
Treatment of rheumatoid arthritis and pain relief in the legs
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Today, the goal of curing rheumatoid arthritis, which causes severe pain in the legs, is a reduction in inflammation of the joints and pain. Another task is to maximize the function of the joints and prevent their destruction and deformation. The earlier a person begins to treat arthritis, than he will achieve great success. Aggressive pain management can improve the function of the joints, stop their damage and reduce the pain in the legs. How to do it?
The problem of optimal treatment of arthritis
Optimum cure of the leg joints from this disease includes a combination of medications, rest, exercises to strengthen the muscles, joints and ligaments, their protection, and information about the disease for the patient. Treatment depends on the overall health status, age of patients and their physical activity. Treatment is most successful if the patient and the doctor cooperate with each other.
In the treatment of rheumatoid arthritis, at least two classes of drugs are used: from the first row - fast-acting and second-line medications - delayed action. They are better known as modifying pains antirheumatic.
The so-called first-line drugs are cortisone and aspirin (corticosteroids), which doctors use to reduce inflammation and pain in the legs. Preparations of the so-called second series are called to promote the remission of arthritis and are able to prevent aggressive destruction of the joints.
The degree of destruction of leg joints in rheumatoid arthritis varies depending on the general condition of the affected. Those who suffer less destructive forms of the disease can manage leg pain. With early treatment, the function of the legs improves and the risk of disability, like the destruction of the joints of the legs, is minimized. But this is provided that the person was treated earlier with second-line drugs (pain-modifying antirheumatic drugs.
Most people require more aggressive second-line drugs, such as methotrexate, and anti-inflammatory drugs are also needed. From time to time these medications of the second line are used in combination. In some cases, they counteract severe deformity of the leg joints, and then surgery may be necessary.
"The first line" of medicines for rheumatoid arthritis
Acetylsalicylate (aspirin), naproxen (Paracetamol), etodolac (Lodine) and ibuprofen and are examples of non-steroidal anti-inflammatory drugs (NSAIDs). They are drugs that can reduce inflammation of the tissues, pain and swelling of the legs in rheumatoid arthritis. Aspirin in doses exceeding those that people take to treat headaches and fever are effective anti-inflammatory drugs for the treatment of leg joints during the course of rheumatoid arthritis.
Aspirin has been used to treat and improve joints since ancient Egyptian times. New NSAIDs are as effective as aspirin, to reduce inflammation and pain, and require much smaller doses per day. The response of patients to various NSAID medications is changing. Therefore, it is not unusual for a doctor to try several NSAIDs in order to identify the most effective agents, with the least side effects.
Fighting the side effects of drugs
The most common side effects of aspirin and other NSAIDs may be gastrointestinal upset, abdominal pain, exacerbations of ulcers and even gastrointestinal bleeding. In order to reduce the side effects of the gastrointestinal tract, NSAIDs are usually taken with meals.
Additional drugs are often recommended to protect the stomach from ulcers. These medical oral agents include antacids, sucralfate (Carafate), inhibitors (Prevacid, etc.), imizoprostol (Cytotec). The newest means - selective NSAIDs - may include inhibitors, for example celecoxib (Celebrex), which fight inflammation, but not with such a high risk of irritation of the walls of the stomach and risk of bleeding.
Corticosteroid preparations
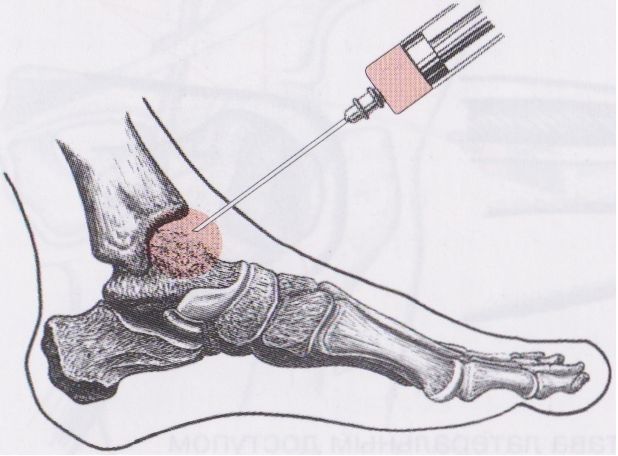
Corticosteroids can be taken orally or injected directly into tissues and joints. They are more powerful than NSAIDs in reducing inflammation and restoring the mobility of the leg joints and returning their function. Corticosteroids are useful for a short period during strong outbreaks of disease activity, or when the body does not respond to NSAIDs. However, corticosteroids can give strong side effects, especially when administered at high doses over time.
