Medical expert of the article

New publications
A bone cyst
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
A bone cyst is a cavity in the hard form of connective tissue, most often developing in childhood, without obvious clinical signs until a pathological fracture due to the destruction of bone tissue.
Bone cyst belongs to a large group of osteodystrophic pathologies of the body's skeletal system. More than 70 years ago, many doctors associated bone cyst with osteoblastoclastoma, then the cyst became an independent nosological entity and today belongs to tumor-like bone diseases. This group includes the following osteodystrophic pathologies:
- Chondromatosis.
- Cysta ossea solitaria (osteocystoma) - solitary bone cyst.
- Cysta ossea aneurysmatica - aneurysmal bone cyst.
- Intraosseous ganglion (juxtacortical cyst).
- Eosinophilic granuloma of bone.
In the international classification of diseases ICD 10, a bone cyst is in class M 85 - "Other disorders of bone density and structure", and is designated as follows:
- M85.4 – single (solitary) bone cyst.
- M85.5 – aneurysmal bone cyst.
- M85.6 - Other bone cysts.
Epidemiology
The statistics regarding bone cysts are as follows:
- Among all benign neoplasms, bone cysts are diagnosed in 55-60% of cases.
- SCC – a solitary cyst is diagnosed in 75-80% of patients.
- ACC – aneurysmal cyst is detected in 20-25% of cases.
- 70-75% of bone cysts are accompanied by pathological fractures.
- Simple solitary cysts most often affect males – 60-65%.
- Aneurysmal cysts are more often diagnosed in girls – 63%.
- The age of patients ranges from 2 to 16 years. Bone cysts are rarely diagnosed in adult patients.
- Simple solitary cysts develop in tubular bones in 85% of cases.
- Localization of solitary cysts in the humerus is 60%.
- Localization of solitary neoplasm in the femur bones – 25%.
- Localization of aneurysmal cysts in tubular bones is 35-37%.
- Localization of aneurysmal cysts in the vertebrae is 35%.
- Formation of aneurysmal neoplasms in the pelvic bones – 25%.
- Bone cysts form in the bones of the upper limbs in 65-70% of cases.
 [ 5 ], [ 6 ], [ 7 ], [ 8 ], [ 9 ], [ 10 ], [ 11 ], [ 12 ], [ 13 ]
[ 5 ], [ 6 ], [ 7 ], [ 8 ], [ 9 ], [ 10 ], [ 11 ], [ 12 ], [ 13 ]
Causes bone cysts
Both types of cystic formations in bone tissue are defined in ICD-10 as tumor-like bone pathology of unspecified etiology.
The causes of bone cysts have been studied for a long time; there is information about clinical observations of similar diseases dating back to the 17th century. In the 19th century, Rudolf Vikhrov first described a bone cyst as a disintegrating enchondroma; later, in 1942, bone cysts were divided into types: juvenile simple cyst and aneurysmal cyst. Terminologically, a cystic bone neoplasm is defined in the classification, but is a constant topic for medical discussions. One group of doctors believes that a cyst is a purely radiological concept, more of a symptom than a separate pathology. In their opinion, cystic formations are a consequence of systemic dystrophic damage to bone tissue. Other theories also have a right to exist, although, like the first, they are not substantiated by reliable clinical and statistical data. For example, one of the versions concerning the etiology of a cyst considers the formation of a benign tumor as a result of the transformation of giant cell tumors. There is also a theory of traumatic etiology, which explains the appearance of a cyst due to solid damage to bone tissue. Currently, the generally accepted version is the theory of dystrophic changes in bone caused by impaired hemodynamics. In turn, blood circulation can be impaired by both trauma and the general inflammatory process of the body. The latest observations of domestic surgeons and orthopedists suggest local dysfunction of intraosseous hemodynamics, activation of fermentation, destruction of glucosaminoglycans, collagen fibers and protein structures. As a result of this pathological chain, osmotic and hydrostatic pressure in the cyst cavity increases, bone tissue is destroyed, which cannot withstand the dynamic load. Thus, the dysplasia process is disrupted in the bone growth zone, ossification changes, pathological hypervascularization of the metaphyseal part and bone tissues is formed, and a cyst is formed.
Such large disagreements lead to the fact that unclear, unspecified causes of bone cysts do not allow for an objective classification of the types, types, and activity of neoplasms, and, accordingly, the possibility of drawing up a single algorithm for the treatment of such pathologies is excluded.
To summarize, we can highlight several of the most reliable options that explain the etiology of bone cyst development:
- A systemic dystrophic process caused by a disruption in the blood supply to bone tissue, as a result of which the absorption of bone tissue (resorption) prevails over the process of osteogenesis (bone formation).
