors are in no hurry with radical measures, because the appointment of surgical intervention and chemotherapy drugs also do not pass without a trace for the human body.
That is, if the first or second stage of the pathology with a sluggish form of development is diagnosed, then such a clinical picture can be observed for a decade, periodically alternating with periods of remission and relapses, the doctor only conducts constant monitoring of the patient's condition, ready to take adequate measures at any time.
But we should immediately reassure you that follicular lymphoma, if detected in time and adequately treated, in isolated cases becomes the cause of death for the patient.
But it is also possible to observe the opposite clinical picture, when the tumor begins to progress rapidly, spreading metastases in all directions like tentacles. With such a clinical picture, doctors begin to act immediately, prescribing a course of laser and/or chemotherapy. If the patient's metastasis has affected the bone marrow, the oncologist may decide to prescribe surgery for its transplantation. It is worth mentioning right away that with such a picture of the disease, one should not count on complete remission. Even if the focus of pathology was completely removed, such a patient can live three to five years at most.
At later stages of pathological development, with the appearance of metastases and in organs more distant from the focus, the attending physician - oncologist prescribes laser and/or polychemical therapy to such a patient.
Today, the most popular treatment regimen that gives good therapeutic results is the CHOP method, which is represented by a treatment protocol that includes such drugs as vincrestine, cyclophosphamide, doxorubicin, and prednisolone.
The plant-based alkaloid vincrestine has an antitumor effect on the patient's body. This medicine is administered to the patient orally intravenously. The administration schedule is once a week.
The attending physician prescribes the dosage of the drug strictly individually. The single starting amount of the drug administered to an adult patient is from 0.4 to 1.4 mg, calculated per m2 of the patient's body surface, taken once a week. The starting dosage for small patients is 2 mg calculated per m2 of body surface, taken once a week.
If necessary, the doctor may prescribe intrapleural administration of the drug, i.e. the pharmacological fluid is supplied to the cavity space between the pulmonary membranes. With this method of administration, 1 mg of the drug is supplied to the patient's body, which was diluted with 10 ml of saline solution immediately before the procedure.
Contraindications to taking this medicine include diseases of the central or peripheral nervous system, increased sensitivity of the patient's body to one or more components of the drug. This also includes pregnancy or breastfeeding.
There are also recommendations on how to handle drugs of this pharmacological category.
- This medication should be administered with extreme caution, after making sure that the needle is in a vein. Do not allow non-venous infusion of the pharmacological fluid to avoid necrosis.
- During this medical procedure, the nurse must protect her eyes, and if the medicine gets into them, she must rinse them very quickly and thoroughly in clean running water.
- Before the start of the administration of chemotherapy drugs during treatment, regular monitoring of the peripheral blood condition is necessary.
- Constant monitoring of the biochemical characteristics of liver function is also necessary.
- If the level of neutrophils decreases below the critical level, the procedure for administering the chemotherapy drug is not prescribed, but is postponed until the normal parameters are restored.
- To prevent the development of a hepatotoxic effect, the chemotherapeutic drug is prohibited from being taken in parallel with radiation therapy that affects the kidney and liver area.
Medical personnel who work with these drugs used for chemotherapy are required to comply with all personal protective equipment requirements that apply when in close contact with toxic chemical compounds.
Along with CHOP, the CVP regimen, which includes such medications as vincrestine, cyclophosphamide, and prednisolone, also shows no less effectiveness.
The antineoplastic drug cyclophosphamide, which belongs to the alkylating chemical compounds, can be prescribed by the attending physician, based on the pathological picture, either intramuscularly, intravenously, intraperitoneally, or intrapleurally.
Immediately before the relevant procedure, the drug is diluted with water for injection, with 10 ml of diluent per bottle of the drug with a dose of 0.2 g. The control indicator of the drug's quality is the time it takes for the drug to dissolve in water - it should not exceed four minutes.
The specialist chooses the scheme for administering the drug independently. There are several such schemes.
- A single dose is calculated as 3 mg per kilogram of the patient's weight, about 200 mg, which are administered once a day. The method of administration of the drug: intravenously or intramuscularly.
- A single dose is calculated as 6 mg per kilogram of the patient's weight, about 400 mg, which are administered once twice a day. The method of administration of the drug: intravenously or intramuscularly.
- A single dose is calculated as 15 mg per kilogram of the patient's weight, about 1 g, administered intravenously once every five days.
- A single dose is calculated as 30-40 mg per kilogram of the patient's weight, about 2-3 g, which are administered intravenously once every two to three weeks.
The amount of the drug used for one course of therapy ranges from 6 to 14 g. After completion of the main course, maintenance therapy is usually practiced, which involves intravenous or intramuscular administration of 0.1 - 0.2 g of the drug twice over the course of one week.
This medicine is also used as an immunosuppressant. In this case, the doctor prescribes a quantitative component of the medicine at the rate of 1.0 - 1.5 mg per kilogram of the patient's weight, which corresponds to a daily amount of 50 - 100 mg. If the body has increased tolerance to the drug, the doctor can prescribe the intake of 3 - 4 mg per kilogram of the patient's weight.
