Medical expert of the article

New publications
Corrective osteotomy
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Corrective osteotomy is indicated in case of trauma, bone deformities, improper bone fusion. The operation involves dissection of the bone under general anesthesia, with further fixation of its parts with the help of special instruments. The term "osteotomy" from the Greek language translates as "bone dissection". Conditionally, osteotomy can be called artificial, intentional damage to the bone to optimize its configuration and condition. As a consequence of such an intervention, the deformity disappears, the fragments fuse properly, which allows the patient to return to a normal way of life in the near future.
Indications for the procedure
Corrective osteotomies are performed on various bones and joints. Depending on the specific situation, the intervention can be performed:
- For the purpose of repositioning and ensuring physiologically correct positioning of the bone;
- To correct curvature, to give the necessary bone configuration;
- To correct the length of a limb that has congenital or post-traumatic changes.
Corrective osteotomy directly involves bone dissection for subsequent correction of position and shape with further fixation of the fragments using special devices. First, the bone is artificially dissected (broken), its position is corrected, and then its parts are fixed using various devices (hinges, plates, implants, etc.). As a result of such manipulations, the fragments are fused in the correct position. After the necessary rehabilitation, the patient can return to the usual way of life.
Indications for corrective osteotomy may include:
- Injuries with or without compromised bone integrity (complete or partial fractures, dislocations or subluxations);
- Incorrect fusion after traumatic injury, self-treatment, improper intervention, etc;
- Congenital curvatures and defects;
- Complications of chronic pathologies (joint ankylosis, rickets, arthrosis, etc.).
Depending on the technique used, there are the following types of osteotomies:
- Closed corrective osteotomy is performed without violating the integrity of soft tissues (the specialist performs bone correction without incisions);
- Open corrective osteotomy involves mandatory soft tissue dissection to provide direct access to the affected bone.
Depending on the indications, the following types of intervention are distinguished:
- Osteotomy to correct the curvature (directly corrective osteotomy).
- Surgery for limb lengthening (involves excision of the bone of a longer limb with further osteosynthesis - hinge connection using special fixation devices). This type of intervention is often referred to as an articulated osteotomy.
The directionality of the artificial fracture is differentiated:
- Derotational (transverse) osteotomy;
- Linear (along the bone);
- Wedge-shaped (with a complicated triangle-type trajectory);
- Zigzag;
- Stepped (in the form of stair treads);
- Arc-shaped.
Corrective osteotomy is also known to be classified according to the area of the body on which it is performed:
- Femoral osteotomy is indicated for patients with valgus deformity, femoral neck fracture, dislocation or subluxation;
- Mandibular osteotomy (so-called Rauer's oblique osteotomy, etc.);
- Limb-reconstructing surgery;
- Osteotomy for repositioning the tibia, tibia, etc.
Preparation
Corrective osteotomy surgery is performed routinely. At the preparatory stage, the patient must undergo an appropriate examination plan, which includes:
- A general blood and urine examination to evaluate the circulatory and urinary systems;
- Blood glucose levels to rule out diabetes mellitus;
- Biochemical blood tests to detect liver and kidney dysfunction;
- A coagulogram to determine the quality of blood clotting;
- Fluoroscopy, electrocardiography;
- X-rays to assess the degree of musculoskeletal changes and determine the extent of surgical intervention;
- CT scan or MRI if indicated.
In addition, consultations with other specialists such as a general practitioner, surgeon, orthopedist, anesthesiologist, cardiologist, etc. Are often required.
Patients who are overweight are advised to follow a special diet at least a few weeks before the operation. Immediately before the corrective osteotomy, you should refrain from eating and drinking 10-12 hours before the intervention. The patient should take a shower in the morning. If there are any chronic diseases that require regular medications, it is necessary to tell the doctor in advance: it may be necessary to refuse to take these medications during the operation and postoperatively.
Technique of the corrective osteotomy
The surgery is performed under anesthesia, adhering to the following steps:
- Administering anesthesia;
- Incision of soft tissues with their dilatation with the help of fixators;
- Dissecting the bone with a chisel or osteotome;
- Juxtaposition of broken fragments, removal of some of them, replacement with a graft (if indicated);
- Bonding of the fragments using appropriate fixings;
- Wound closure.