- A disorder of a certain stage in embryonic development, when there is an anomaly in the formation of metaphysis cells of bone tissue. Metaphysis is a structural part of bone tissue, due to which the bone is able to grow in childhood and adolescence.
- Chronic bone trauma.
Symptoms bone cysts
Clinical manifestations, the symptom complex of bone tissue tumors, consists of three main signs:
- The presence or absence of severe pain.
- The tumor itself can be palpated, and its density and estimated size can be determined first.
- The presence or absence of dysfunction of the limbs and motor activity in general.
Symptoms of a bone cyst depend on the type of tumor, the rate of its development, location and ability to spread to surrounding tissues and structures.
Both simple solitary bone cyst (SSBC) and aneurysmal bone cyst have common etiopathogenetic causes, but their symptoms are different, as are the radiological visual indicators. Common symptoms of bone cysts concern the following manifestations and signs:
- The cyst debuts with clinical manifestations against the background of the child’s general health.
- A bone cyst begins to manifest itself as pain when falling or making sudden movements.
- A cyst can provoke a pathological fracture in the area where pain was periodically felt.
Cyst in the leg bone
A bone cyst of the lower limb is most often diagnosed in children aged 9 to 14 years and is defined as fibrous osteitis of the femur or tibia. In 50% of cases, the first clinical symptom that cannot be overlooked is a pathological fracture. Radiologically, a cyst in the leg bone is confirmed in the form of a picture showing a characteristic expansion of bone tissue with a clearly visible resorption zone in the middle. The pathological focus has clear boundaries, especially if there is no reaction from the periosteal hymen (periosteum). A bone cyst of the leg is a benign tumor-like neoplasm and has a favorable outcome in 99% of cases. Bone tissue destruction develops spontaneously, the process begins with transient pain and slight swelling in the area of cyst development.
Symptoms of a leg bone cyst may include:
- Transient pain in the cyst area over a long period of time.
- Impaired support function of the leg, pain when walking.
- Outward rotation of the leg is possible with a pathological fracture.
- There is always swelling in the fracture area.
- When a fracture occurs, the axial load on the leg causes severe pain.
- Palpation of the fracture area causes pain.
- The "sticky heel" symptom is absent.
In clinical orthopedic practice, spontaneous bone restoration within 2-3 years is not uncommon. However, if the cyst is accompanied by a pathological fracture, a cystic cavity remains at the site of bone fusion, which is prone to recurrent development. Nevertheless, surgeons note a paradoxical phenomenon: a fracture can accelerate fibrous restoration of bone tissue, as it helps to reduce the size of the cyst cavity. Often, it is the pathological fracture that is a kind of therapy for the cystic formation itself, and the injury is treated in a standard way, like all other types of fractures. With such development of a leg bone cyst, dynamic observation is required, in which the main examination method is X-ray. With a favorable course of the recovery process, the images show a slow but steady obliteration of the cyst cavity. In more complex cases, when bone destruction progresses, the cyst is scraped out. Then symptomatic treatment is prescribed, including with the help of injectable steroids. Timely treatment of a bone cyst of the lower limb helps to avoid recurrent fractures and pathological shortening of the leg as a result of deformation of the bone tissue.
Talus cyst
Astragalus seu talus, the talus is part of the ankle joint, which also includes the tibia. Talus cyst is most often diagnosed in young people, less often in children under 14 years of age, which distinguishes this pathology from many other bone tissue cysts. It is well known that SCC and ACC are typical diseases associated with dysplasia of the growth zone of the bone, developing in childhood. However, the specificity of the talus is that it is almost entirely responsible for the walking process and takes on the entire weight of a person in motion. Thus, this bone is often subjected to stress, becoming a rather vulnerable area, especially in the presence of osteopathies or calcium deficiency in the bone.
The talus transfers the load to the heel and the midfoot, so its pathologies often manifest themselves as symptoms in the bones of these areas.
Clinical signs of talus cyst:
- The development of a cyst begins in a hidden manner.
- An active talus cyst manifests itself as increasing pain that becomes intense during prolonged walking or running.
- A talus cyst can cause an ankle fracture.
Typically, such a tumor is defined as benign, but it should be removed as early as possible to prevent pathological fractures.
The cyst is visualized as a subchondral neoplasm with clear contours. The tumor does not spread to the joint, but may limit its mobility.