These side effects for arthritis include weight gain, facial puffiness, thinning of the skin and bones, bruising even with minor bruises, cataracts, the risk of infection, atrophy of the leg muscles and the destruction of large joints such as the hip joints. Corticosteroids (not all!) Can also give an increased risk of contracting infectious diseases. These side effects can be partially avoided, gradually reducing the dose of corticosteroids.
A sudden cessation of corticosteroids with rheumatoid arthritis can lead to bouts of illness or other symptoms - so a sharp corticosteroid withdrawal is not recommended. Thinning of bones due to osteoporosis can be prevented by taking calcium supplements and vitamin D supplements.
Preparations of the second line
"Second line" or delayed-action drugs "against rheumatoid arthritis (pain-modifying antirheumatic drugs) First-line drugs (NSAIDs and corticosteroids) can reduce joint inflammation and pain, they may not necessarily prevent joint damage and deformity.
Rheumatoid arthritis requires drugs other than those recommended by the doctor for NSAIDs and corticosteroids in order to be able to stop active damage to the bone, cartilage and adjacent soft tissues. The medicines needed for good treatment of this disease and pain in the legs associated with it are of various forms. This medication of the already mentioned "second line" or "delayed-action" means can require several months or weeks in complex treatment to influence the body effectively. They are used for a rather long period of time, even for several years, and in different doses.
The most effective drugs can promote remission, thereby slowing the progressive destruction of joints and their deformation. Sometimes all second-line drugs are used together, and this is a good combination therapy for arthritic joints in the legs. As in the first line, the doctor can try different preparations of the second line, then the treatment is optimal.
Features
Recent studies have shown that patients who respond to delayed-action medications with rheumatoid arthritis control can actually reduce the small but real risk of developing lymphoma (lymph node cancer), which sometimes worries the patient in combination with rheumatoid arthritis.
Hydroxychloroquine (plakvenil) is used to treat malaria. It has been used to treat rheumatoid arthritis for quite some time. Possible side effects of this drug include muscle weakness in the legs and hands, the occurrence of stomach disorders, skin rashes, changes in the structure of the joints of the legs.
The change in the visual function is rare, people taking this drug should apply for control to the ophthalmologist.
Sulfasalazine (Azulfidine)
It is an oral preparation that is traditionally used in the treatment of mild and moderate bowel inflammation, for example, ulcerative nonspecific colitis and Crohn's disease in the form of colitis. Sulfasalazine is also used to relieve the symptoms of rheumatoid arthritis, it needs to be done in combination with anti-inflammatory drugs. Sulfasalazine, as a rule, is well tolerated. But the side effects after taking it include a rash and upset stomach.
Since sulfasalazine is made up of sulfur-containing compounds and salicylic acid, it should be avoided for people with an allergy to sulfur-containing drugs. Methotrexate is highly popular among doctors as a drug of the second line of medicines, because it is effective and has few side effects. It also gained an advantage due to the flexibility of the dosage (they can be adjusted according to the needs of the person). Methotrexate is a remedy for immunosuppressive drugs. It can affect the condition of the bone marrow and liver, rarely causes cirrhosis of the liver. All people taking methotrexate need regular blood tests to monitor her condition and liver function.
Gold salts for the treatment of arthritis and pain in the legs
Gold salts were used to treat the symptoms of rheumatoid arthritis for many decades of the last century. Aurothiomalate sodium (water-soluble) and arothioglucose - a gold suspension - are injected, every week for several months and up to a period of several years. Auranofin as an oral drug for the treatment of rheumatoid arthritis and pain in the legs, was introduced in 1980. It is much better tolerated than previous drugs, but it affects the body a little slower.