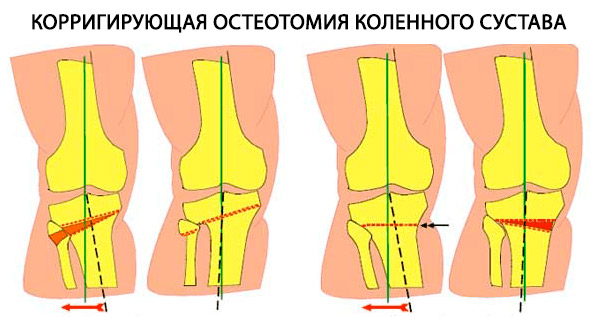
Corrective tibial osteotomy is performed to restore the pathologically altered limb and redistribute the load on it. For this purpose, the disturbed segment of the articulation is "unloaded" by transporting the fulcrum as close to its anatomical location as possible. Corrective osteotomy of the tibia is performed in stages:
- Wedge-shaped artificial fracture of a bone using an osteotome.
- Fixation of fragments using special fasteners (screws, plates).
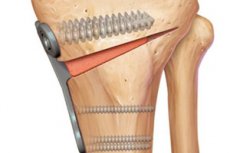
Corrective osteotomy of the knee joint involves performing an artificial fracture of the tibia with the subsequent placement of a special plate, which helps to change the axis of the limb and relieve pressure on the affected cartilage. Also partially cross the tibia, correct the curvature, after which the area is fixed in the desired position. There is no need for external immobilization. The total duration of the operation is about 50-60 minutes. The patient remains in the hospital for 3-4 days. [1], [2]
Corrective osteotomy of the foot is indicated in patients with valgus deformity of the first toe, hallux valgus, associated with chronic biomechanical disorders and changes in the first metatarsophalangeal joint. The surgery involves making an incision in the first metatarsal bone and stabilizing its position. One of the common types of this surgery is Scarf-osteotomy. Currently, the corrective osteotomy of the first metatarsal bone is performed percutaneously, with minimal traumatization of tissues, which reduces the likelihood of postoperative scarring and shortens the rehabilitation period. [3]
The forefoot is operated on as follows:
- Cut into the lateral surface of the foot;
- Perform a bone osteotomy and put the articulation of the first metatarsal bone in the correct position;
- Remove the pineal mass;
- Fix the first phalanx with screws or spokes;
- Restore the anatomically correct position of the ligamentotendinous apparatus;
- Stitches.
Corrective osteotomy of the tibia is performed in several variants: [4]
- Linear osteotomy with bone graft introduction.
- Wedge osteotomy with removal of the wedge of bone.
- Angle osteotomy.
In the hip region, in valgus or varus curvatures, patellofemoral contractures, and paralysis of the rectus femoris muscle, corrective surgery is performed primarily in the supramuscular zone.
Corrective femoral osteotomy for valgus and varus curvature is performed in two variants: [5]
- Linear with bone grafting.
- Wedge-shaped with removal of the wedge of bone.
Surgery in the diaphysis of the humerus is performed to correct a malunion of a fracture, more commonly a suprascapular fracture. [6], [7] Corrective osteotomy of the humerus can be performed as:
- Angle osteotomy for malunion of a surgical neck fracture of the shoulder;
- Suprascapular osteotomy in patients with varus curvature of the humerus.
To lengthen the limb, an oblique osteotomy is performed with further application of skeletal traction to the distal end. The required length, which is usually within the range of 2-7 cm, is achieved by dosing the weight. A segmental osteotomy according to Bogoraz can be used to equalize and lengthen the limb at the same time. Compression-distraction devices are used for lengthening, which are applied to the bone area after the osteotomy. This method allows to lengthen the limb up to 20 cm with preservation of motor capabilities in the adjacent joints. The daily lengthening rate is about 1 mm.
Corrective osteotomy of the radius is performed using palmar or rear access. The palmar access is suitable for the consequences of flexion fractures using palm plates with angular stability. [8], [9] An incision of up to 10 cm is made along the radial flexor of the hand, which, once exposed, is withdrawn toward the elbow. The periosteum is peeled off the metaphysis, lifted and separated. In the area of incorrect fusion an osteotomy and open juxtaposition of the fragments are performed. [10] The necessary graft is placed in the formed defect, fixed with Kirschner spokes, or the ulna is shortened with osteosynthesis with the LCP plate. The wound is drained and sutured layer by layer. [11]
The dorsal access is suitable for correcting the consequences of extensor fractures. A linear dissection is performed in the area of Lister's tubercle projection with an incision of the proximal zone of the dorsal ligament of the wrist. The extensor canals of the second, third, and fourth fingers are opened, extensor tendons are withdrawn to the sides. In the area of incorrect fusion, an osteotomy and open juxtaposition of the fragments are performed. A graft is placed in the formed defect and osteosynthesis is performed using LCP plates.