The localization of the cyst in the talus is considered to be unfavorable due to frequent relapses of the pathology even with a carefully performed operation. The high risk of complications is associated with the specific anatomical structure of the talus and its intensive blood supply. Blood flow impairment, both at the time of a pathological fracture and during an inevitable operation in adult patients, can lead to avascular necrosis and even patient disability. In addition, the talus is surrounded by other bone tissues - the calcaneus, navicular, ankle bone, so determining the exact location of the cyst or fracture, and surgical access are very difficult. Surgery for astragalus seu talus cyst is considered one of the most difficult among all surgical techniques for removing bone cysts, and the process of graft engraftment is also difficult. The recovery and rehabilitation time after surgical intervention on the talus can last for 2-3 years. In 5-10% of cases, treatment ends with the patient becoming disabled, mainly in patients over 45 years of age.
Metatarsal bone cyst
Metatarsus, metatarsal bone, is a connection of five small tubular bones, rather short and fragile compared to other bones of the foot. Each of the five parts of the metatarsal bone in turn consists of a base, body and head, the most protruding forward, long is the second metatarsal bone, the shortest and strongest is the first. It is in them that a bone cyst most often forms, although according to statistics, such tumor-like formations in these parts of the foot are rarely diagnosed early and are most likely confused with other bone diseases. In structure, the metatarsal bones are very similar to the metacarpal bones, but still visually look narrower and compressed on the sides, although with all their fragility they successfully cushion our gait, help to withstand static loads of body weight.
Diagnosis of a metatarsal bone cyst is very difficult due to various reasons:
- Rare cases of the disease and the lack of statistically and clinically confirmed information about such pathologies.
- Similarity of symptoms of metatarsus cysts and other tumor-like formations in this area.
- Pathological fractures of the metatarsal bone are common in the presence of osteopathy.
- Lack of uniform diagnostic differential criteria.
Errors in examination and diagnosis of metatarsal cysts or metatarsal cysts are quite common and are one of the reasons for the high percentage of patient disability. In addition, there are descriptions of malignancy of the metatarsal bone cyst, when an advanced process or recurrence of a spontaneous fracture leads to malignancy of the tumor. Diagnostics should be thorough and include, in addition to collecting anamnesis and standard X-ray examination, CT, ultrasound, scintigraphy, and histology. Conservative treatment of metatarsal cysts does not bring results, so they are most often operated on. The only way to avoid surgery may be an uncomplicated fracture, after which the cyst collapses and disappears. But such cases can only occur in a few patients, mainly under the age of 12. Treatment of adult patients is much more difficult and traumatic. The cyst is resected, the bone defect is filled with aloplastic material.
Cyst on the arm bone
Manus – the upper limb, the hand consists of the following anatomical parts:
- Angulum membri superioris - the shoulder girdle, which in turn consists of the following structural parts:
- Shoulder blade.
- Collarbone.
- Articulatio acromioclavicularis - acromioclavicular joint.
- Humerus - shoulder bone.
- Forearm:
- Ulna – paired ulna.
- Radius – paired radius bone.
- Brush:
- The wrist consists of 8 bones.
- Scaphoid, triquetral, lunate, pisiform bones – proximal level.
- Trapezoid, capitate, hamate bones - distal level of the hand.
- The metacarpus, consisting of 5 bones.
- Fingers are the bones of the phalanges.
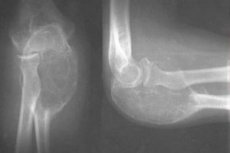
A bone cyst of the arm is mainly localized in the shoulder girdle, much less often cystic dysplasia is noted in the forearm or in the bones of the hand. This is due to the fact that SCC and ACC prefer to form in the metaphyseal sections of tubular long bones, small and short bone structures simply do not have the necessary cavity width for the development of tumors and are not able to intensively and quickly lengthen during the period of intensive human growth - childhood and adolescence. Clinical cases of diagnosis of solitary cysts in the distal phalanges of the fingers of adult patients described in the medical literature can be considered a rarity and most likely, such definitions are erroneous. Quite often, bone cysts are difficult to separate from osteoblastoclastomas or chondromas with similar symptoms. Accurate diagnosis and differentiation is possible only with CT or MRI, which is not always available to patients.
Radiographically, a bone cyst appears as a light, rounded area in the bone metaphysis; the tumor has clear boundaries, inclusions are usually absent, the cortical layer is significantly reduced, often swollen. Histological analysis of the wall of the formation shows weakly vascularized connective tissue with signs of hemorrhage in an aneurysmal cyst or without them when determining a solitary cyst.
The process of developing a cyst in the arm bone is always accompanied by focal destruction, resorption of bone substance. Gradually increasing, the cyst shifts towards the diaphysis, without affecting the shoulder joint, without causing changes in the periosteum and any signs of inflammation in general.
Symptoms of a cystic formation in the upper limb are non-specific, the patient may feel periodic discomfort during rotational movements of the arm, raising the arm up, playing sports. The tumor rarely manifests itself with visual signs, only a large cyst may look like a clear swelling.