Side effects of drugs with gold (oral and orally administered) include skin rash, oral ulcers, kidney damage with the presence of protein in the urine, as well as possible damage to the bone marrow in the presence of anemia and a low content of white blood cells in the blood. People receiving treatment with drugs with gold salts should undergo regular blood monitoring and take urine tests. Gold, taken orally, can cause diarrhea. These gold medications have lost interest in patients with arthritis due to the availability of more effective therapies.
Immunosuppressive drugs
D-penicillamine may be useful in some cases of progressive types of rheumatoid arthritis. Its side effects are similar to those that the patient receives from drugs with gold. These side effects include chills, fever, mouth ulcers, skin rashes, metallic taste in the mouth, kidney and bone marrow diseases, indigestion and joint pain, in particular, leg joints. People who take this drug need to monitor urine and blood tests. D-penicillamine can infrequently cause symptoms of other autoimmune diseases, and it is rarely recommended for curing rheumatoid arthritis.
Immunosuppressive medications are powerful drugs that suppress the work of the human immune system. Immunosuppressive drugs are successfully used to repay the symptoms of rheumatoid arthritis, in particular - with pain in the legs. These include methotrexate, as well as, azathioprine (Imuran), including cyclophosphamide (Cytoxan), and cyclosporine (Sandimmune) and chlorambucil (Leukeran). Because of serious side effects, immunosuppressive drugs (except methotrexate) are usually recommended for those who suffer from a very aggressive disease or rheumatoid inflammation with serious complications such as vasculitis - that is, inflammation of the blood vessels.
An exception is a drug such as methotrexate, which is often associated with complex side effects and its content must be checked in the blood. Methotrexate is preferred as a second-line preparation for a qualitative result.
Immunosuppressive drugs
Immunosuppressive drugs can depress the function of the bone marrow and cause anemia, as well as a low content of white blood cells in the blood, in addition. This condition is threatened by a low number of platelets. A small amount of white blood cells in the blood can increase the risk of infections in the body, while a low platelet count can increase the risk of bleeding.
The drug Methotrexate can sometimes lead to cirrhosis of the liver, as described above, and cause allergic reactions in the lungs. Cyclosporine can lead to kidney damage and increased blood pressure. Due to potentially complex side effects, immunosuppressive drugs are used in small doses, usually in combination with effective anti-inflammatory drugs.
New treatments for rheumatoid arthritis
New "second line" drugs to reduce the symptoms of rheumatoid arthritis can contain leflunomide (Arava) and tocilizumab. Each of these drugs can increase the risk of infection and the development of infections, this information should be brought to the consciousness of the patient when he takes these new second-line drugs. Leflunomide is available to alleviate the symptoms of leg pain and stop the progression of arthritis.
This is similar to blocking the effect on the body of a very important enzyme, which plays a role in the activation of the immune system. Arava can provoke hair loss, kidney, liver, diarrhea, and / or rash in some people. Do not take this medication directly during pregnancy or in front of her because of probable birth defects and avoid this medication for women who are planning a pregnancy.
Medicines that represent a new approach to curing rheumatoid arthritis are products of modern science - biotechnology. They are mentioned in the literature as biological agents or powerful modifiers of biological reaction. Compared with traditional drugs for arthritis, powerful biological medications affect the body much faster and can have a strong effect on the stage of progressive joint damage. In general, the methods of action of bio-agents are more directed, more defined with a degree of influence than traditional drugs from arthritis.
Biological preparations
Etanercept, infliximab, adalimumab are biological medications that are capable of intercepting protein agents in inflamed joints (tumor necrosis factor), which contributes to inflammation of the joints with arisen rheumatoid arthritis. These TNF-blockers are able to intercept the protein before acting on a natural receptor that can "turn on" the inflammation process. This effectively blocks inflammation provokers from inflammation of the cells.
Symptoms - pain, swelling and other symptoms that indicate an unhealthy state of the legs, can be quickly reduced in those people who use these drugs. Etanercept should be administered subcutaneously 1-2 times per week. Infliximab is an injection that is made directly into the vein (the drug is injected intravenously).
Adalimumab is administered subcutaneously once every two weeks or once every 1 week. Golimumab is administered subcutaneously every month. Certolizumab pegol is injected with a needle under the skin every 2-4 weeks. Each of these medicines is now evaluated by doctors only in practice, so that doctors can determine which of the roles these drugs can play in treating patients at different stages and in different forms of rheumatoid arthritis. Recent studies have shown that modifiers of the biological response and prevent progressive destruction of joints in rheumatoid arthritis.