Corrective pelvic osteotomy is used to optimize and restore support function - in particular, to create a support zone for the proximal segment of the femur. This technique is indicated in patients with congenital hip dislocation, valgus or varus curvatures, false articulations of the femoral neck. The operation is performed on the pelvic bones or femur. [12], [13]
Patients with ankylosis of the hip are intervened according to the curvature detected. McMurry intervertebral osteotomy is performed on patients with pseudarthrosis of the femoral neck and stage I or II coxarthrosis. During the operation, in pseudarthrosis, the load is transferred from the fracture feature to the femoral head, while in coxarthrosis, its full immersion in the acetabulum is ensured.
Contraindications to the procedure
Corrective osteotomy may not always be used. The patient will be refused if he/she has the following contraindications:
- Disorders of bone formation, including age-related disorders (corrective osteotomy is not performed on persons over 60-65 years of age);
- Osteoporosis;
- Excessive overweight, obesity (intervention may be delayed until body weight is normalized);
- Rheumatoid arthritis;
- Circulatory (blood supply) disorders in the area of the proposed operation;
- Pustular dermatopathology, skin infection in the area of the proposed surgery;
- Any trimester of pregnancy, breastfeeding period until the baby reaches 1.5 years of age;
- Various decompensation states, general severe pathologies;
- Clotting disorders;
- Pathologies of bone and cartilage repair.
As you can see, some contraindications are absolute, and some are temporary - that is, corrective osteotomy can be performed after they are eliminated. Only the operating surgeon decides whether the operation can be performed.
Consequences after the procedure
Before referring a patient for surgery, the doctor must necessarily inform him about possible complications and adverse effects of this intervention, even if the risk of their development is minimal. Theoretically probable complications after the procedure:
- Infection in the wound, suppuration;
- Improper fusion due to displacement of bone fragments;
- The formation of a false joint;
- Weakening or loss of skin sensation;
- Implant rejection;
- Delayed tissue regeneration, prolonged recovery.
Among the transient temporary impairments:
- The appearance of a thickening in the area of the incision;
- Sensory disturbances;
- Redness, pain in the area where the surgery was performed.
To minimize the risk of postoperative complications, the patient is prescribed appropriate medications (including antibiotics), physical procedures, exercises LFK. If timely and adequate measures are taken, the rehabilitation period is significantly reduced and facilitated.
Care after the procedure
The course and duration of the rehabilitation period depend on the general condition and age of the patient, as well as the type of surgery. For example, corrective osteotomy of the tibia requires longer recovery, up to three months or more. At the same time, the bone fragments fuse completely after 4-6 months at the earliest (provided the surgery was successful and the patient's general condition is normal).
For the fastest tissue regeneration, it is important to adhere to all doctor's recommendations:
- Limiting the load on the operated limb;
- Adherence to a special diet;
- Performing LFK exercises;
- Massage;
- Physical therapy;
- Taking analgesics and recuperative medications;
- Use of special orthopedic devices approved by the attending physician.
Corrective knee osteotomy is characterized by a shorter rehabilitation period. It is important to follow these recommendations throughout the rehabilitation period:
- Day 1: Application of elastic bandage or splint, bed rest, ice compress. Movement to the toilet is possible with the use of crutches. Dosed isometric load on the muscles of the thighs and lower leg is recommended.
- Day 2: Application of elastic bandage, limited flexion and extension of the leg in the knee joint under medical supervision, cold application, isometric exercises.
- Day 3: Application of compression hosiery, practicing movements under the supervision of a doctor, applying cold.
- For 1.5 months: Application of a bandage, compression hosiery. Practicing knee movements without making sharp turns. Walking with crutches, lymphatic drainage massage, measures to prevent blood clots.
- 1.5 months after surgery: Control radiography, motor activity according to the results of the examination. Movement training, exercises to restore muscle strength.
Sporting activities on the knee joint are allowed no earlier than 10 months after the intervention.
In general, corrective bone osteotomies involve subsequent, sometimes prolonged, wearing of elastic bandages, orthoses, compression underwear. Motor activity is increased strictly gradually, under the supervision of a specialist. The patient moves at first on crutches, then the load is gradually increased. Training exercises are strictly dosed, starting with extension and flexion movements, with a gradual increase in activity. Physiotherapy is mandatory: cold application, use of heparin ointment, lymphatic drainage massage, prevention of thrombosis. More active training should begin no earlier than 7 weeks after surgery.
Corrective osteotomy is a high-tech reconstructive intervention actively practiced to correct bone and joint curvatures by aligning the loading axis. This method demonstrates good results and often avoids endoprosthetics.