The most typical symptom, or rather evidence of the neglect of the process, is a pathological fracture. Most often, the fracture is localized in the forearm, it can be provoked by both physical exertion (lifting weights), and a fall, a bruise. A pathological fracture or bone fracture quickly heals, while the cyst cavity decreases, it disappears.
A cyst on the arm bone is diagnosed using X-rays, osteoscintigraphy, computed tomography and ultrasound. Treatment with timely diagnosis and a small cyst size is carried out conservatively, with immobilization of the upper limb and puncturing. If there is no positive dynamics within 1.5-2 months, the cyst is removed surgically. Surgery is also indicated if the cyst does not decrease after a pathological fracture. It must be removed to avoid a repeated recurrent fracture of the arm.
The prognosis of a cyst in the arm bone in children is generally favorable, the specificity of the child's body is that the ability to self-correct and reparate at this age is very high. In adults, the process of recovery, rehabilitation of the arm lasts much longer, damage to muscle tissue during surgery can provoke some limitations in the functions of the upper limb. In addition, there is a risk of rejection of the bone implant introduced into the resection defect. Complete implantation of alloplastic material or autotransplant requires from 1.5 to 3 years.
Solitary bone cyst
In the last century, a solitary simple cyst was considered the final stage of the formation of a giant cell bone tumor. Currently, a solitary bone cyst is considered an independent nosological unit according to ICD-10. The disease most often affects children and adolescents, it is no coincidence that it is also called a juvenile bone cyst.
Cysta ossea solitaria or solitary bone cyst is diagnosed more often than aneurysmal neoplasm. In 65-70% of cases, a solitary cyst is detected in childhood in boys and looks like a benign single-chamber formation, localized mainly in the shoulder girdle or in the hip bones. Symptoms of a simple bone cyst are nonspecific, often the manifestation of a clinical sign and the reason for visiting a doctor is a pathological fracture. Statistically, among patients with a solitary bone cyst (SBC), boys aged 9 to 15 years predominate. Solitary cysts do not occur in adult patients, thus, the established diagnosis of SBC in people over 40 years old can be considered an error associated with insufficient differentiation of benign bone tumors.
Localization and symptoms of solitary bone cyst:
- The predominant area of development of SCC are tubular long bones - the shoulder girdle area, femurs. Localization of a simple cyst in small short bones is not typical and requires careful differentiation from chondroma, sarcoma, ganglion.
- SCC develops asymptomatically over a long period, sometimes up to 10 years.
- Indirect signs of the development of a solitary cyst may include transient pain in the area where the tumor is located.
- In the area of cyst development, if it increases to 3-5 centimeters or more, a small visible swelling is possible.
- A characteristic sign of a formed large cyst is a pathological spontaneous fracture, uncomplicated by displacement.
- During the initial examination and palpation, the cyst is felt as a painless lump.
- Pressure on the wall of the neoplasm causes the destroyed bone area to bend.
- The cyst does not limit the range of motion, with the exception of a femoral cyst, which causes intermittent claudication.
A solitary bone cyst develops within the clinical stages:
- Active development of the cyst causes a thickening of the bone visible on an X-ray image, and can provoke a pathological fracture and immobilization of the damaged joint. The active stage lasts from six months to 1 year.
- The passive stage of cyst development begins with the moment of tumor displacement to the center of the bone, while the cyst significantly decreases in size and collapses. This stage can also be asymptomatic and lasts from 6 to 8 months.
- The bone restoration stage begins from the moment the bone system stops growing, 1.5-2 years after the onset of the active stage. However, destructive bone lesions remain and can still be a provoking factor for a pathological fracture. The fracture, in turn, promotes the closure of the cyst cavity and the compensatory replacement mechanism of filling the cavity with bone tissue.
Juvenile solitary bone cyst is most often treated conservatively and with immobilization of the damaged area. If this method does not produce results and the disease progresses, the cyst is removed surgically, resection is performed within the intact tissues with mandatory allo or autoplasty.
Treatment of patients over 16-18 years of age is 90% surgical, since detection of a cyst at this age indicates its long-term development and significant destruction of the bone, which is a huge risk of multiple recurrent fractures.
Aneurysmal bone cyst
ACC or aneurysmal bone cyst is quite rare in surgical practice, but the complexity of its treatment is due not to isolated diagnoses, but rather to the unspecified etiology. In addition, ACC is most often detected in the spine, which in itself indicates the seriousness of the disease and the risk of complications from the spinal cord. A large aneurysmal cyst or multi-chamber tumor localized in the bone tissue of the vertebra can cause paresis and paralysis, and also has a tendency to malignancy.