 [16]
[16]
Modifiers of biological reaction
They are currently recommended to be used after second-line drugs have proved ineffective. Modifiers of biological reaction (TNF-inhibitors) are costly. They are often used in combination with methotrexate and other DMARDs. In addition, it should be noted that the blocking of TNF-biological agents is increasingly used in combination with methotrexate.
These drugs should be avoided for people with significant stagnation in the work of the heart, heart failure or demyelinating diseases (such as multiple sclerosis), as they can worsen a person's condition. Anakinra (Kineret) is another preparation of biological properties that is used for the permanent treatment of moderate and severe forms of rheumatoid arthritis.
Anakinra works by binding to the cell protein (pro-inflammatory cytokines). Anakinra is injected under the skin daily. Anakinra can be used alone or with other BVAP. The speed of anakin is not as strong as that of other biological agents.
Rituximab
Rituximab (Rituxan) are typical antibodies, they were first used to treat lymphoma, cancer of the lymph nodes. Rituximab can be effective in the treatment of autoimmune diseases, such as rheumatoid arthritis, for it depletes B cell functions that are important for killing inflammation cells and producing abnormal antibodies. Rituximab helps treat mild and active forms of rheumatoid arthritis in patients who could not benefit from the treatment of TNF-blocking biologics.
Preliminary studies have shown that rituximab has been used to benefit in the treatment of severe forms of rheumatoid arthritis, which is complicated by severe inflammation of the blood vessels (i.e., vasculitis) and cryoglobulinemia. Rituximab is used for intravenous infusion in two doses at a rate of two weeks approximately every six months.
Abatacept
Abatacept (Orencia) is a powerful biological medical product that blocks active T cells. Abatacept is used to treat adults with arthritis who are not treated with traditional BPVP drugs. Abatacept is a means for intravenous infusion over the course of a month.
Tocilizumab
Tocilizumab (Actemra) has recently been approved for the treatment of adult patients with moderately severe active rheumatoid arthritis (RA). Tocilizumab is the first approved biological preparation that is capable of blocking interleukin-6 (IL-6), which is a chemical agent of inflammation in the acute form of rheumatoid arthritis.
Tocilizumab is a drug for intravenous infusion over the course of a month. Biological preparations are often used in combination with traditional drugs in the practice of curing rheumatoid arthritis, they are usually not used with other biological agents because of the risk of serious infections that is unacceptable.
The drug Prosorba
The drug Prosorba is used to reduce or relieve symptoms of moderate to severe pain in rheumatoid arthritis in adult patients with a long-standing form of the disease, those who could not recover or tolerate anti-rheumatic pain medication (DMAP). The exact role of this method today is poorly assessed by physicians, it is not normally used at present.
Rheumatoid arthritis, pregnancy and pain in the legs
Rheumatoid arthritis often passes or reduces symptoms with the course of pregnancy. During pregnancy, rheumatoid arthritis and leg pain tend to decrease and be minimized during pregnancy. Unfortunately, this reduction in inflammation of the joints during pregnancy and pain in the legs is unstable after childbirth.
Medications that are commonly used to treat severe inflammation of the leg joints, such as non-steroidal anti-inflammatory drugs, including ibuprofen (Motrin, Advil), naproxen (Aleve), and others are not used during pregnancy. Drugs that are used to stop the progression of rheumatoid disease, such as methotrexate and cyclosporine (Neoral, Sandimmune), should not be used during pregnancy, they must be discontinued long before conception because of the potential risk to the fetus. Biological preparations for pain relief in the legs due to rheumatoid retreat are not used during pregnancy.
In rheumatoid arthritis, which is activated during pregnancy, steroid drugs such as prednisone and prednisone are often used to relieve pain in the legs to soothe the inflammation of the joints. These drugs do not have a negative effect on the fetus.
Diet and other methods of treating arthritis for pain relief in the legs
Doctors say that there is no special diet for treating manifestations of rheumatoid arthritis. A hundred years ago, such diets were advertised as a rejection of foods such as tomatoes that aggravate the manifestations of rheumatoid arthritis. This is no longer perceived as true. Fish oil was shown in advertising as a useful product in some short-term studies with rheumatoid arthritis.