For intraperitoneal or intrapleural administration, the dosage of the drug may range from 0.4 to 1.0 g.
Contraindications to the use of the drug in question are hypersensitivity of the patient's body to the component composition of the drug, as well as if the patient's medical history includes severe renal dysfunction, leukopenia (with a leukocyte level in the blood below 3.5 x 109/l), bone marrow hypoplasia, anemia or cachexia, thrombocytopenia (with a platelet level in the blood below 120 x 109/l). This recommendation also applies to the terminal stage of the disease itself, as well as if the woman is pregnant or breastfeeding a newborn.
But the oncological direction of medicine is constantly improving, scientists and pharmacologists are finding new drugs, methods and forms. Today, some oncological clinics practice innovative methods of treatment using the patient's stem cells. Although even against the background of the current level of medicine, such a disease as follicular lymphoma has not yet been fully studied and is not completely curable.
Oncologists consider the following factors to increase the risk of an unfavorable outcome:
- Age group of patients over 60 years old.
- The patient's hemoglobin level is determined by figures below 120 g/l.
- If the patient is diagnosed with stage three or four development.
- Increase in lactate dehydrogenase.
- If the doctor observes that the patient has cancer that affects more than four groups of lymph nodes.
After a course of chemotherapy or laser therapy, the patient is required to undergo maintenance therapy, which is designed to improve his immune status, which has been significantly reduced by the treatment.
After receiving chemotherapy drugs, the patient's immunity is greatly reduced and in order to avoid a secondary infection, which in many cases is the cause of death, such a patient must stay in a sterile environment for a certain period of time.
When secondary leukemia is detected in a patient, which develops against the background of follicular lymphoma, affecting areas of the bone marrow, the oncologist is forced to prescribe a transplant of this substance to the patient from one of his closest relatives. Otherwise, it will be quite difficult to find a full-fledged donor. But if the operation went well, this method shows high therapeutic results.
The most important thing is not to miss the moment and contact a specialist as soon as possible! Sometimes, not only the future quality of a person's life, but also his life depends on time!
Prevention
It is quite difficult to give advice on how to prevent the pathology discussed in this article, but it is still worth discussing some life aspects that will help reduce the risk of any cancerous neoplasms.
Therefore, prevention of follicular lymphoma is indicated by several recommendations:
- Maintaining a healthy lifestyle.
- Giving up bad habits.
- Balanced, rational nutrition, rich in microelements and vitamins.
- Maintaining your immune system at the proper level.
- In case of illness (of any nature), relief therapy should be carried out in a timely manner and until complete recovery.
- Make sure that the body does not become overcooled or overheated for a long time.
- Avoid excessive sunbathing, baths, saunas and solariums.
- When choosing a place for your home, it is advisable to give preference to areas with a clean ecosystem, away from large industrial zones.
- Elimination of hypodynamia. Movement is life.
- Many experts believe that thought is material, so as not to test the negative aspect of this expression on yourself - think only positively, relaxation and pleasant music are welcome.
- A person's daily routine should harmoniously combine workloads and rest periods.
- Regularly, at least once a year, undergo a comprehensive preventive examination in a specialized medical institution.
Forecast
It is problematic to unambiguously assess the consequences of the pathology for a patient diagnosed with non-Hodgkin's lymphoma, since the result of antitumor therapy largely depends on the degree of the disease.
If doctors diagnose a first or second degree pathology, showing a nodular rate of progression, then in nine out of ten patients the prognosis for follicular lymphoma is quite favorable, which is based on a correct diagnosis and an adequate chemotherapy regimen.
In case of establishing non-Hodgkin's lymphoma, which has one of the varieties of the third stage of development, the prognosis of the nodular course of the disease has a less favorable color. The survival rate for this clinical picture is only five people out of ten diagnosed cases.
The good news is that the pathological development of the fourth stage of the disease, when metastases already affect quite distant organs, is very rare. The prognosis for this course of the disease is unfavorable, even with the necessary therapeutic measures. Therapeutic therapy only makes it possible to prolong the patient's life a little (at best, for several years), but a fatal outcome is almost inevitable.
Quite often, the death of such a patient does not occur directly from the cancerous tumor, but the cause of death is a secondary infection, which quite easily enters an organism weakened by the disease.
Monitoring the survival of such patients is quite sad: out of twenty patients diagnosed with stage IV follicular lymphoma, two or three survive.
The contaminated environment, food and fast pace of life do not give health to modern man. Monoclonal tumor consisting of mature B-lymphocytes - follicular lymphoma. The diagnosis of cancer knocks a person and his close relatives off track, putting them in a dilemma - what to do? There is only one answer - without delay, seek advice at a specialized oncology center, undergo a full examination and possible treatment prescribed by an oncologist. Only a timely and rapid response to the problem and adequate therapy can increase the patient's chances for the quality of his future life, or even just for life itself. Preventive examinations should not be ignored. "Take care of your health from a young age" - this folk wisdom is the best fit for the topic of today's article! Take care of yourself and be healthy!
 [ 23 ]
[ 23 ]