AAC is a significant, extensive lesion of bone tissue, the cyst looks like a multi-chamber, less often a single-chamber cavity filled with blood exudate, the walls can be interspersed with small bone parts. Until the middle of the last century, an aneurysmal tumor was not identified as an independent disease and was considered a type of osteoblastoclastoma. Today, AAC is diagnosed as a benign tumor, burdened with multiple complications when localized in the spine area.
The specificity of the development of an aneurysmal cyst is that it is very aggressive, unlike a solitary tumor. Rapid growth and increase in its size sometimes resembles a malignant process, however, AAC very rarely becomes malignant and is quite successfully operated if detected in time. Most often, AAC is diagnosed in children during the period of intensive growth - 6 to 15-16 years old, according to some information, aneurysmal tumors predominate in girls, although this information is contradictory and not confirmed by reliable statistics. The favorite localization of AAC is the cervical and thoracic spine, sometimes it forms in the bones of the hip joint, in the lumbar region and extremely rarely in the calcaneus. A large AAC can capture several vertebrae at once - up to 5, which is complicated by paralysis, including irreversible.
Symptoms of ABT – aneurysmal bone tumor:
- The onset may occur without clinical signs, asymptomatically.
- As the cyst grows, the child experiences transient aching pain in the area of the damaged bone.
- The pain intensifies with physical exertion, tension, and may bother you at night.
- In the area where the cyst is formed, swelling is clearly visible.
- A cyst located near a joint limits its range of motion.
- An aneurysmal tumor in the femur causes lameness and disrupts the supporting function.
- A large cyst causes paresis and partial paralysis, which debut at first glance without any apparent objective reason.
- Trauma or bruises can provoke the acceleration of cyst development.
AAC can have the following forms of development:
- Central AAC – localization in the center of the bone.
- Eccentric AAC - an enlarging cyst that invades nearby tissues.
An uncomplicated aneurysmal bone tumor can close on its own after a pathological fracture, but such cases are very rare, most often AAC has to be operated. The most difficult operations are considered to be those to remove a cyst on the vertebra, since the surgeon works with a very vulnerable and dangerous area - the spinal column and multiple nerve endings. After removing AAC, a very long recovery period is required, rehabilitation measures, in addition, aneurysmal cysts are prone to recurrence even in the case of a carefully performed operation. The risk of relapse is very high, according to statistics, 50-55% of patients who have undergone surgical treatment are again referred to the surgeon. The only way to reduce the risk of relapse can be constant medical supervision and regular examination of the skeletal system.
Where does it hurt?
Forms
Symptoms of a bone cyst depending on its type:
- Solitary, juvenile bone cyst is most often diagnosed in boys - in 60-65% of cases. In adult patients, SBC is extremely rare and can be considered an advanced dystrophic process that has not been diagnosed for a long period. Most typically, a solitary cyst manifests itself at the age of 9 to 16 years, when the child begins the process of intensive growth. The favorite place for localization of SBC is considered to be long tubular bones, as a rule, this is the metaphysis of the femur or humerus. The onset of pathology is latent, asymptomatic, occasionally the child may complain of periodic pain in the bone or swelling in the area of cyst development. In 60-70% of cases, the first obvious sign of SBC is a pathological fracture caused by mild trauma - a slight bruise or a simple fall. When a tubular bone is affected by a cystic neoplasm, it thickens and has a peculiar club-shaped form in the area of cyst development. Palpation of the bone does not cause painful sensations, pressure on the cyst wall shows some deflection in the area of softening of the bone tissue. The joint, limb do not lose mobility, their functions, the only problem for the motor activity of the femur or ankle bone can be the loss of the proper sense of support. The development of a simple bone cyst occurs in certain stages:
- The active stage of development, which lasts about a year and is characterized by swelling, rarefaction of the metaphysis, which corresponds to the X-ray picture showing a clear process of osteolysis - complete destruction of the bone without compensatory replacement by other tissues. At the same time, the limitation of mobility of the nearby joint, contracture, and there may be recurrent pathological bone fractures are clearly felt.
- The active phase gradually passes into a latent, passive stage. This is especially characteristic of the development of a cyst that is not accompanied by fractures and pain. The cyst can capture the metadiaphysis, gradually shifting further from the growth zone, decreasing in size. A solitary cyst in the passive stage is always asymptomatic and can be latent for up to six months.
- Bone tissue restoration stage. The latent solitary cyst slowly moves to the diaphysis, this occurs over a period of one and a half to two years. During this time, destruction occurs in the bone tissue, but it does not manifest itself clinically, an exception may be a sudden fracture against the background of complete health and the absence of a traumatic factor - a fall or bruise. Fractures are also not felt as strong, traumatic and, depending on the localization, can be carried by the child literally - on their feet. Fusion, the fracture sites contribute to the narrowing of the cyst cavity, reducing its size. In clinical orthopedic practice, this phenomenon is called restoration in place. In the area of the bone cyst, a seal or a very small cavity may remain. However, the bone restoration process is completed, in general, about 2 years pass from the debut of the development of a solitary cyst to its reduction.