The advantages of medications for eliminating simtomas of rheumatoid arthritis remain unproven. Symptomatic pain relief can often be achieved by oral acetaminophen (Tylenol) - these are topical products that are rubbed into the skin. Antibiotics, in particular, tetracycline, minocycline (Minocin), have been tested to eliminate the symptoms of rheumatoid arthritis in recent clinical trials. The first results showed that there is a slight and moderate improvement in the symptoms of arthritis.
Minocycline, it turns out, prevents the development of important enzymes - the mediators of tissue destruction, they are called metalloproteinases.
Diseases of the legs, except the tissues, which are affected by rheumatoid inflammation, are considered individually.
Exercises for joint mobility in arthritis
Properly performed regular physical exercises are extremely important for maintaining joint mobility and strengthening the muscles around the arthritic joints of the leg joints. In these conditions, the pool is particularly useful, because it allows you to perform exercises with a minimum load on the joints. Professional doctors can offer support at physical exertion for the restoration of leg joints.
For example, exercises for the mobility of the joints of the feet and toes can be useful for reducing inflammation and maintaining the alignment of the curved joints. Such devices as canes, crutches, can help in everyday life. Heat and cold on the legs alternately - conditions that can alleviate the symptoms before and after training.
Surgical intervention can be recommended to restore the mobility of leg joints or to repair damaged leg joints. Doctors who specialize in surgery for painful joints are orthopedic surgeons. Operations range from arthroscopy to partial and complete replacement of the leg joint.
Arthroscopy
Arthroscopy is a surgical technique, during which the doctor enters the tube, as an instrument in the joint, to see and eliminate deformed tissue.
Arthroscopy of the entire joint is a surgical procedure, in which the destroyed joint is replaced with artificial materials. For example, small joints of hands or feet can be replaced by plastic.
Large joints, such as thighs or knees, can be replaced with metal parts.
Psychological support
Exercises for the joints, minimizing emotional stress, can help improve the overall health of people who suffer from rheumatoid arthritis. Support and special psychological groups provide people with rheumatoid arthritis time so they can discuss their problems with others and learn more about their illness.
What is the prognosis for people with rheumatoid arthritis?
Since the beginning of an early, aggressive treatment, prospects for those affected by rheumatoid arthritis can be very good. The position of physicians regarding the possibility of fighting this disease has undergone tremendous changes since the beginning of this century. Doctors now seek to eliminate any signs of disease activity, preventing its outbreaks and seizures. Disease can be controlled and joint efforts of the doctor and the patient can lead to good results.
Patients have a less favorable prognosis when they have deformities of the joints of the legs or hands, disability, permanent uncontrolled inflammation of the joints, and / or rheumatoid diseases affecting any other organs of the body. In general, rheumatoid arthritis is usually potentially more destructive for leg joints, when rheumatoid factor or citrulline antibodies are present in the blood.
Is it possible to prevent rheumatoid arthritis and pain in the legs?
Currently, there are no specific measures to prevent rheumatoid arthritis. Because smoking, the effects of inflammatory and chronic periodontal diseases increases the risk of developing rheumatoid arthritis, these actions should be avoided.
What research is done for people with rheumatoid arthritis?
Scientists around the world are studying many promising new approaches for eliminating the symptoms of rheumatoid arthritis and leg pain. Such areas include treatment methods that block the effects of specific inflammation factors such as tumor necrosis factor (TNFalpha), B cells and T cell functions, and interleukin-1 (IL-1), as described above. Many other drugs are being developed against certain critical white blood cells involved in rheumatoid inflammation. In addition, new drugs with new mechanisms of action differ from traditional drugs.
Other methods of affecting the joints will more accurately determine which patients are prone to developing an aggressive disease such as rheumatoid arthritis. A recent study of antibodies has shown that the presence of citrulline antibodies in the blood is associated with a tendency to more destructive forms of rheumatoid arthritis.
Genetic research can bring many new opportunities for early diagnosis and accurate treatment of leg tissue in the near future. There are studies that use gene analysis to determine which patients are at greater risk and more aggressive course of the disease. All this is due to the improvement of technology. We are on the verge of huge improvements in how to manage rheumatoid arthritis.