- An aneurysmal cyst is most often diagnosed in girls, the neoplasm develops in bone tissue of various structures and localizations - in tubular bones, in the spine, in the pelvic or femoral bones, very rarely - in the calcaneus. In girls, an aneurysmal cyst is clinically manifested in puberty, before the first menstrual cycle until the hormonal system is completely stabilized. At this time, not only the hormonal background changes, but also the blood coagulation system, which significantly affects the blood supply to bone tissue. At the age of 11 to 15 years, ACCs of the femur are most often diagnosed. Unlike a solitary cyst, an aneurysmal cyst is characterized by a very acute, clinically manifested onset, the symptoms of which may be as follows:
- Painful sensations, paroxysmal, localized at the site of cyst development.
- Visible swelling, puffiness of the bone.
- A lump that can be clearly felt.
- Local hyperthermia, possible reddening of the skin in the area of the cyst.
- Dilation of the venous vessels at the site where the ACC develops.
- In case of pathological fractures of the vertebra in the acute stage, paresis or partial paralysis is possible.
- After the acute stage, the symptoms of the bone cyst subside, the process stabilizes, but tissue destruction continues.
- Radiologically, stabilization of the acute period looks like significant resorption of bone tissue; in the center of the lesion there is a capsule that includes within its borders clots of fibrinous tissue, the remains of the hemorrhage process.
- ACC in the pelvic bones can reach enormous sizes – up to 20 centimeters in diameter.
- During the stabilization period (6-8 weeks), calcification of bone tissue is possible, therefore this form of cyst is called an ossifying subperiosteal aneurysmal cyst.
- With an aneurysmal cyst developing in the spine, a visible extensive compaction and swelling of the bone are possible. In addition, the child develops compensatory muscle tension, which aggravates the pain symptom.
- A specific compensatory posture is characteristic of spinal cord damage – support of the hands on the hips, pelvic bones, often children in a sitting position try to support their head with their hands. All this indicates a violation of the normal supporting function of the spinal column.
In general, symptoms of ACC develop within clinically defined phases:
- I – resorption and osteolysis.
- II – limited mobility.
- III – recovery phase.
The period of development of an aneurysmal bone cyst from the onset of the disease to the last phase can last from one to three years. Also, relapses are typical for ACC, according to surgeons-pathologists, they reach 30-50% of all identified cases.
Diagnostics bone cysts
Diagnosis of bone cysts is always difficult, this is due to the absence of specific symptoms, and a similar radiographic picture of other neoplasms, and not fully clarified etiology of intraosseous benign tumors. In the process of determining the type and nature of the course of the cyst, errors are often made, their percentage is very high - up to 70% of erroneous diagnoses. Inaccurate diagnosis of bone cysts leads to incorrect treatment tactics and frequent relapses, less often increases the risk of tumor malignancy.
What do need to examine?
How to examine?
Differential diagnosis
The main fundamental criteria for the accurate differentiation of benign tumor-like formations in the bone are clinical and radiological parameters, indicators:
- Anamnesis, medical history.
- Age of the patient. In most cases, the development of a solitary or aneurysmal cyst is typical for childhood and adolescence.
- The localization of a bone cyst is not only in the anatomical structure of the body, but also in the structure of bone tissue.
- Size of the focal lesion.
- Presence or absence of a pathological fracture.
- Histological indicators.
It is very important to differentiate bone cysts from malignant intraosseous tumors, which require urgent and specific treatment. Such diseases may include osteogenic or osteoclastic sarcoma, osteoblastoclastoma, carcinoma.
The difference between an aneurysmal cyst and malignant tumors may be its preferential localization in tubular, large bones and location in the metaphysis, diaphysis. A solitary tumor, unlike malignant neoplasms, never causes a reaction from the periosteum and does not spread to nearby tissues.
Differential criteria that help to distinguish a malignant process from SCC or ACC
Disease |
Osteoblastoclastoma |
ACC or SKK |
Age |
20-35 years and older |
2-3 years - 14-16 years |
Localization |
Epiphysis, metaphysis |
Metaphysis, diaphysis |
Bone shape |
Obvious swelling of the bone |
Spindle shape |
Contours of the destruction focus |
Clear boundaries |
Clear |
State of the cortical layer |
Intermittent, thin, wavy |
Smooth, thin |
Sclerosis |
Not observed |
No |
Periosteal reaction |
Absent |
Absent |
State of the pineal gland |
Thin, wavy |
No obvious changes |
Adjacent diaphysis |
No changes |
No changes |
Methods that may be included in the diagnosis of bone cysts:
- Collection of anamnesis – complaints, subjective and objective symptoms, presence of pain, its radiation, time and duration of symptoms, their dependence on the load and the possibility of relief with medications.
- Clinical examination.
- Determination of orthopedic status – posture in motion, at rest, functional activity, limb asymmetry, muscle symmetry, presence or absence of contracture, identification of changes in vascular pattern.
- Radiography.
- Contrast cystography.
- Computed tomography.
- Ultrasound.
- MRI – magnetic resonance imaging.
- Computer thermography – CTT.
- Puncture.
- Determination of intraosseous pressure - cystobarometry.
Bone cysts are differentiated from the following diseases:
- Osteosarcoma.
- Giant cell tumor.
- Nonossifying fibroma.
- Osteoma.
- Primary osteomyelitis.
- Osteoblastoma.
- Chondroma.
- Lipoma.
- Chondroblastoma.
- Fibrous dysplasia.
Topical diagnostics is also indicated before surgery to remove the cyst or bone marrow cyst; in addition, the patient requires dynamic observation, and therefore periodic diagnostic monitoring of the condition of the cyst and bone tissue in general.
Who to contact?
Treatment bone cysts
Despite the availability of high-tech equipment and new treatment methods, bone cysts are still considered a difficult to treat disease that is prone to recurrence.
A bone cyst diagnosed in childhood and not having complications is treated with conservative methods. Surgeries are indicated only for children over 3 years old, in cases of aggressive development of the process. If the tumor provoked a spontaneous fracture, the treatment of the bone cyst consists of standard steps that orthopedists and surgeons take in the treatment of common traumatic fractures. At the slightest suspicion of a fracture, an immobilizing material is applied to the bone - a splint, then diagnostic measures are carried out. A cyst and a fracture in the hip, shoulder area require a plaster cast and immobilization for 1-1.5 months. If a cyst is detected, but there is no fracture, the patient is shown maximum rest and unloading - a sling bandage on the shoulder or the help of a stick, crutches when walking. Conservative treatment also includes punctures, which can significantly speed up the process of bone tissue reparation. Treatment of a bone cyst with a medicinal puncture is as follows:
- Intraosseous anesthesia is administered.
- The cyst is punctured and material is taken from it for histological examination.
- The punctured cyst cavity is washed with an aseptic solution.
- A protease inhibitor is introduced into the cavity to neutralize aggressive fermentation (contrycal). For children over 12 years of age, the introduction of kenalog or hydrocortisone into the cavity is indicated.
- The end of the puncture is perforation of the cyst from all sides to create an outflow of exudate and reduce intracavitary pressure.
- The puncture is performed several times at a time determined by the surgeon (2-4 weeks).
- After completion of treatment, monitoring of the bone tissue condition is required using X-rays (2-3 months after the last puncture).
- During the puncture, the area of the bone affected by the cyst must be immobilized.
- After successful puncture and closure of the cyst cavity, a course of exercise therapy is prescribed for at least 6 months.
The total duration of conservative treatment of a bone cyst is at least six months. If conservative treatment is ineffective, as confirmed by dynamic observation for 2-3 months, the cyst is subject to surgical removal by resection and subsequent bone grafting with autologous or alloplastic material.
Folk remedies for the treatment of bone cysts
It is obviously inappropriate to talk about folk remedies for treating bone cysts. Any neoplasm developing in the body is considered tumor-like, that is, prone to complications and a more serious process - malignancy. Bone cysts are considered a poorly studied pathology, the etiology of which has not yet been determined, so folk remedies for treating bone cysts not only do not help, but can also harm.
The ineffectiveness of treating bone cysts with so-called folk methods is due to the pathogenetic features of tumor formation. The pathogenesis is based on a local disruption of the blood supply to bone tissue. Such intraosseous "starvation" leads to the activation of the enzymatic function, lysis, which results in the destruction of glycosaminoglycans, protein elements and collagen structures. This complex process is always accompanied by increased osmotic and hydrostatic pressure in the cyst cavity, other chronic destructive processes inside the bone. That is why folk remedies for the treatment of ACC or SCC are not able to bring the desired benefit, the barrier for active plant substances is too high, preventing them from achieving the goal.
In addition, all patients willing to experiment with their health should pay attention to the key word "tumor" in the diagnosis, since a bone cyst is a benign tumor-like formation. Treatment of vertebral cysts with untested means is especially dangerous, because all neoplasms in the spinal column are prone to malignancy and inadequate therapy can lead to irreversible consequences.
The only remedy that is relatively safe and can somewhat alleviate the symptoms of a pathological fracture caused by a cyst may be a special diet. The patient's diet should include foods that
Rich in vitamins, calcium. It is very useful to eat fruits, vegetables rich in vitamin C, the presence of vitamin D and phosphorus is also important.
Products that help restore bone tissue faster:
- Milk and fermented milk products.
- Fish, including sea fish.
- Sesame seeds.
- Citrus.
- Sweet bell pepper.
- Currant.
- Cherry.
- Hard cheeses.
- Jelly, marmalade, any products containing gelling agents.
Carbonated drinks should be excluded from the menu, and consumption of sweets and coffee should be limited.
Otherwise, treatment of bone cysts should be carried out under strict medical supervision, and not with the help of dubious and unverified recommendations, since only adequate therapy can restore motor activity and restore normal functions of the skeletal system.
Prevention
To date, there are no uniform recommendations for the prevention of solitary or aneurysmal bone cysts. Prevention of bone cysts in pediatric and older patients can only consist of following these simple rules:
- Regular medical check-ups, starting from the moment of the child's birth. A surgeon's consultation should become a mandatory annual procedure; if there are alarming symptoms - complaints about pain, gait disturbances, movements, posture, the help of a surgeon or orthopedist is needed immediately. The earlier a bone cyst is detected, the more successful the treatment will be and most likely surgery will not be required.
- The recurrence of a cyst in bone tissue can only be prevented by surgical intervention and subsequent long-term treatment, which should not be interrupted even if recovery appears.
- Children with a history of diseases of the skeletal system, musculoskeletal system, systemic diseases, protracted chronic inflammatory processes should be protected from any traumatic, mechanical factors.
- Children and adults involved in active sports should undergo medical examinations, including X-rays of the skeletal system, more often than those who lead a passive lifestyle. Professional injuries, bruises can become a factor causing the development of an aneurysmal bone cyst.
- Parents should be attentive to any changes in the child's health. Most often, the onset of the development of SCC and ACC is asymptomatic, only periodically disturbing the little patient with transient pain. In addition, pathological fractures do not always manifest themselves in the clinical sense as standard fractures, their only sign may be a slight limp, limited range of motion of the arm, compensatory postures that help reduce the load on the spine.
Prevention of bone cysts in the absence of uniform standard rules should obviously become the responsibility of the person himself or, if we are talking about a child, his parents.
Forecast
Obviously, only the attending physician can talk about the prognosis of a bone cyst. Everything depends on the patient's age, the duration of the latent period of cyst development, the presence or absence of complications, and a pathological fracture.
In general, the prognosis for a bone cyst is as follows:
- Children under 15-16 years old – the prognosis is favorable in 85-90% of cases. Relapses occur with an aneurysmal cyst or technical errors made during surgery. Repeated surgeries, although traumatic, are not considered severe. In addition, the child's body has a high degree of reparative capacity, so restoration of motor activity is guaranteed in 99% of cases.
- Adult patients have a harder time with bone cyst treatment, and they are more likely to have relapses. In addition, diagnosing ACC in patients over 35-40 years old is difficult, the cyst has to be differentiated from other tumor-like diseases, most often against the background of a pathological fracture. A fracture is also more difficult to tolerate, the recovery period is much longer than in children. The prognosis for bone cysts in adult patients is favorable in 65-70% of cases, the rest of the diseases are undifferentiated malignant or complex tumors, including intraosseous ones. Also, the likelihood of successful recovery is reduced by incorrectly chosen treatment tactics. Conservative therapy for bone cysts can only be effective in childhood, in other patients it can lead to massive bone destruction and serious complications. Vertebral cysts are the most dangerous in terms of compression symptoms and general vulnerability of the spinal column.
The statistical data on the recurrence of the process are as follows:
- SBC (solitary bone cyst) – relapses occur in 10-15% of cases.
- ABC (aneurysmal bone cyst) has a 45-50% recurrence rate.
In general, the prognosis of a bone cyst depends on timely and differentiated diagnostics, which in turn determines the therapeutic tactics and strategy of the rehabilitation period.
A bone cyst is considered a benign formation that can be classified as a borderline condition between a true tumor and an osteodystrophic process of bone tissue dysplasia. The main danger is the long asymptomatic course of the disease, which most often ends in a pathological fracture. A bone cyst localized in the upper body - in the upper limbs, shoulder girdle, in the vertebrae, not burdened with a fracture, as a rule, does not require surgical treatment. A bone cyst of the lower limbs is enucleated in order to prevent the potential risk of fractures or their recurrence. Solitary bone cysts tend to spontaneously resolve, aneurysmal neoplasms are more pathological, although in 90-95% with adequate and timely treatment their prognosis is also favorable, the only complication can be considered a fairly long recovery period, requiring patience from the patient and compliance with all medical recommendations.